
Abstract
Objectives:
This study was performed to evaluate the significance of intraoperative preservation of the internal branch of the superior laryngeal nerve (ibSLN) during surgery for hypopharyngeal squamous cell carcinoma (HSCC).
Methods:
Twelve patients with HSCC underwent surgery between January 2017 and December 2018. Sensation in the hypopharyngeal mucosa was tested using a flexible laryngeal endoscope on postoperative day 5.
Results:
Surgeries were successfully performed in 10 patients with HSCC arising from the internal wall of the pyriform fossa and in 2 patients with HSCC arising from the posterior wall of the hypopharynx. The main trunk of the ibSLN was preserved in all patients. Testing of sensation in the hypopharyngeal mucosa revealed the presence of the cough reflex in all patients. All patients achieved a full normal oral diet at a median of 8.5 days (range, 6-11 days) and removal of the tracheal tube at a median of 10 days (range, 7-12 days).
Conclusions:
Our results showed that preservation of the ibSLN during surgery for HSCC is feasible and important in the recovery of sensation in the hypopharyngeal mucosa.
Keywords
Introduction
Head and neck cancer is the sixth most common type of cancer worldwide. Squamous cell carcinoma (SCC), arising from 3 anatomical regions of the hypopharynx, including the pyriform fossae, posterior wall of the hypopharynx, and posterior region of the cricoid mucosa, accounts for approximately 8% of all head and neck cancers.1,2 Approximately 20% to 30% of these patients have early-stage disease (stages I and II) at the time of diagnosis, and the 5-year overall survival rate is approximately 45%. 3
The treatment of hypopharyngeal SCC (HSCC) depends on the clinical stage. The protocol of induction chemotherapy with consequent (chemo)radiotherapy or surgery is usually recommended for patients with late-stage disease, whereas surgery or definitive radiotherapy is suggested for patients with early-stage disease. 3
Rapid recovery of swallowing function has attracted increasing attention in recent years with respect to the functional outcomes, which may impact the postoperative quality of life of patients with early-stage HSCC. During the initial postoperative period, enteral nutrition is administered to patients through a nasogastric tube, and oral alimentation is adopted when the swallowing function has recovered. One of the most important factors that impacts the swallowing function is hypoesthesia of the hypopharyngeal and laryngeal mucosa caused by impairment of the internal branch of the superior laryngeal nerve (ibSLN). 4 The ibSLN, arising from the vagus at the nodose ganglion, splits into branches before or after traversing the thyrohyoid membrane (Figure 1) and then distributes to the mucosa of the laryngeal vestibule and pyriform fossae. Injury to the ibSLN results in a loss of sensation in the innervated area, leading to aspiration pneumonia or even cardiopulmonary failure.4,5 Hence, intraoperative preservation of the ibSLN may be important for the recovery of sensation in the hypopharyngeal mucosa after surgery for HSCC.
