
Abstract
Objectives
The traditional Tanzer-Brent method, which uses the integral engraving of costal cartilage, provides insufficient three-dimensional sensation and is characterized by poor firmness of the auricle framework. This tends to cause the absorption deformation of the auricle framework after surgery. In order to reduce the absorption deformation as well as make the reconstructed auricle more three-dimensional and the ear shape more realistic, our ear reconstruction team invented a novel method to make an auricle framework with autologous costal cartilage. The auricle framework made by this novel method has been applied to auricle reconstruction and has achieved excellent surgical results.
Patients and Methods
Clinical data and postoperative data were collected for patients with unilateral microtia who received auricle reconstruction using the novel method of auricle framework construction in Plastic Surgery Hospital from January 2020 to June 2022. The therapeutic effect of this novel method was evaluated by the satisfaction rate of patients and their families and by the prevalence of postoperative complications.
Results
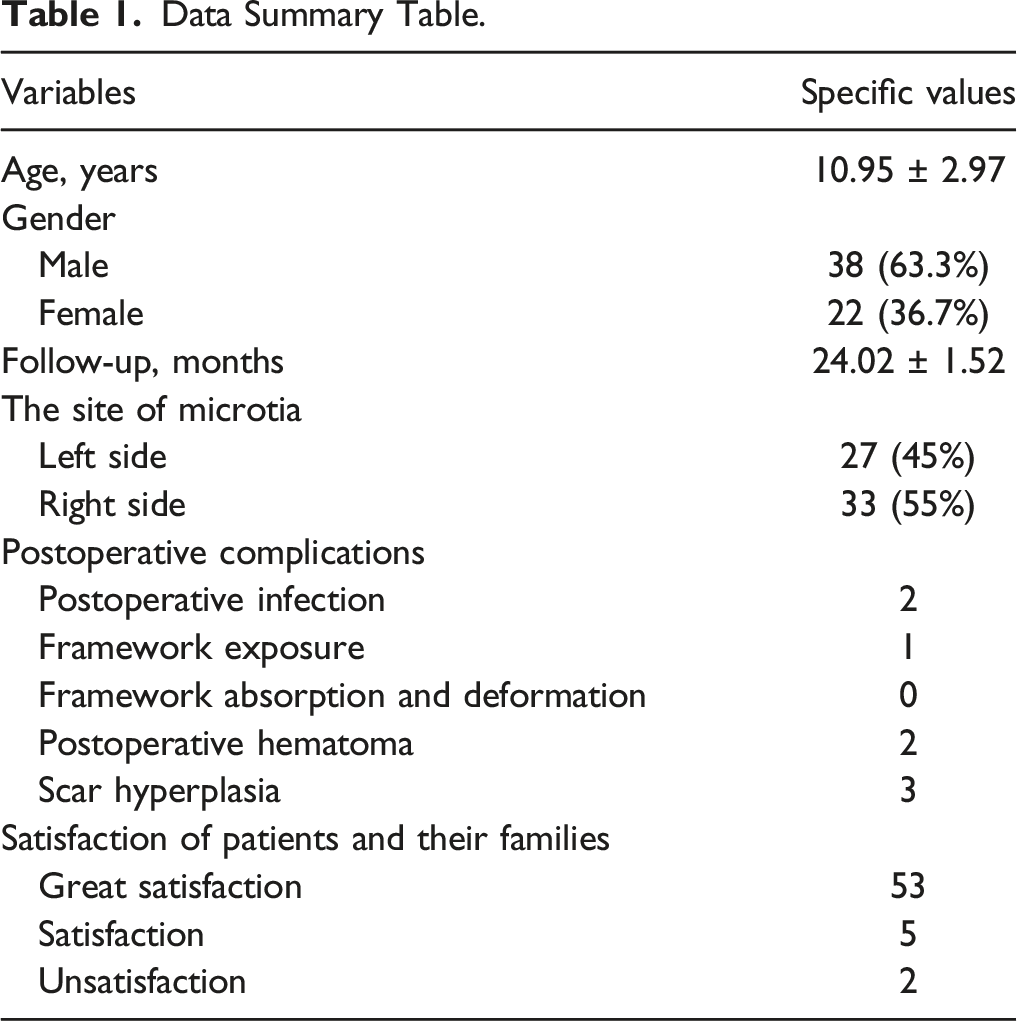
A total of 60 patients were enrolled in this study. The average age was (10.95 ± 2.97) years old. The mean follow-up time was 24.02 ± 1.52 months. The satisfaction rate of patients and their families was 96.7%. In terms of postoperative complications, two patients had postoperative infection, one patient had framework exposure, no patients had framework absorption and deformation, two patients had postoperative hematoma, and three patients had scar hyperplasia.
