
Abstract
Objective
We conducted this meta-analysis to compare the efficacy of these two surgical methods by comparing the incidence of major evaluation indicators.
Methods
The databases such as PubMed, Embase, the Cochrane Library, China National Knowledge Infrastructure, Wanfang, and VIP information databases were searched.
Results
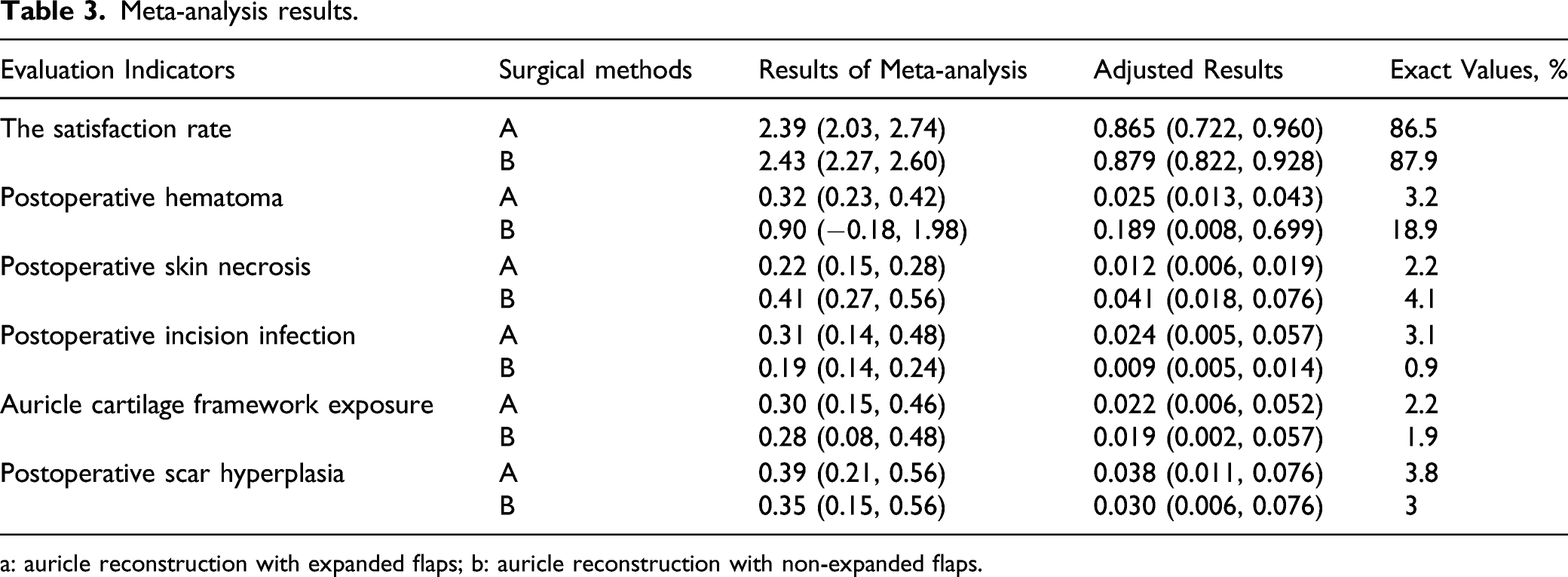
The satisfaction rate of patients with auricle reconstruction using expanded flaps was 86.5%, and the satisfaction rate of patients with auricle reconstruction using non-expanded flaps was 87.9%. The incidence of postoperative hematoma was 3.2% in patients with auricle reconstruction using expanded flaps and 18.9% in patients with auricle reconstruction using non-expanded flaps. The incidence of postoperative skin necrosis was 2.2% in patients with auricle reconstruction using expanded flaps and 4.1% in patients with auricle reconstruction using non-expanded flaps. The incidence of postoperative incision infection was 3.1% in patients with auricle reconstruction using expanded flaps and 0.9% in patients with auricle reconstruction using non-expanded flaps. The incidence of cartilage framework exposure was 2.2% in patients with auricle reconstruction using expanded flaps and 1.9% in patients with auricle reconstruction using non-expanded flaps. The incidence of postoperative scar hyperplasia was 3.8% in patients with auricle reconstruction using expanded flaps and 3% in patients with auricle reconstruction using non-expanded flaps. The publication bias of included literature was evaluated by Egger test. There was no publication bias in this Meta-analysis (P > .05).