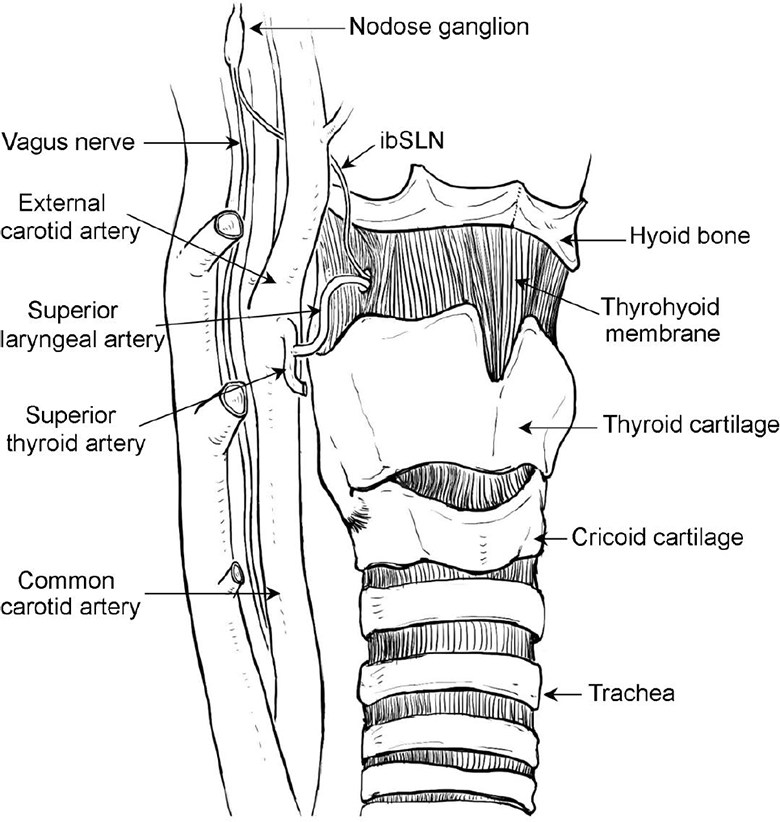
Relationship of the internal branch of the superior laryngeal nerve (ibSLN) to important branches of the carotid artery and laryngeal skeleton. The ibSLN, arising from the vagus at the nodose ganglion, traverses the thyrohyoid membrane along with the superior laryngeal artery arising from the superior thyroid artery.
In the present study, we evaluated the significance of intraoperative preservation of the ibSLN in the recovery of sensation in the hypopharyngeal mucosa and in the achievement of a full normal oral diet after surgery for HSCC.
Patients and Methods
Design of the Study
The present study was designed to evaluate the significance of intraoperative preservation of the ibSLN in the recovery of sensation in the hypopharyngeal mucosa during surgery for HSCC. Sensation in the hypopharyngeal mucosa was tested using a flexible laryngeal endoscope. The times of achievement of a full normal oral diet and removal of the tracheal tube after the surgery were also calculated.
Patients
Treatments for patients with primary HSCC in our hospital include definitive radiotherapy, induction chemotherapy, concurrent systemic therapy/radiotherapy, and surgery according to the National Comprehensive Cancer Network Guideline Version 2, 2016 (Cancer of the hypopharynx). Treatments for HSCC of different tumor-node stages were explained carefully to all the patients and their families to help the patients