Conclusion
This novel method of making the auricle framework is more standardized, easier to master for plastic surgeons, and more conducive to the clinical application of plastic surgery. Through this study, we believe that this novel method offers significant therapeutic advantages and can be used as a unified standard for construction of an auricle framework using autologous costal cartilage.
Introduction
Microtia is one of the common organ malformations in plastic surgery. 1 Auricle reconstruction is the main treatment for microtia. Successful auricle reconstruction requires the reconstructed ear with good shape, realistic details, proper projection, and symmetrical position. Auricle reconstruction is considered one of the most challenging procedures in plastic surgery due to its complexity. 2 In auricle reconstruction surgery, the auricle stent currently used is mainly divided into two types, one is the auricle framework made of medical high-density porous polyethylene biological material (Medpor), and the other is the auricle framework made of the patient’s autologous costal cartilage. 3 Auricle frameworks made from autologous costal cartilage are more commonly used in the treatment of microtia patients in China. 4
The auricle framework made from the patient’s autologous costal cartilage has many advantages, such as avoiding the occurrence of immune rejection reaction, reducing the situation of foreign body infection, and reducing the surgical cost of the patients. However, the technical requirements for doctors to make auricle frameworks with autologous costal cartilage are higher.
5
The traditional Tanzer-Brent method, which uses the integral engraving of costal cartilage (Figure 1), has insufficient three-dimensional sensation and poor firmness of the auricle framework, which is easy to cause the absorption deformation of the auricle framework after surgery, thus affecting the surgical effect.
6