Conclusion
The auricle reconstruction using non-expanded flaps is dominant in four of the six evaluation indexes. Therefore, we believe that the auricle reconstruction using non-expanded flaps has better therapeutic effect in patients with microtia. Due to the limitations of this meta-analysis, the conclusions of this meta-analysis still need to be further verified.
Introduction
Congenital microtia is one of the most common organ malformations in plastic surgery. 1 Its main treatment is auricle reconstruction. The reconstructed ear needs to have good shape, realistic detail, proper projection, and symmetrical position to be considered a successful auricle reconstruction. Because of the complexity of the surgery, auricle reconstruction is considered one of the most challenging procedures of plastic surgery. Since Dr Tagliacozzi first performed auricle reconstruction in 1597, plastic surgeons have invented many surgical methods for auricle reconstruction in the process of treating patients with congenital microtia, such as Tanzer method, Brent method, Nagata method, Park method, and so on. 2 Now, these methods are still widely used by plastic surgeons to treat congenital microtia.
At present, the methods of auricle reconstruction used by plastic surgeons are mainly divided into auricle reconstruction with expanded flaps and auricle reconstruction with non-expanded flaps. 3 Most of the studies published in recent years on auricle reconstruction with expanded flaps and auricle reconstruction with non-expanded flaps are observational studies on the therapeutic effects of one of the two kinds of surgery. Few studies have directly compared the efficacy of the two surgical methods. Therefore, there is insufficient direct evidence to evaluate the clinical efficacy of the two surgical methods. We conducted this meta-analysis to compare the efficacy of these two surgical methods by comparing the incidence of major evaluation indicators. It is expected to provide reference for plastic surgeons in the treatment of microtia.
Material and methods
This meta-analysis was carried out according to the PRISMA guidelines. 4
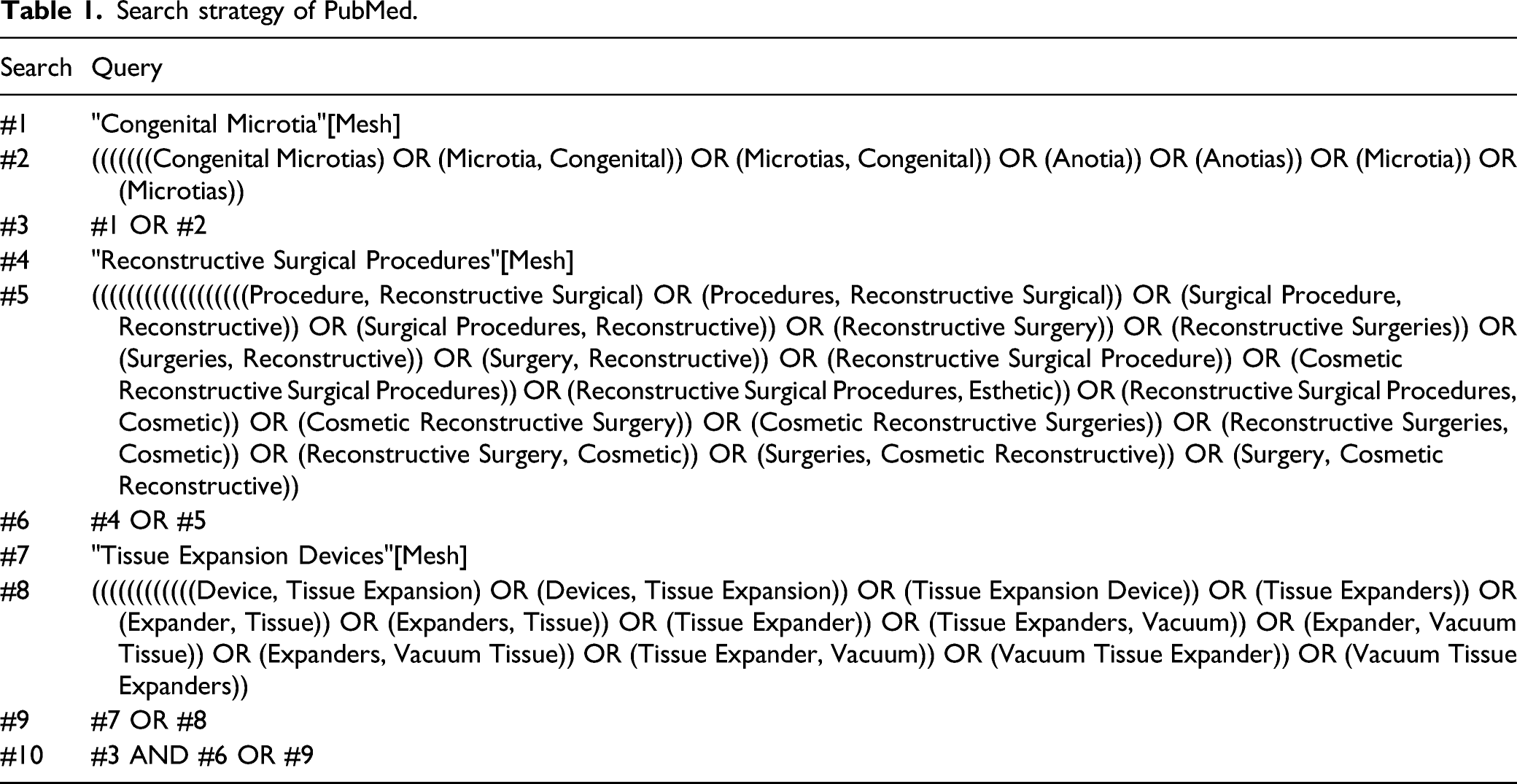
Search strategy
Search strategy of PubMed.
