
Abstract
Objective
The objective of this study was to compare the outcomes of endoscopic cartilage myringoplasty (ECM) with or without plasma radiofrequency (RF) tuboplasty (PRT) for repairing chronic large perforation with Eustachian tube dysfunction (ETD).
Materials and methods
Chronic large perforations with ETD were randomly divided into receiving ECM or ECM plus PRT. During the 24 months follow-up, the Eustachian tube score (ETS), Eustachian Tube Dysfunction Questionnaire-7 (ETDQ-7), ET inflammation scale, hearing results, and graft success rate of the patients were analyzed.
Results
A total of 61 subjects were included in the study. Difference of ETS was significant before and after surgery in the ECM + PRT group (P < .05) but the ECM group was not (P > .05). Also, significant between-group difference was found regardless of post-24 months ETS and improvement value. Postoperative ETDQ-7 scores were significantly reduced compared with preoperative ETDQ-7 scores in both groups (P < .05), also, significant between-group difference was found regardless of post-24 months ETDQ-7 scores and improvement value. The graft success rate was 86.7% in the ECM group and 96.8% in the ECM + PRT group at postoperative 24 months (P > .05). In addition, although the ECM + PRT group showed a better air-bone gap improvement than the ECM group, the difference was not significant (13.01 ± 2.97 vs 10.92 ± 0.69 dB; P > .05). No PRT procedure-related serious adverse events were reported during the follow-up process. No patients developed atelectasis or otitis media with effusion in either group.
Conclusion
ECM combined with low-temperature PRT did not affect the graft success rate but showed a better long-term improvement in ETS and ETDQ-7 than cartilage myringoplasty for the treatment of chronic perforation with ETD. In addition, although PRT showed a better hearing improvement, the difference was not significant between the 2 groups.

Introduction
Although the conventional belief is that obstructive Eustachian tube (ET) dysfunction (ETD) may have an adverse impact on the outcomes of tympanoplasty, there is still no consensus that ETD is a decisive factor in the outcome of tympanoplasty.1-3 Because balloon Eustachian tuboplasty (BET) is commonly-used technique for ETD in recent years, some authors suggested BET combined with tympanoplasty to improve the outcome of tympanoplasty for the patients with ETD.1,4,5 Nevertheless, these studies showed conflicting results.1,4,5 Previous studies have identified the cartilaginous portion of the ET as the most frequent site of dysfunction,6-8 while some recent scholars believed that the hypertrophic tissue from the ET orifice is the most common pathogenesis of ETD.9-11
Previously, CO2 laser tuboplasty or microdebrider tuboplasty has been reported to remove the hypertrophic tissue of the ET orifice, thereby improving the ET function,7-9 but there were no consecutive studies due to pain during healing period. The excessive heat penetration generated by laser can accelerate organizational structure damage, local inflammation response, and the formation of scar tissue, contributing to intensified pain. 12 On the contrary, low-temperature plasma radiofrequency ablation (RFA) is a radiofrequency (RF) method of tissue destruction, RF technique works at 60°C, the produced thermal damage to surrounding tissues is much smaller than that caused by laser, with a minimized inflammatory response and pain sensation as well as a contracted healing time. 12
The use of RFA has become increasingly widespread in otolaryngology in recent years. Some studies suggested that postoperative pain scores after RFA were significantly lower than those after laser intervention, but RFA was significantly better than CO2 laser ablation in postoperative mucosal recovery.13,14 A study showed complete epithelialization by postoperative day 7 following RFA but postoperative day 14 following CO2 laser. 15 Also, compared with microdebrider’s mechanical injury, RFA may cause less inflammation. 16 In addition, the plasma knife head can be bent to a narrow space and cut off the hypertrophic tissue that is difficult to be handled by the linear beam of CO2 laser. 12
Recently, plasma radiofrequency ablation tuboplasty (PRT) has been used to treat chronic otitis media with effusion with ETD and obtain the satisfactory effects.10,11 However, to date, there have been no reports of tuboplasty combined with tympanoplasty on the chronic perforation with ETD. The objective of this study was to compare the postoperative outcomes of endoscopic cartilage myringoplasty (ECM) with or without RF ablation (RFA) tuboplasty for the treatment of chronic perforation with ETD.