In order to reduce the absorption deformation of the auricle framework after surgery and make the reconstructed auricle more three-dimensional and the ear shape more realistic and beautiful, our ear reconstruction team invented a novel method to make auricle framework with autologous costal cartilage. Similar to Lego building blocks, the auricle framework is made by sculpting rib cartilage into components that are then assembled together. By this method, the structures of the helix, the antihelix, the scapha, the triangular fossa, and the upper foot and the lower foot of the antihelix were three-dimensional and realistic. Moreover, we apply the traditional Chinese mortise and tenon joint structure in the auricle framework so as to increase the stability of auricle framework and make it not easy to deform. The auricle framework made by this new method has been applied to auricle reconstruction and achieved excellent surgical results. The traditional Tanzer-Brent method, which uses the integral engraving of costal cartilage.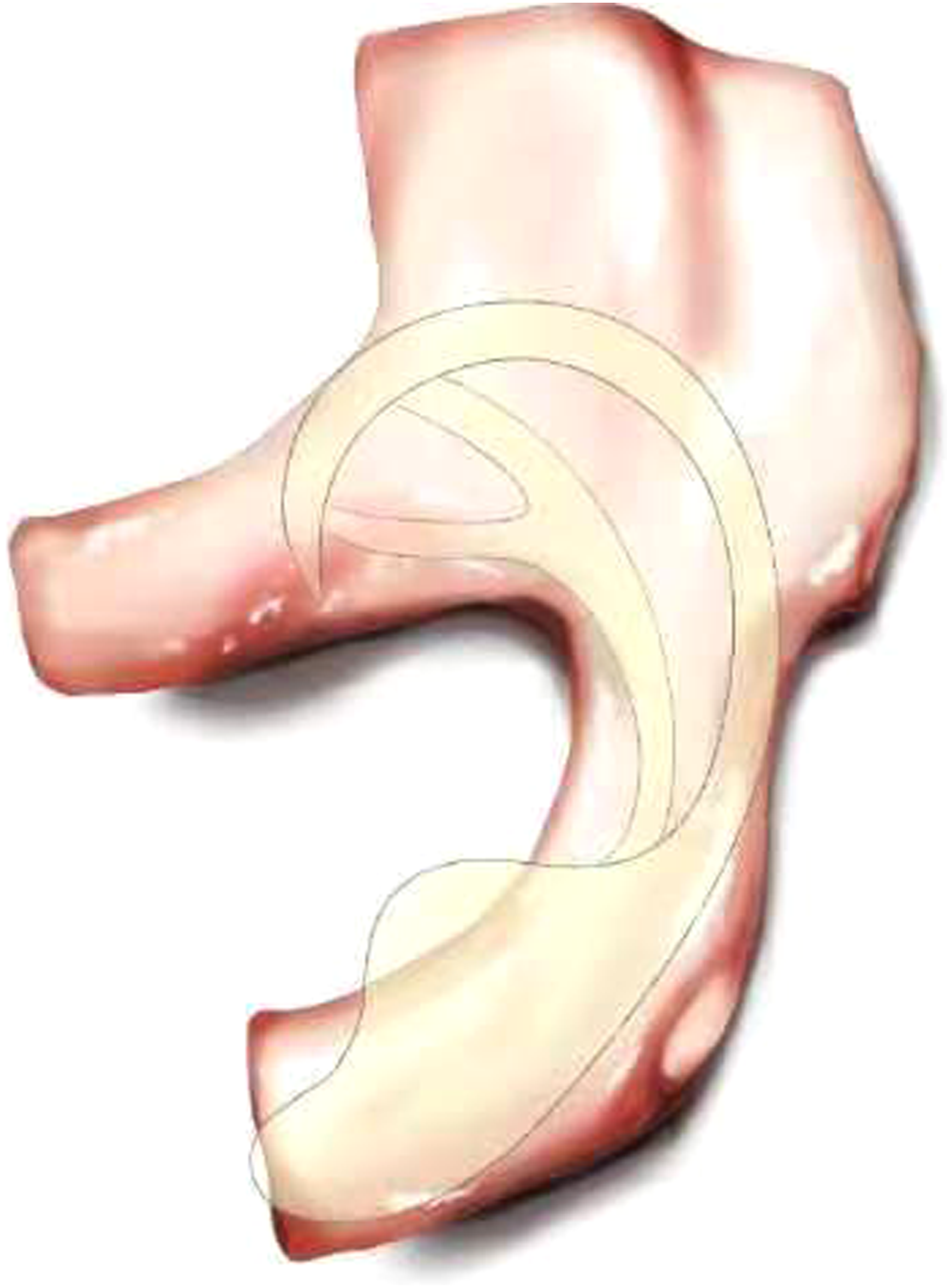
Patients and Methods
The study was reported following the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement. 7
Clinical Data
Clinical data and postoperative data of patients with unilateral microtia who received auricle reconstruction using the novel method of auricle framework in Plastic Surgery Hospital from January 2020 to June 2022 were collected.
Ethics Approval and Consent to Participate
Patients and their families who participated in the study have signed informed consent. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study has been approved by Medical Ethics Committee of Plastic Surgery Hospital, Chinese Academy of Medical Sciences.
Inclusion and Exclusion Criteria
Inclusion criteria: Patients with unilateral microtia were healthy without other serious diseases and could tolerate general anesthesia without obvious hemifacial shortness; The patient and his family agreed with the doctor’s diagnosis and treatment plan and cooperated with the doctor’s follow-up.
Exclusion criteria: Patients with bilateral microtia; Patients unable to tolerate general anesthesia; Patients with obvious hemifacial shortness; Patients and their families refused to sign informed consent.