The inclusive and exclusive criteria
Inclusive criteria
Studies that include randomized controlled trials, controlled clinical trials, prospective and retrospective cohort comparative studies, case-control studies, and cross-sectional studies report on the treatment of microtia using auricle reconstruction with expanded flaps or auricle reconstruction with non-expanded flaps. The auricle frameworks used in auricle reconstruction are all cartilage frameworks. The study population is patients with congenital microtia. The evaluation indicators of the study include the satisfaction rate of patients to the effect of surgical treatment, postoperative hematoma, postoperative skin necrosis, postoperative incision infection, cartilage framework exposure, and postoperative scar hyperplasia.
Exclusive criteria
Articles are published repeatedly; studies do not include the research indicators needed for Meta-analysis; research data are missing. No auricle reconstruction with expanded flaps or auricle reconstruction with non-expanded flaps is used in the studies. The auricle frameworks used in auricle reconstruction are not cartilage frameworks. The study population is not patients with congenital microtia.
Data extraction and paper quality evaluation
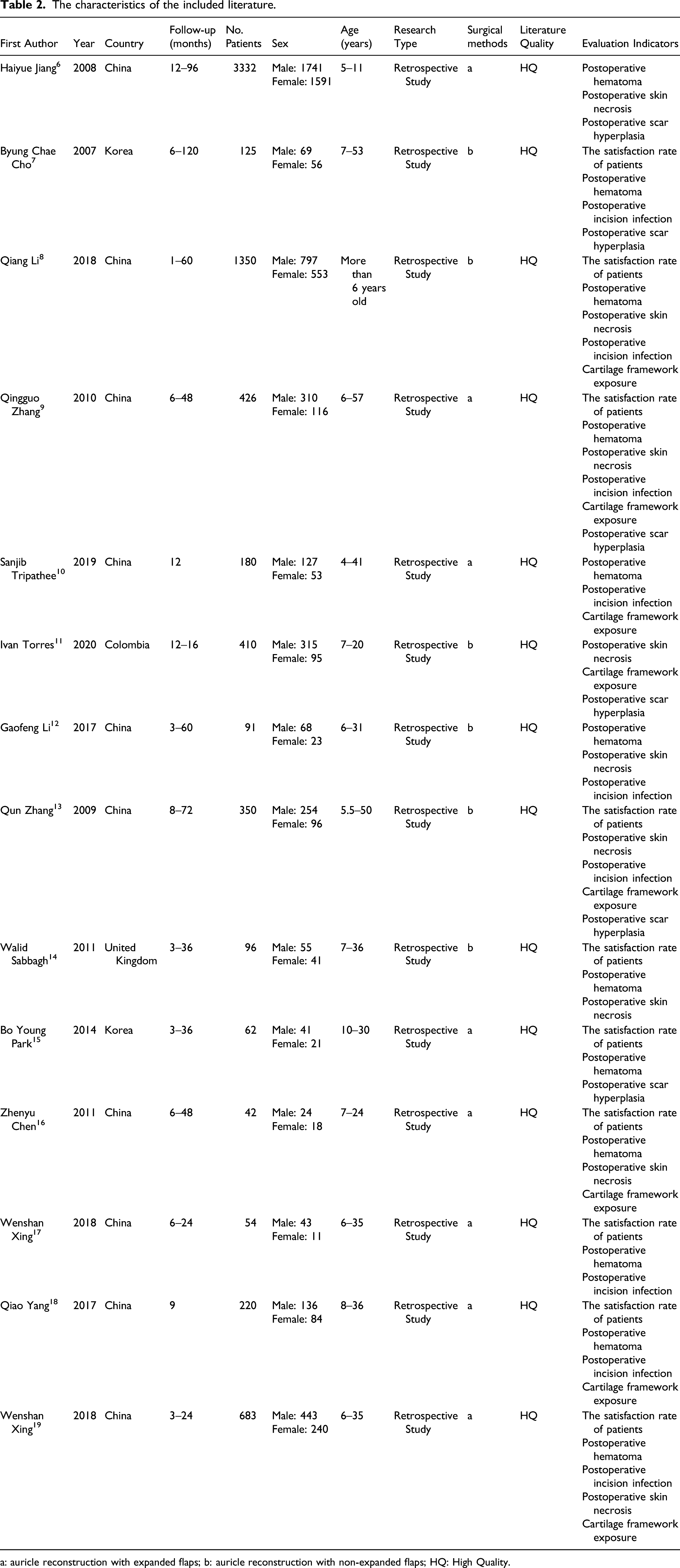