Materials and Methods
Ethical Considerations
The study was conducted in accordance with the ethical standards stated in the “Declaration of Helsinki.” The study was approved by Medical Ethical Committee of Wenzhou medical university affiliated yiwu hospital (protocol number: K2020-IBR-027). Informed consent was obtained from all participants.
Patient Selection
Consecutive adult patients diagnosed with chronic large perforations with obstructive ETD were enrolled in the study. Inclusion criteria were 16 years old and above, large perforations with 1/4 to 1/2 of the tympanic membrane (TM), dry ears for >3 months, good pneumatization of the mastoid, a diagnosis of obstructive ETD for at least 3 months, and ET inflammation scale more than 2. Exclusion criteria were revision surgery, adhesive perforation, cholesteatoma, acute infection, poor pneumatization of the mastoid, ossicular chain abnormalities, preoperative air-bone gap (ABG) above 40 dB, fungal otitis externa, the obstruction of the ET in bony parts, and nasal or nasopharyngeal manifestations (as allergic rhinitis, chronic sinusitis). Prior to enrollment, all patients received a high-resolution thin-slice computed tomography scan of the temporal bone, audiograms, endoscope, ET inflammation scale, and Eustachian tube function (ETF) evaluation before surgery. The perforation site was classified as anterior, posterior, or inferior by reference to the position of the malleus handle. Diagnosis of obstructive ETD was based on a total Eustachian Tube Dysfunction Questionnaire-7 (ETDQ-7) score higher than 14.5 17 and Eustachian tube score (ETS) ≤5.2,18,19
Patients were randomly allocated to the 2 groups using a block randomization method. Group allocation was performed using a sealed envelope approach; patients were allocated to an ECM or ECM + PRT.
ETDQ-7 Assessment
The ETDQ-7 is a validated, standardized, 7-item self-report questionnaire to assess ETD symptom severity. The questionnaire is not specific to the affected ear(s). Each item is assessed on a scale of 1 (no problem) to 7 (severe problem), and an overall score, which is the mean of the scores for the 7 items, is calculated. Scores in the range of 1 to 2 indicate no-to-mild symptoms, scores of 3 to 5 indicate moderate symptoms, and scores of 6 to 7 indicate severe symptoms. ETD was suggested by a total ETDQ-7 score of greater than 14.5. 17
ETS Assessment
ETS includes the objective measurement of Tubomanometry (TMM) and the subjective measurement of Valsalva and Toynbee maneuvers. TMM is determined by using the sensor at the closed external ear to detect the pressure change in the middle ear. 18 When swallowing, 3 specific pressures (ie, 30, 40, and 50 mbar) are applied to the nasopharynx. The system can automatically calculate the ET opening index or R-value, which reflects the time between pressure application in the nasopharynx and measurement of a pressure change in the external auditory canal (EAC). An immediate opening of the ET (R < 1) is weighted with 2 points, a delayed opening (R > 1) yields 1 point, and no opening (negative or no measurable R) yields 0. A positive Toynbee’s clicking sound when swallowing and a positive Valsalva’s maneuver are rated 0 for “never,” 1 point for “sometimes,” and 2 points for “always.” The patient’s specifications should be related to at least the previous 2 months. The final ETS is the sum of the scores of the 5 items, ranging from 0 to 10. 18
ET Inflammation Scale
The ET inflammation scale assesses mucosal inflammation within the nasopharyngeal orifice and lumen, as well as ET function, as follows: grade 1—normal mucosa and normal dilation; grade 2—mildly-inflamed mucosa, no apparent impairment of dilation; grade 3—moderately-inflamed mucosa, some impairment of dilation; and grade 4—severely-inflamed mucosa, unable to dilate.10,11
Audiometric Measurements
Audiometric data were assessed preoperatively and at 24 months postoperatively. Pure-tone averages were calculated for both air conduction (AC) and bone conduction (BC) by averaging the thresholds at 500, 1000, 2000, and 3000 Hz; in most cases, a threshold of 4000 Hz was used to interpolate the threshold of 3000 Hz per the standards of the Hearing Committee of the American Academy of Otolaryngology—Head and Neck Surgery. The ABG was calculated by subtracting AC from BC thresholds. ABG closure was defined as the difference between the preoperative and postoperative ABG.