make the treatment decision. Between January 2017 and December 2018, 12 patients with T1-2N0-1M0 primary HSCC who selected surgery as their primary treatment were enrolled in the present study. The main clinical and pathological characteristics of the patients are presented in Table 1. Clinical staging of the tumors was assessed according to the sth edition of the Union for International Cancer Control (UICC 2008) tumor–node–metastasis classification of malignant tumors.
Main Clinical, Pathologic Characteristics, Therapy, and Follow up of Patients with Hypopharyngeal SCC.
Abbreviation: SCC, squamous cell carcinoma.
Review of the ibSLN
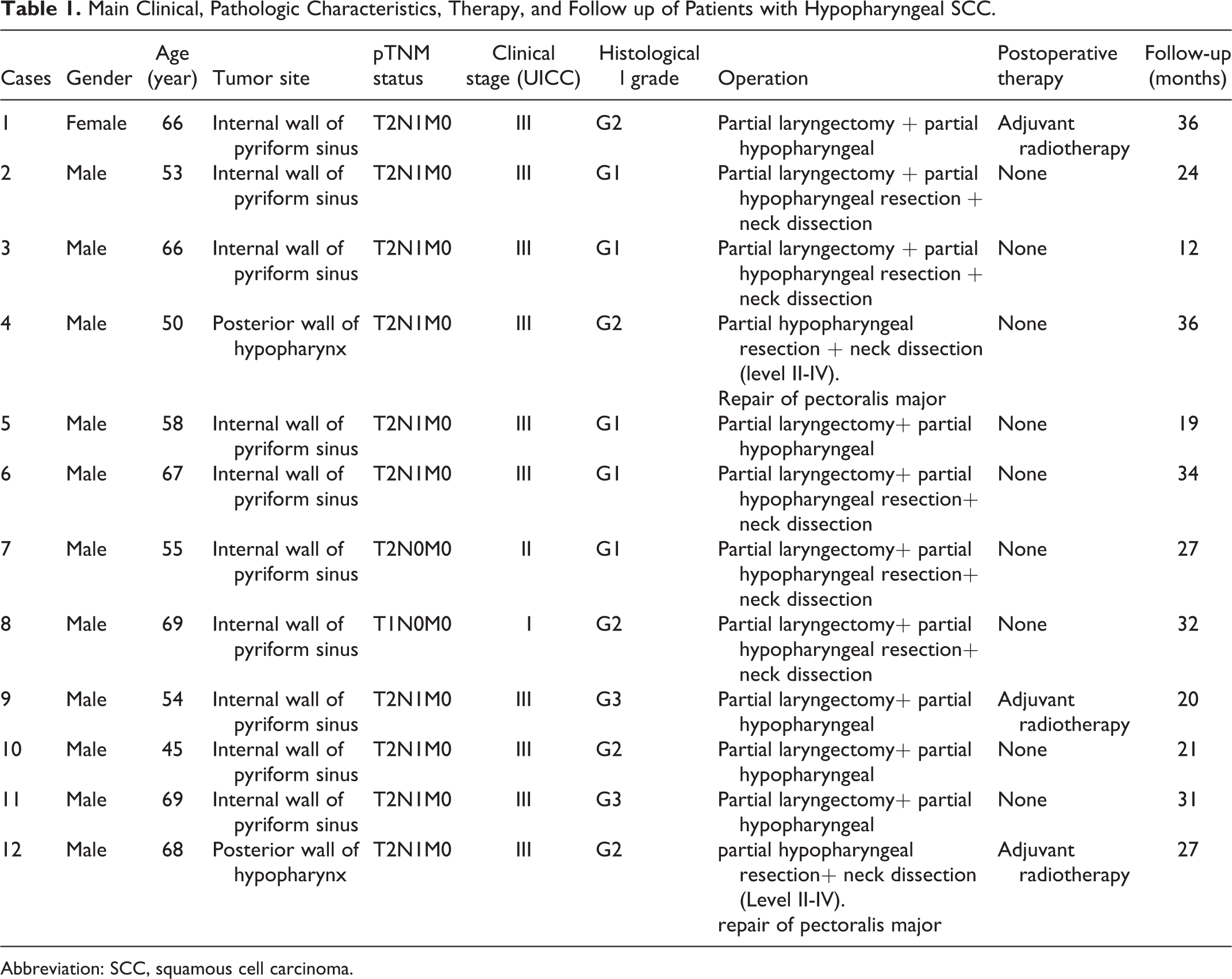
The PubMed database (http://www.ncbi.nlm.nih.gov/pubmed) was queried for “internal branch of superior laryngeal nerve” in the English language. Relevant articles retrieved through this search were reviewed, and the distribution of the ibSLN is shown in Figure 2.
Distribution of the 3 branches of the internal branch of the superior laryngeal nerve (ibSLN). The ibSLN subdivides into 3 branches. The superior branch (I) runs to the lingual part of the epiglottis and sends small fibers through the epiglottic foramina to the laryngeal surface. The middle branch (II) runs through the mucosa of the vestibule of the larynx, quadrangular membrane, and vestibular folds. The inferior branch (III) distributes to the mucosa of the pyriform recess and postcricoid region.