We developed a special standardized form for data extraction to extract the data from the included studies. The data extraction process will be done independently by the two researchers. The disagreements in the data extraction process will be resolved by a third researcher. The data extracted from the included articles include the first author of the article, the year of publication, the country, study design, sample size, evaluation indicators, research and conclusions. For the acquisition of missing data, we will contact the corresponding author of the study via email. The quality of included studies were evaluated by the Newcastle–Ottawa Scale (NOS). 5 The quality of the articles was evaluated from three aspects: patient selection, study comparability and outcome assessment. The highest quality of the literature was 9 stars and the lowest 0 stars. A score of 0–3 stars equated to a low quality (LQ) study, a score of 4–6 stars equated to a moderate quality (MQ) study, and a score of 7–9 stars equated to a high quality (HQ) study. Only HQ studies were included in this meta-analysis.
Statistical analysis
Stata 16.0 software was used for statistical analysis of the data. Original data included in the literature were first transformed by double arcsine method to make them conform to normal distribution and then analyzed in Stata. The initial conclusion obtained by Meta-analysis was then restored using formula (P = (sin(tp/2))2) to reach final conclusion. The therapeutic effect of the two surgical methods was compared by comparing the incidence of indicators. Heterogeneity was evaluated by the I2 statistic. The random effect model was used in this Meta-analysis. The publication bias of included literature was evaluated by Egger test. The Egger test with P < .05 as the existence of publication bias.