Surgical Approach
All operations were performed by the same surgeon. All the patients underwent endoscopic cartilage-perichondrium underlay myringoplasty, which does not involve raising a tympanomeatal flap and trimming perforation margins.
A single-layer perichondrium-cartilage composite graft was harvested from the ipsilateral tragus. The graft in both groups was supported medially and laterally by biodegradable NasoPore (Stryker Canada, Hamilton, ON, Canada). The tragus incision was not sutured. Rather, pressure was applied using gauze soaked with erythromycin ointment.
The epithelium was removed from the distal malleus handle if any. The lateral perichondrium was elevated circumferentially around the cartilage graft, with attachment of the cartilage graft. Cartilage was trimmed based on the perforation size and type, with the graft being ≥1 mm larger than the perforation margins. A notch was created in the cartilage graft to accommodate the malleus handle, if necessary. The perichondrial graft, which should be 2 mm larger than the cartilage graft, was also trimmed peripherally.
Endoscopic Cartilage Myringoplasty
The cartilage graft was placed trans-perforation medial to the remnant TM and the annulus, with a notch in the cartilage accommodating the malleus handle if necessary. The perichondrium graft was also placed trans-perforation medial to the remnant TM and the annulus but lateral to the cartilage (and malleus handle) (Figure 1).

Surgical procedure of the ECM + PRT group. Cartilage myringoplasty. (A) Middle ear packing. (B) Graft placement. (C) Graft end. RF ablation tuboplasty. (A) Lateral outfracture of the inferior turbinate. (B) Inferior ablation turbinectomy. (C) RF ablation of the ET orifice. ECM, endoscopic cartilage myringoplasty; ET, Eustachian tube; PRT, plasma radiofrequency tuboplasty; RF, radiofrequency.
Endoscopic Cartilage Myringoplasty + Plasma Radiofrequency Tuboplasty
In this group, PRT was firstly performed on the operated side before ECM. PRT technique had been described by a previous study. 11
The RF coblation system was marketed by China Micro Medical Limited Shanghai Micro Medical Devices Co, Ltd (Shanghai, China); the Evac 70 Plasma Wand was preferred. During the entire process, the Evac 70 Wand was set at an ablation power of 7 and a coagulation power of 3. The Coblation system was introduced by 0° or 45° endoscope via the ipsilateral nasal passage. Patients underwent PRT targeting hypertrophic tissue of the ET orifice 11 (Figure 1). No nasal packing was applied after RFA.
Postoperative Follow-Up
Patients were discharged on the day after surgery. The packing gauze was removed in postoperative week 1, and biodegradable synthetic polyurethane foam was aspirated from the EAC in postoperative week 2, which allowed the graft and the ET orifice to be visualized endoscopically. Postoperative follow-up was scheduled at 1st, 2nd, and 4th week and at 3rd, 6th, 12th, and 24th month. The patients were asked about altered taste, vertigo, and tinnitus at each follow-up examination. The graft success, audiometric outcome, ET inflammation scale, ETS, and ETDQ-7 improvement were evaluated at postoperative 24th month. Graft success was defined as the presence of an intact graft without residual or re-perforation. Residual perforation was defined as the presence of perforation within 3 months after surgery, while re-perforation defined as the presence of perforation during 4 to 24 months after surgery.