Technical Description
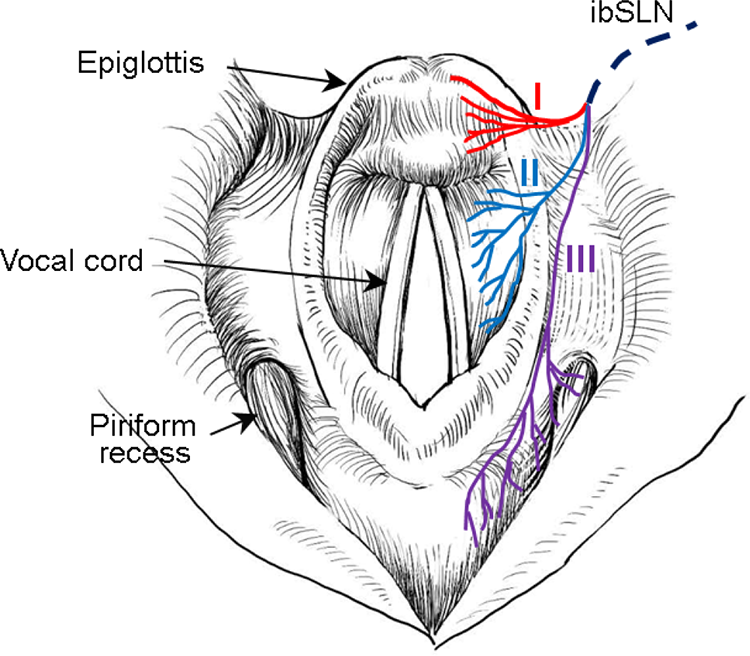
Computed tomography (CT) angiography of the neck was performed preoperatively. A transcervical incision was made. The soft tissue of the neck was elevated, and the common carotid artery, external carotid artery, and superior thyroid artery were consecutively dissected. The superior laryngeal artery was identified and separated from the superior thyroid artery. The ibSLN was dissected along the superior laryngeal artery (Figure 3). The posterior upper part of the thyroid cartilage of the tumor side was excised, and a trans-hypopharyngeal approach to the hypopharyngeal cavity was then implemented (Figure 4). The tumor with wide safety margins was then resected en bloc under direct vision or combined with endoscopy vision (Figure 5). Bipolar cautery was used for hemostasis. After all resection margins were confirmed to be negative based on intraoperative frozen pathology, the wound was closed using subcuticular 4-0 Dexon sutures, and a small Hemovac tube was placed for drainage. Finally, all specimens were sent for paraffin sectioning for final histological examination.
Intraoperative photograph demonstrating the internal branch of the superior laryngeal nerve (ibSLN) immediately before partial laryngectomy. The ibSLN was found to traverse the thyrohyoid membrane along with the superior laryngeal artery (SLA) after consecutive dissection of the common carotid artery (CCA) and superior thyroid artery (STA).
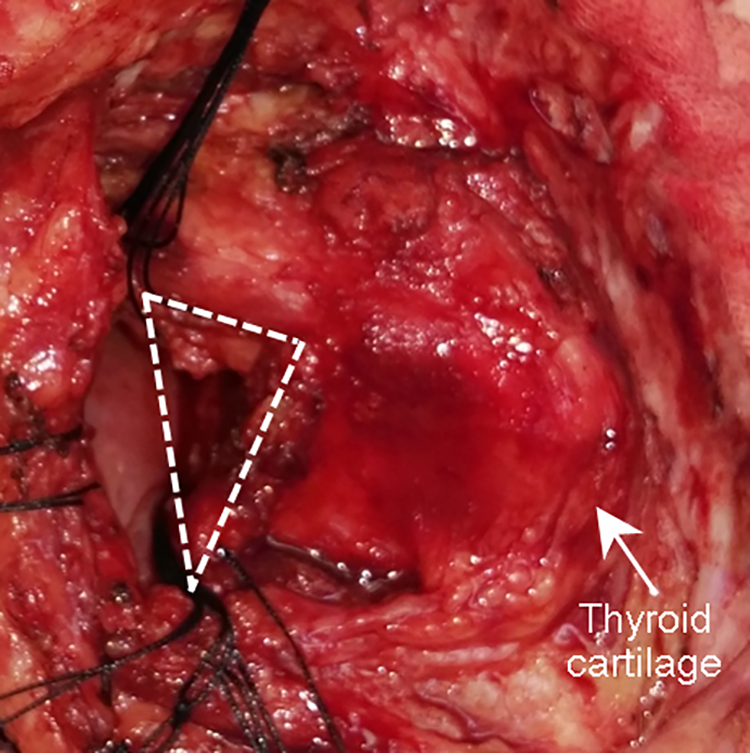
Intraoperative photograph demonstrating a trans-hypopharyngeal approach to the tumor-side hypopharyngeal cavity after excision of the posterior upper part of the thyroid cartilage (area within white dotted triangle).