Results
Literature inclusion
A total of 5302 articles were retrieved. After screening, 14 articles were included in this meta-analysis.6-19 The literature screening process was shown in Figure 1. The characteristics of the included literature were shown in Table 2. PRISMA flow diagram. The characteristics of the included literature. a: auricle reconstruction with expanded flaps; b: auricle reconstruction with non-expanded flaps; HQ: High Quality.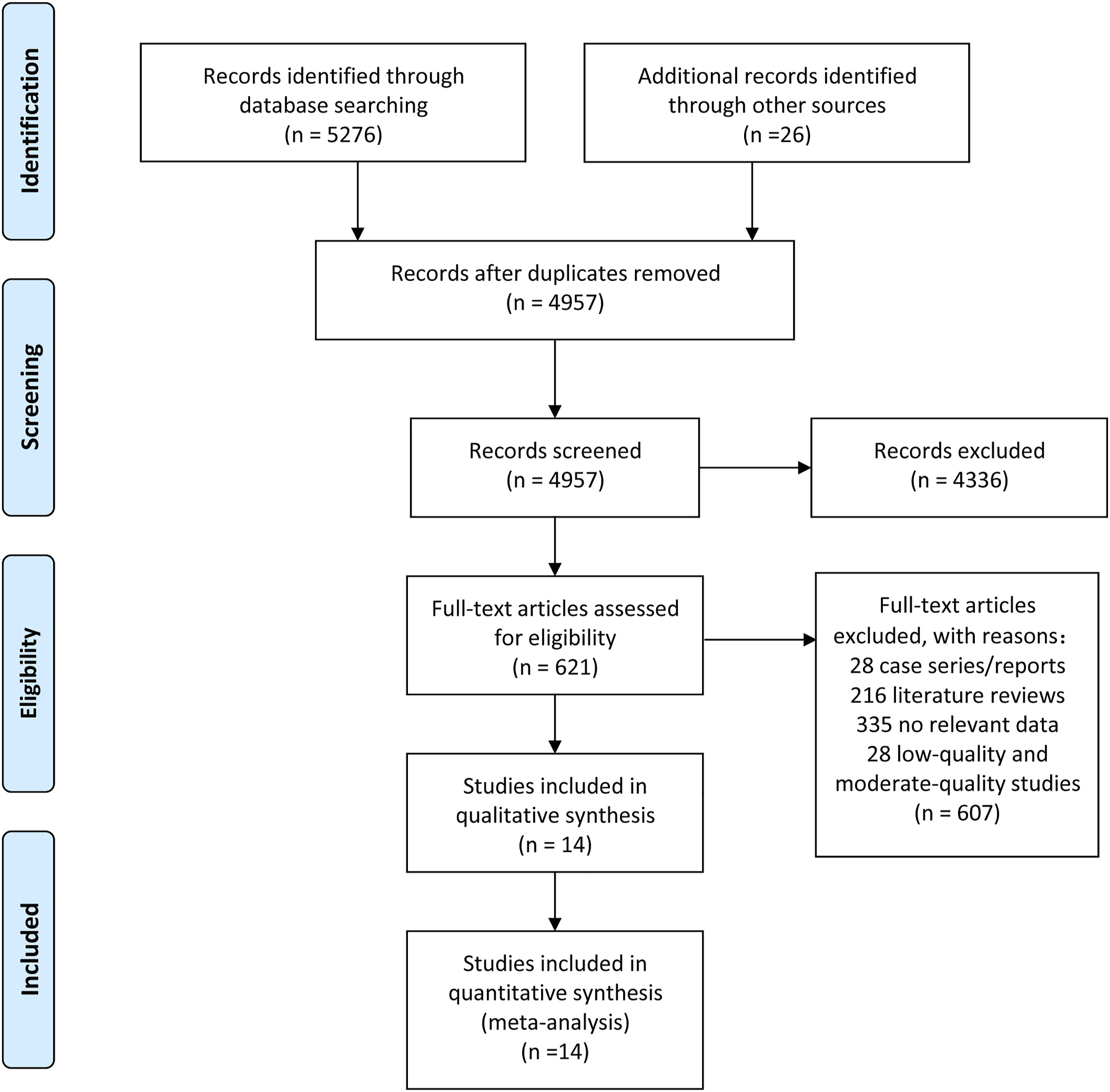
Meta-analysis results
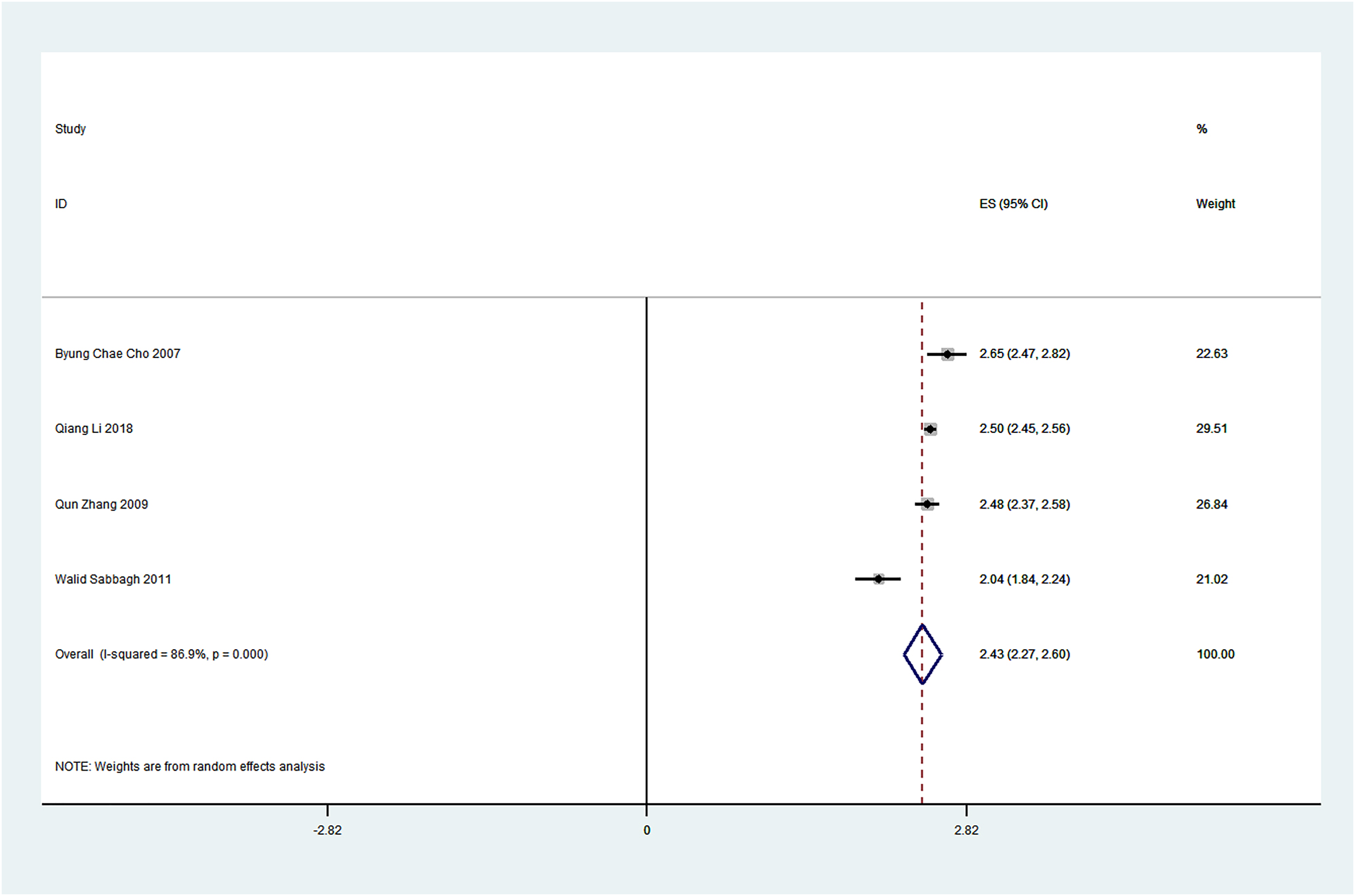
Due to the lack of control data in the single-arm meta-analysis, heterogeneity was high. In order to eliminate the influence of heterogeneity on the results, the random effect model was used for meta-analysis. Through the meta-analysis of the extracted data, we found that the satisfaction rate of patients with auricle reconstruction using expanded flaps was 86.5% (Figure 2), and the satisfaction rate of patients with auricle reconstruction using non-expanded flaps was 87.9% (Figure 3). The incidence of postoperative hematoma was 3.2% in patients with auricle reconstruction using expanded flaps and 18.9% in patients with auricle reconstruction using non-expanded flaps. The incidence of postoperative skin necrosis was 2.2% in patients with auricle reconstruction using expanded flaps and 4.1% in patients with auricle reconstruction