Statistical Analyses
Descriptive statistics were presented as means and standard deviations, and categorical variables were presented as counts and percentages. The Chi-squared (χ2) test was performed to compare categorical variables between groups. The postoperative ABG gains, ETS improvements, ETDQ-7 improvements, average pure tone levels, and the values of the variables were analyzed using the Mann-Whitney U test. All statistical analyses were performed using SPSS (version 20; IBM Corp, Armonk, NY, USA). The criterion for statistical significance was set at P < .05.
Results
Demographic Characteristics
A total of 61 subjects were included in the study. Demographic data for the ECM and ECM + PRT groups are shown in Table 1. The variables such as sex, age, perforation side, position, duration, myringosclerosis, diabetes, and smoking status showed no significant between-group differences before surgery. In addition, we did not find the patients with granulation blocked a tympanic orifice in either group. All the patients completed 24 months follow-up.
Demographic Characteristics of Patients.

Abbreviations: ECM, endoscopic cartilage myringoplasty; F, female; L, left; M, male; PRT, plasma radiofrequency tuboplasty; R, right.
Chi-square test.
Mann-Whitney U test.
ET Inflammation Scale and Wound Healing Process Time of the Orifice of ET
Endoscopic findings showed no significant between-group difference for preoperative ET inflammation scale in nasopharyngeal orifice of ET. However, there was a significant improvement after surgery compared with before surgery for ET inflammation scale in either group. In addition, the postoperative grade 1 in the ECM + PRT group was significantly higher than in the ECM group (P = .028), although no significant between-group difference was found in the postoperative total grade 1 and grade 2 (P = .235) (Table 2).
The ETS, ETDQ-7, Graft Success Rate, and Complications.

P1, comparison among groups; P2, comparison of before and after surgery.
Abbreviations: ECM, endoscopic cartilage myringoplasty; ET, Eustachian tube; ETDQ-7, Eustachian Tube Dysfunction Questionnaire-7; ETS, Eustachian tube score; PRT, plasma radiofrequency tuboplasty.
Mann-Whitney U test.
Chi-squared test.
Of the 31 patients in the ECM + PRT group, complete wound healing of the orifice of ET was achieved in 13 (41.9%) patients at postoperative 1 week, at postoperative 2 weeks in 15 (48.4%) patients, and 4 weeks in 3 (9.7%) patients. In addition, endoscopic examination showed a thickened gray-white pseudomembrane on the posterior wall and posterior cushion of the ET orifice within 3 days after surgery, which disappeared gradually over time. At postoperative weeks 1 and 2, the pseudomembrane completely disappeared, and hyperplastic mucosa of the ET orifice is apparently reduced.
Eustachian Tube Score
No significant difference was found between the 2 groups at preoperative ETS. The postoperative ETS was higher than preoperative ETS in both groups; however, the difference was significant before and after surgery in the ECM + PRT group (P < .05), but the ECM group was not (P > .05). Also, significant between-group difference was found regardless of post-24 months ETS and improvement value (Table 2).
Eustachian Tube Dysfunction Questionnaire-7
No significant difference was found between the 2 groups at preoperative ETDQ-7 scores; however, the postoperative ETDQ-7 scores were significantly reduced compared with preoperative ETDQ-7 scores in both groups (P < .05); also, significant between-group difference was found regardless of post-24 months ETDQ-7 scores and improvement value (Table 2).
Graft Take
Table 2 summarizes the graft success rate. The residual perforation was seen in only 1 (3.2%) patient in the ECM + PRT group, the difference was not significant (P > .05). Nevertheless, re-perforation occurred in 13.3% patients in the ECM group and in 3.2% patients in the ECM + PRT group (Figure 2), and the difference was not significant (P > .05). The graft success rate was 86.7% in the ECM group and 96.8% in the ECM + PRT group at postoperative 24th month, and the difference was not significant (P > .05). Figure 3 shows the healing process of graft in the ECM + PRT group.