Surgical Methods
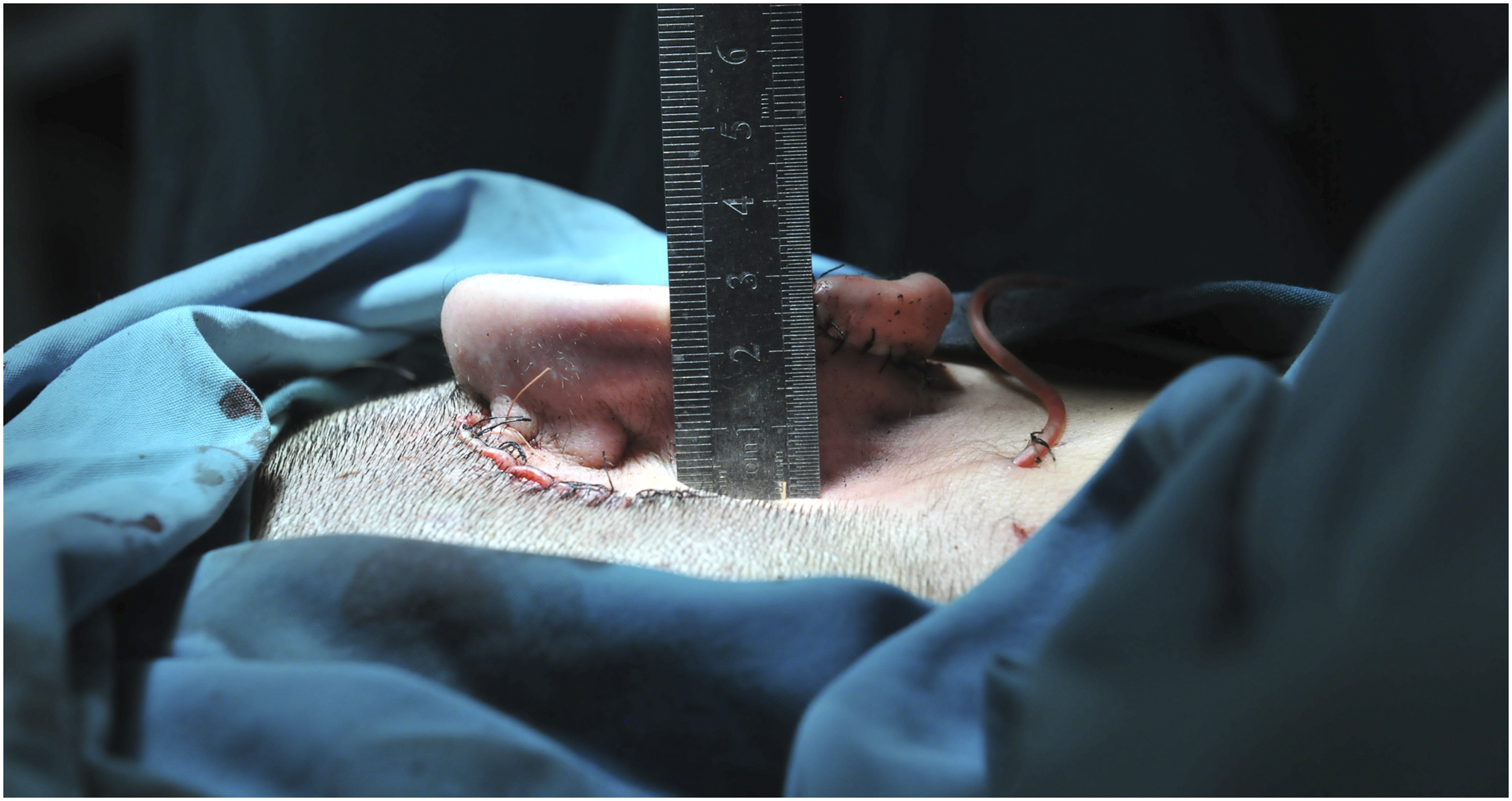
The patient was placed in supine position. After general anesthesia, the posterior ear skin dilator was removed and the expanded flap was trimmed. The 6th, 7th and 8th costal cartilages on the right side of the patient were removed (Figure 2A). The auricle framework was made according to the two-dimensional ear mold of the patient’s healthy side. The 6th costal cartilage was carved into the base part of the auricle bracket, and the scapha and upper foot of the antihelix were carved on the upper part (Figure 2B). Part of the 6th costal cartilage was carved into the lower foot of the antihelix (Figure 2C). Part of the 8th costal cartilage was spliced to the lower end of the base of the auricle framework to form the earlobe part of the auricle framework. Grooves are carved in the splicing part of the lower foot of the antihelix carved from the 6th costal cartilage, the main body of the auricle framework and the lower foot of the antihelix form a mortise and tenon joint structure when combined so as to increase the stability of the auricle framework after assembly (Figure 2D and 2E). The 7th costal cartilage was divided lengthways to carve the helix and antihelix of the auricle framework (Figure 2F and 2G). The remaining 6th, 7th, and 8th autologous costal cartilage fragments were assembled on the dorsal side of the base of the auricle framework to increase the height of the auricle framework to form a suitable projection for the reconstructed auricle (Figure 2H-2J). The expanded flap was used to cover the three-dimensional auricle framework, and the reconstructed auricle was adjusted to the symmetrical position of the healthy ear. After the surgical incision was sutured, a symmetrical and realistic reconstructed auricle was formed (Figures 3