using non-expanded flaps. The incidence of postoperative incision infection was 3.1% in patients with auricle reconstruction using expanded flaps and 0.9% in patients with auricle reconstruction using non-expanded flaps. The incidence of cartilage framework exposure was 2.2% in patients with auricle reconstruction using expanded flaps and 1.9% in patients with auricle reconstruction using non-expanded flaps. The incidence of postoperative scar hyperplasia was 3.8% in patients with auricle reconstruction using expanded flaps and 3% in patients with auricle reconstruction using non-expanded flaps. The detailed meta-analysis results were shown in Table 3. Meta-analysis of the satisfaction rate of patients with auricle reconstruction using expanded flaps. Meta-analysis of the satisfaction rate of patients with auricle reconstruction using non-expanded flaps. Meta-analysis results. a: auricle reconstruction with expanded flaps; b: auricle reconstruction with non-expanded flaps.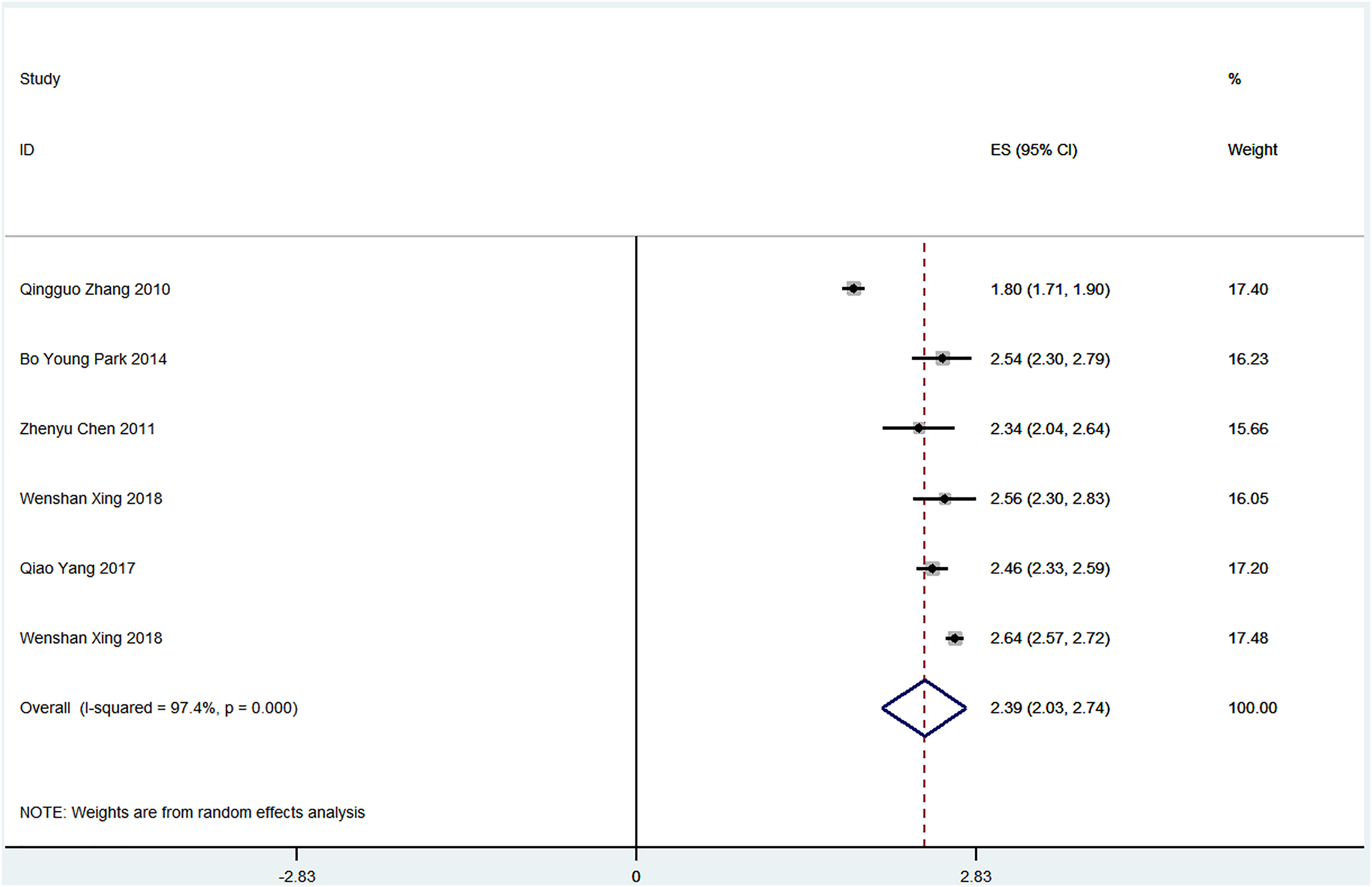
Publication bias detection
Results of Egger test.

a: auricle reconstruction with expanded flaps; b: auricle reconstruction with non-expanded flaps.
Discussion
In this study, a single-arm meta-analysis was used to compare the six evaluation indicators of auricle reconstruction with expanded flaps and auricle reconstruction with non-expanded flaps. Through data analysis, we found that the satisfaction rate, incidence of postoperative hematoma and incidence of postoperative skin necrosis of patients with auricle reconstruction using expanded flaps were all lower than those with auricle reconstruction using non-expanded flaps. However, the incidence of postoperative incision infection, the incidence of cartilage framework exposure, and the incidence of postoperative scar hyperplasia were all higher than those with auricle reconstruction using non-expanded flaps. The auricle reconstruction using non-expanded flaps is dominant in four of the six evaluation indexes (the satisfaction rate, the incidence of postoperative incision infection, the incidence of cartilage framework exposure, and the incidence of postoperative scar hyperplasia). Therefore, we believe that the auricle reconstruction using non-expanded flaps has better therapeutic effect in patients with microtia.
There are few clinical controlled studies that directly compare the efficacy of the two surgical procedures. Therefore, indirect comparison was used in this meta-analysis. We first used single-arm meta-analysis to calculate the satisfaction and complications rates of the two surgical procedures, respectively. The specific satisfaction rate and complications rate were compared to evaluate the efficacy of the two surgical procedures. Due to the lack of research data directly comparing the two surgical procedures, the two-arm meta-analysis cannot be used to determine whether there are statistical differences in the satisfaction and complications rates of the two surgical procedures.