Surgical and healing procedure of the ECM + PRT group. (A) Postoperative perforation. (B) Graft placement. (C) Postoperative 4 weeks. (D) 8 weeks. (E) Re-perforation at 36th month. (F) Postoperative ET orifice, ET inflammation scale grade 4. (G) Inferior ablation turbinectomy. (H) RF ablation of the ET orifice. (I) ET inflammation scale grade 1. ECM, endoscopic cartilage myringoplasty; ET, Eustachian tube; PRT, plasma radiofrequency tuboplasty; RF, radiofrequency.
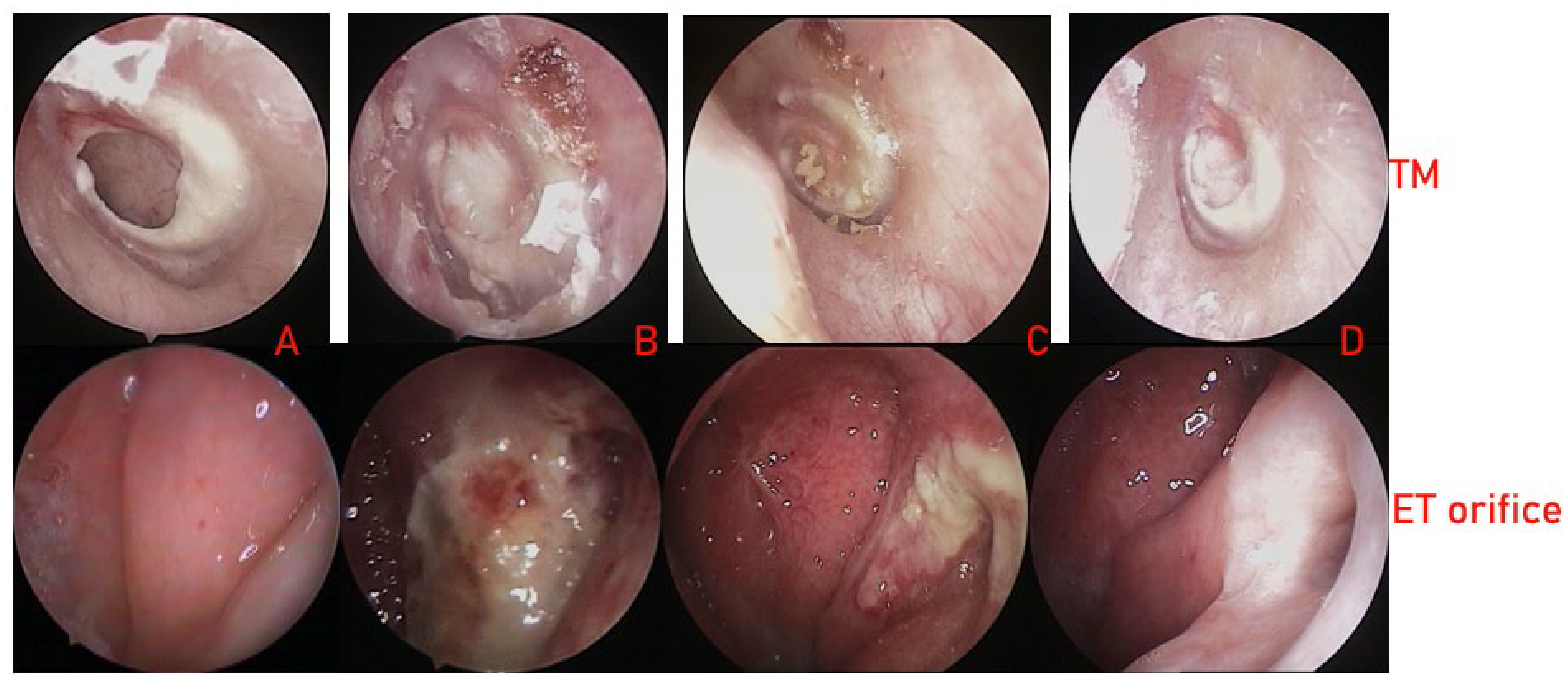
The healing process of the ECM + PRT group. TM healing. (A) Postoperative perforation and ET orifice (Grade 4), (B) postoperative 2 weeks, (C) 4 weeks, (D) 36 months, ET orifice (Grade 1). Figures 1 and 3 are the images of the same patients. ECM, endoscopic cartilage myringoplasty; ET, Eustachian tube; PRT, plasma radiofrequency tuboplasty; TM, tympanic membrane.