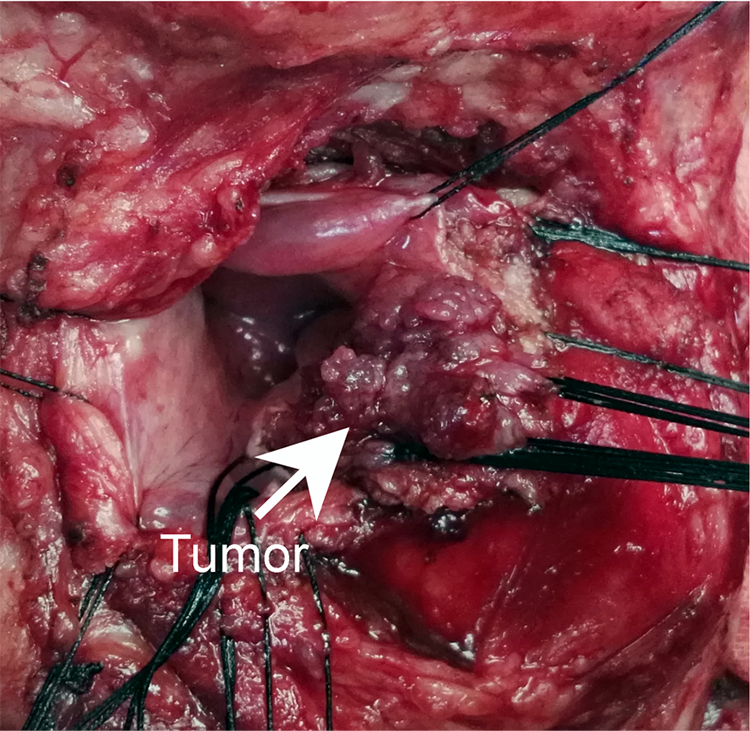
Intraoperative photograph demonstrating partial laryngectomy performed under direct vision.
Ethical Considerations
Before enrollment, informed consent was obtained from all participants. This study was approved by the ethics committee of the First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Results
All 12 surgeries were successfully performed. The tumors were resected en bloc with wide safety margins. Postoperative pathological examination confirmed that the margins were negative. The main trunk of the ibSLN was preserved in all patients during the surgery. In 2 patients, the ibSLN split into branches before traversing the thyrohyoid membrane.
On postoperative day 5, sensation in the hypopharyngeal mucosa was tested using a flexible laryngeal endoscope. All patients coughed when the endoscope tip touched the mucosa of the arytenoid, epiglottis, and pyriform fossae, indicating that the cough reflex was present.
All patients commenced an oral soft diet at a median of 7 (range, 5-9 days) days after the surgery. All patients achieved a full normal oral diet at a median of 8.5 (range, 6-11 days) days and removal of the tracheal tube at a median of 10 (range, 7-12 days) days. Complete head and neck examination, electronic laryngoscope examination, and imaging (CT or magnetic resonance imaging [MRI]) were performed during the follow-up. In detail, the complete head and neck and electronic laryngoscope examinations were performed as follows: year 1, every 1 to 3 months; year 2, every 2 to 6 months; years 3 to 5, every 4 to 8 months; and >5 years, every 12 months. Moreover, CT or MRI were performed as follows: year 1, every 3 to 6 months; and >year 1, every 6 to 12 months. All patients were judged to be disease-free during a follow-up at a median of 27 months (range, 12-36 months).