In terms of patient satisfaction, patients with auricle reconstruction using expanded flaps were 1.4% lower than those with auricle reconstruction using non-expanded flaps. In terms of the incidence of postoperative hematoma, patients with auricle reconstruction using expanded flaps were 15.7% lower than those with auricle reconstruction using non-expanded flaps. In terms of the incidence of postoperative skin necrosis, patients with auricle reconstruction using expanded flaps were 1.9% lower than those with auricle reconstruction using non-expanded flaps. In terms of the incidence of postoperative incision infection, patients with auricle reconstruction using expanded flaps were 2.2% higher than those with auricle reconstruction using non-expanded flaps. In terms of the incidence of cartilage framework exposure, patients with auricle reconstruction using expanded flaps were 0.3% higher than those with auricle reconstruction using non-expanded flaps. In terms of the incidence of postoperative scar hyperplasia, patients with auricle reconstruction using expanded flaps were 0.8% higher than those with auricle reconstruction using non-expanded flaps. Judging from the above specific values, there is not much difference between the two surgical methods. After comprehensive comparison of the six evaluation indicators, the auricle reconstruction using non-expanded flaps has better efficacy.
Auricle reconstruction using non-expanded flaps does not require the use of skin expanders, and the patients can avoid the pain of skin expansion. 20 This may be the reason for a higher satisfaction rate. Compared with the expanded flaps, the non-expanded flaps used in auricle reconstruction are smaller, so they are more susceptible to the pressure of the cartilage framework and cause necrosis. Compared with expanded flaps, non-expanded flaps have less surgical field and more difficulty in hemostasis, so postoperative hematoma is more likely to occur. Because the auricle reconstruction using expanded flaps uses skin expanders, the incision is more susceptible to bacterial infection. Infection of the incision leads to poor healing of the incision, which is more likely to lead to cartilage framework exposure. Compared with auricle reconstruction using non-expanded flaps, the auricle reconstruction using expanded flaps involves skin expanders implantation, so it is more traumatic to patients and more likely to cause postoperative scar hyperplasia.
Both the auricle reconstruction with expanded flaps and the auricle reconstruction with non-expanded flaps have advantages and disadvantages.6-23 The auricle reconstruction with expanded flaps is generally not affected by the degree of ear malformation and is suitable for most patients with microtia. Moreover, the expanded flaps have more blood circulation and are easier to survive. The expanded flaps are thinner and can better present the subunits of the reconstructed auricle after covering the cartilage frameworks, making the shape of the reconstructed auricles more beautiful. But the auricle reconstruction with expanded flaps require the implantation of skin dilators, which takes a longer time to expand skin flaps and increases the risk of complications related to skin dilators, such as water leakage of the skin dilators and exposure of the skin dilators. The auricle reconstruction with expanded flaps increases the duration and cost of treatment for patients with microtia. The auricle reconstruction with non-expanded flaps do not require skin expander implantation, the treatment period is short, and postoperative complications related to skin expanders will not occur. However, the flaps used in auricle reconstruction are not expanded, and the blood circulation of the flaps is easily affected when the flaps are used to cover the cartilage frameworks, resulting in necrosis of the flaps. In addition, the effect of auricle reconstruction with non-expanded flaps is better in patients with loose and thin skin behind malformed ears.
A total of 14 studies involving 7421 patients were included in this meta-analysis. Of these, 4999 patients underwent auricle reconstruction with expanded flaps and 2422 patients underwent auricle reconstruction with non-expanded flaps. To date, this is the first meta-analysis comparing the efficacy of auricle reconstruction with expanded flaps vs auricle reconstruction with non-expanded flaps in patients with microtia. The articles included in this study are of high quality, the sample size is large, the analysis is scientific and rigorous, and the conclusions drawn from this study are of high credibility. However, this meta-analysis also has some limitations: (1) The studies included in single-arm meta-analysis lacked control groups and showed great heterogeneity; (2) Among the 14 studies included in this meta-analysis, 10 were from China, 2 from Korea, 1 from Colombia, and 1 from the United Kingdom. The majority of the populations included in this meta-analysis were from the eastern population. Therefore, whether the conclusions of this study are applicable to patients of other races still needs to be further verified. (3) Although no publication bias was found, this study may still be affected by potential publication bias.
In summary, the auricle reconstruction using non-expanded flaps is dominant in four of the six evaluation indexes. Therefore, we believe that the auricle reconstruction using non-expanded flaps has better therapeutic effect in patients with microtia. Due to the limitations of this meta-analysis, the conclusions of this meta-analysis still need to be further verified.
Footnotes
Acknowledgments
This article does not contain any studies with human participants or animals performed by any of the authors. For this type of study informed consent is not required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is supported by the Institute Foundation of Plastic Surgery Hospital, Chinese Academy of Medical Sciences (3060120031).