Hearing Outcome
Table 3 summarizes the hearing outcomes. No significant between-group difference was found regardless of pre- or postoperative AC, pre- or postoperative BC, pre- or postoperative ABG value or ABG improvement.
Comparison between Hearing Gains, the ABG, and BC.
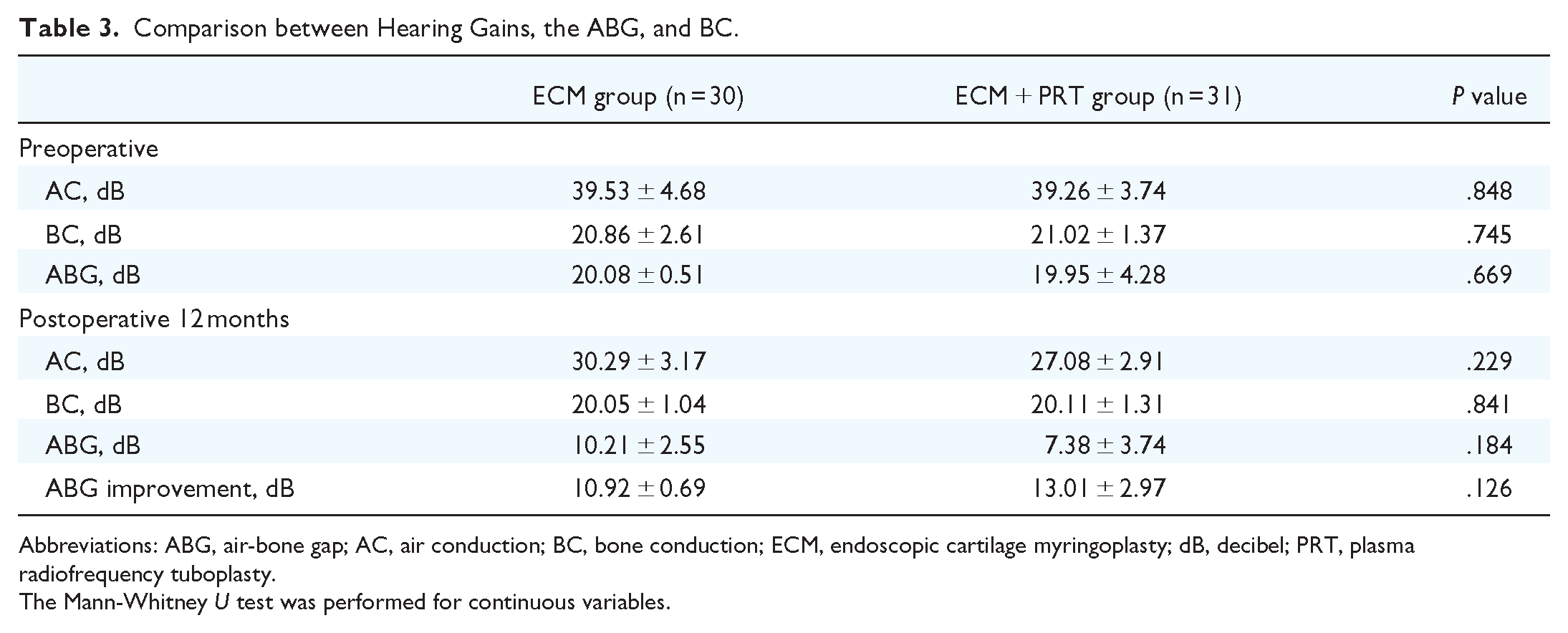
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction; ECM, endoscopic cartilage myringoplasty; dB, decibel; PRT, plasma radiofrequency tuboplasty.