Discussion
Many studies to date have been conducted to investigate the recovery of swallowing function after chemoradiotherapy and reconstruction of the hypopharynx in patients with late-stage HSCC.6-13 The posttreatment swallowing function is usually influenced by edema and stricture of the transferred free flaps, such as jejunal, ileocolic, and gastro-omental free flaps. However, few studies have focused on the rapid recovery of the swallowing function in patients with HSCC. Free flaps are less frequently used during surgery for HSCC; therefore, dysphagia caused by stricture of free flaps rarely occurs. One of the main factors affecting rapid postoperative recovery of swallowing function in patients with HSCC is the loss of sensation in the mucosa of the residual larynx and hypopharynx due to surgical impairment of the ibSLN.4,5
The ibSLN is responsible for introducing the signal of the laryngeal cough reflex (LCR) to the central nervous system.14,15 Widdicombe and Tatar 16 reported that the LCR is abolished when the ibSLN is sectioned. During the swallowing process, the LCR prevents food and secretions from flowing into the lower airway through the larynx, ultimately preventing the occurrence of aspiration pneumonia. 17 The SLN splits into the ibSLN and external SLN at the level of the hyoid bone. The ibSLN, accompanied by the superior laryngeal artery, traverses laterally to medially and pierces the thyrohyoid membrane.5,18,19 In most cases, after piercing the thyrohyoid membrane, the ibSLN immediately courses through the lateral glossoepiglottic fold and splits into the superior, middle, and inferior branches. In some cases, however, the ibSLN splits into these branches proximal to the site where the thyrohyoid membrane is pierced.5,18,19 The superior branch of the ibSLN, which is responsible for the sensory afferents of the laryngeal face of the epiglottis and laryngeal vestibule, extends to the lingual face of the epiglottis and perforates the epiglottis. The middle branch of the ibSLN distributes fibers to the mucosa of the aryepiglottic fold and ventricular fold. The inferior branch of the ibSLN runs behind the postcricoid region to the mucosa of the lower pharynx. It establishes an anastomosis with the recurrent laryngeal nerve and sends fibers to the interarytenoid muscle by penetrating the mucosa of the postcricoid region.5,18 Understanding these courses and distributions of the ibSLN and its branches is helpful to avoid the risk of ibSLN injury caused by cutting or retractor-induced compression of the nerve during a surgery.
In the present study, we routinely preserved the main trunk of the ibSLN. The preservation of the branches of the ibSLN (Figure 2) was dependent on the location of the tumor. Specifically, the superior and middle branches of the ibSLN were well preserved during resection of the tumors arising from the internal wall of the pyriform fossa, whereas the middle branch of the ibSLN was partly transected or transected as a whole depending on the location and size of the tumor. Moreover, the inferior branch of the ibSLN was transected and removed along with the resected specimen. Testing of sensation in the larynx and hypopharyngeal mucosa showed that the cough reflex was consistently present in all patients after the surgery. The short indwelling time of the nasogastric tube also supported that the branches of the ibSLN were well preserved. In view of the severity of ibSLN excision and rapid recovery after ibSLN preservation observed in routine clinical practice, a randomized trial is not necessary at the present time. The idea of ibSLN preservation has been proposed in previous reports of supraglottic and supracricoid partial laryngectomy; however, the specific method of ibSLN preservation has not yet been elucidated.20-22 Therefore, the results of the present study cannot be compared with those of previous studies because whether the ibSLN was preserved remains unclear. Only one study to date has introduced a method to preserve the ibSLN. However, the corresponding report did not provide a detailed description of the postoperative recovery of sensation in the hypopharyngeal mucosa. Moreover, the number of patients was not stated in that report. 23 In the present study, in which the ibSLN and its branches were preserved during surgical treatment for HSCC in 12 patients, the importance of preservation of the ibSLN in the rapid recovery of sensation in the hypopharyngeal mucosa and in the achievement of a full normal oral diet after the surgery was elucidated.
Conclusion
Our study showed that the surgical methods of preservation of the ibSLN and its branches are feasible and important in the recovery of sensation in the hypopharyngeal mucosa and in the achievement of a full normal oral diet after undergoing surgery for HSCC.
Footnotes
Authors’ Note
This study was approved by the ethics committee of The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China. Informed consent was obtained from all participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation of China (No. 81972527) and Natural Science Foundation of Guangdong Province (No. 2014A030313031).