The Mann-Whitney U test was performed for continuous variables.
In addition, although the ECM + PRT group showed a better ABG improvement than the ECM group, the difference was not significant (13.01 ± 2.97 vs 10.92 ± 0.69 dB; P > .05).
Complications
There were no cases of graft medialization, graft lateralization, or significant blunting in either group. None of the patients reported sensorineural hearing loss, vertigo, or intractable tinnitus during the follow-up process. No RFA procedure-related serious adverse events were reported, including stenosis and/or synechia of the orifice of ET, and nasal and oral hemorrhage in the ECM + PRT group; also, no patients reported pharyngalgia, and no patients developed symptoms of patulous ET in the ECM + PRT group. No patients developed atelectasis or otitis media with effusion in either group.
Discussion
This study showed that postoperative ET inflammation scale grades 1 and 2 in the ECM + PRT group had significantly improved compared with preoperative scales. This results further demonstrated in a previous study. RFA can ablate hypertrophic tissue in the ET orifice, which causes minimal inflammation and a lower infection rate compared with laser or microdebrider tuboplasty.12,16 In this study, no patients reported postoperative pharyngalgia. A total of 41.9% patients showed complete wound healing of the orifice of ET at postoperative 1 week and 48.4% at postoperative 2 weeks. An animal study has shown rapid regeneration of respiratory epithelium following RFA compared with laser ablation. 16 However, grade 1 was seen at postoperative 24 months in the ECM group, and the number of grade 2 had improved than before surgery, although the improvement was not significant. This results revealed that myringoplasty could improve the ET function in some patients with ETD. This may explain why aural fullness disappeared after tympanoplasty in some patients with chronic perforation. The reason may be that normal physiological functions in the mastoid, ET, and middle ear ventilation system was recovered, thereby reducing the mucosa edema of ET.
Although ETS had an improvement before and after surgery in either group, the difference was significant in the ECM + PRT group in this study. Similar improvement also occurred in the ETDQ-7 score. This results suggested that ECM + PRT group had better recovery of middle ear function and subjective symptom improvement, which agreed with a previous study. Previous studies suggested that RFA tuboplasty significantly improved the ETDQ-7 scores and Valsalva maneuver for the patients with ETD.10,11 In addition, it is well known that the opening of ET is not the only factor affecting middle ear ventilation. The middle ear balance system is also affected by the volumes of mastoid and tympanic cavity, the air-containing middle ear cavity, and mucosal dispersion.2,20 Li et al 2 believed that tympanoplasty can relieve intratympanic inflammation by reconstructing TM, improve the middle ear pressure balance system, and recover the ET function. Si et al 5 reported that ETS was not improved after ECM alone for the adhesive otitis media. In their study, adhesive otitis media not only had ETD but also abnormal gas exchange between middle ear and mastoid resulting from edema and fibrosis of mucous because of long-term effusion. 5 However, in our study, these patients had dry ear at least 3 months and well pneumatization of the mastoid and middle ear. We did not find the patients with granulation blocked a tympanic orifice in either group. Thus, these patients had good gas exchange function of middle ear and mastoid.
Although the ECM group had high re-perforation, the difference in graft success rate was not significant between the 2 groups. This result suggested that ETD did not affect the graft success rate of cartilage myringoplasty. Previous studies also proved that ETD affected the graft success rate of temporalis fascia, but cartilage myringoplasty did not.2,21 Cartilage is a stiff materials, which can better resist negative middle ear pressure for a long time.5,22,23 On the other hand, the graft success rate depends more on the function of middle ear and mastoid ventilation.2,20,24 Takahashi et al 20 suggested that impairment of all the middle-ear pressure-regulation functions was likely to cause poor outcome of tympanoplasty, and not all the ears on which all the functions were poor had poor postoperative outcome.
Tympanoplasty could be performed when at least one of aeration of the mastoid and ET functions is good. Another possibility is that the patients who were identified as poor ET function before surgery, the integrity of the middle ear was restored after myringoplasty, thus improving the ET function, and this may be enough for the middle-ear pressure-regulation function. 20 Si et al 5 compared the cartilage myringoplasty and BET plus cartilage myringoplasty and obtained similar graft success rate (93.3% vs 96.7%) at postoperative 2nd year.
There were significant differences in hearing improvement in either group before and after surgery, while the ECM + PRT group showed better hearing recovery. These results revealed that PRT may further improve ETF and lead to a better hearing outcome following tympanoplasty. Nevertheless, the differences in the hearing improvement was not significant between the 2 groups. This result was similar with a previous study.
Si et al 5 found that the difference in postoperative hearing improvement was not statistically significant between the cartilage and BET + cartilage groups. This implies that cartilage tympanoplasty plays a key role in the hearing recovery for the patients with the patients with normal ossicular chain and good pneumatization of the mastoid and middle ear, RFA could not address the problem of irreversible mechanical vibration in the TM and middle ear acoustic structures. On the contrary, Hsieh et al 1 found that the ABG improvement in the BET + tympanomastoidectomy group was significantly better than that of the tympanomastoidectomy alone group, while this difference was not statistically significant between the 2 groups for postoperative ABG of 20. This may be explained by the difference in the study participants and graft material between our and their studies. Cartilage graft was applied in our and Si et al 5 ’s studies, but the fascia graft and mastoidectomy were in Hsieh et al 1 ’s study. The fascia or perichondrium graft is superior to the cartilage-perichondrium graft in terms of auditory-mechanical vibration.25,26
No patients developed atelectasis or otitis media with effusion in either group. In addition, no RFA procedure-related serious adverse events were reported in the ECM + PRT group. Also, no nasal packing was applied because the plasma cutter head used in RFA has the functions of ablation, cutting, and hemostasis, no postoperative nasal and oral hemorrhage were seen. However, the limitation of this study was small sample size and a single institutional study, large sample size, and multi-center study should be considered in the future.
Conclusion
ECM combined with low-temperature PRT did not affect the graft success rate but showed a better improvement in ETS and ETDQ-7 than cartilage myringoplasty for the treatment of chronic perforation with ETD. In addition, although PRT showed a better hearing improvement, the difference was not significant between the 2 groups.
Footnotes
Acknowledgements
None.
Author Contributions
Zhengcai Lou: Interpretation of data for the work, design of the work, analysis of data for the work, drafting the work, agreement to be accountable for all aspects of the work; final approval of the version to be published; Zihan Lou: Interpretation of data for the work, analysis of data for the work, drafting the work and technical the diagram, agreement to be accountable for all aspects of the work, and final approval of the version to be published; Tian Lv: Analysis of data for the work; agreement to be accountable for all aspects of the work; and Zhengnong Chen: Interpretation of data for the work, design of the work, final approval of the version to be published.
Availability of Data and Materials
The datasets supporting the conclusions of this article are included within the article.
Consent for Publication
Informed patient consent was obtained in writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shanghai Medical innovation project, China (Grants # 22Y11902100), Technology Agency of Jinhua City, China (Grants # 2022-3-042).
Ethics Approval and Consent to Participate
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Yiwu Central Hospital in Yiwu, Zhejiang, China. Informed consent was obtained from all participants.