-6). The novel method of making auricle framework. (A): The 6th, 7th, and 8th costal cartilages on the right side of the patient were removed. (B): The 6th costal cartilage was carved into the base part of the auricle bracket, and the scapha and upper foot of the antihelix were carved on the upper part. (C): Part of the 6th costal cartilage was carved into the lower foot of the antihelix. (D): Grooves are carved in the splicing part of the lower foot of the antihelix carved from the 6th costal cartilage. (E): the main body of the auricle framework and the lower foot of the antihelix form a mortise and tenon joint structure when combined. (F): The 7th costal cartilage was divided lengthways. (G): The 7th costal cartilage was carved into the helix and antihelix of the auricle framework. (H): Frontal view of auricle framework. (I): Lateral view of auricle framework. (J): Posterior view of auricle framework. Lateral view of a typical patient with right ear reconstruction. Posterior view of a typical patient with right ear reconstruction. Lateral view of a typical patient with left ear reconstruction. Posterior view of a typical patient with left ear reconstruction.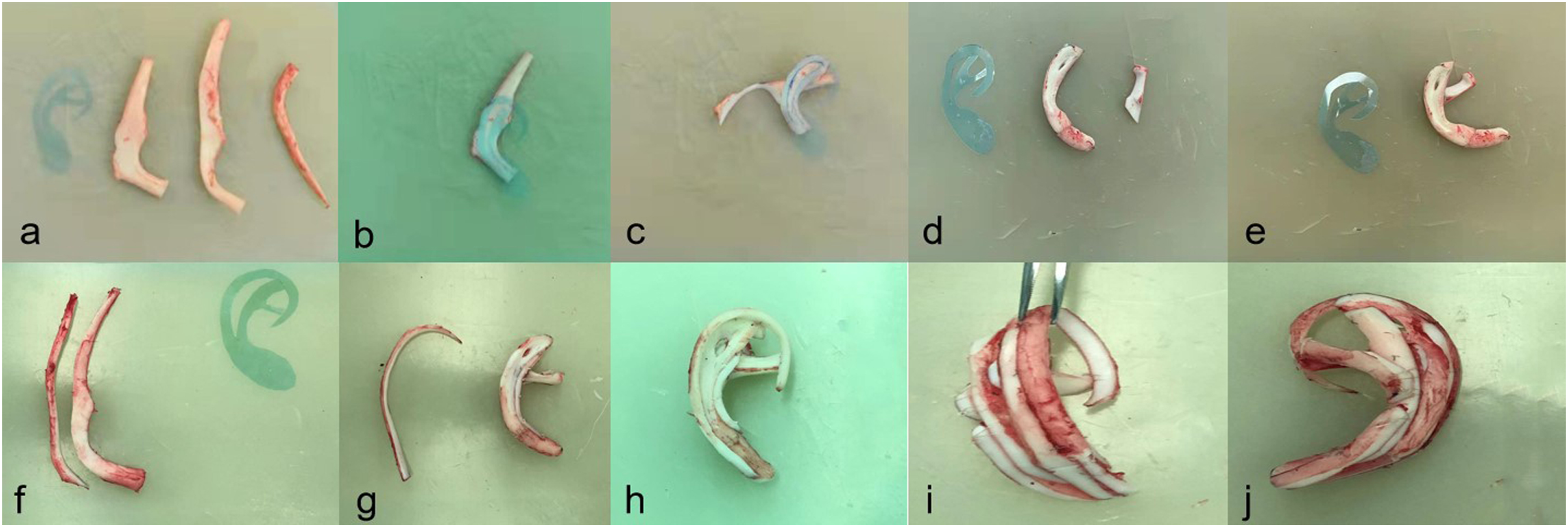



Main Outcome Measures
We conducted postoperative follow-up for each patient by telephone, and each patient was followed-up once a month. And the therapeutic effect of the novel method to make auricle framework was evaluated mainly by the satisfaction rate of the patients and their families. In addition, we also recorded the postoperative complications of the patients.
Results
Data Summary Table.

Lateral view of a typical patient 2 years after auricle reconstruction.
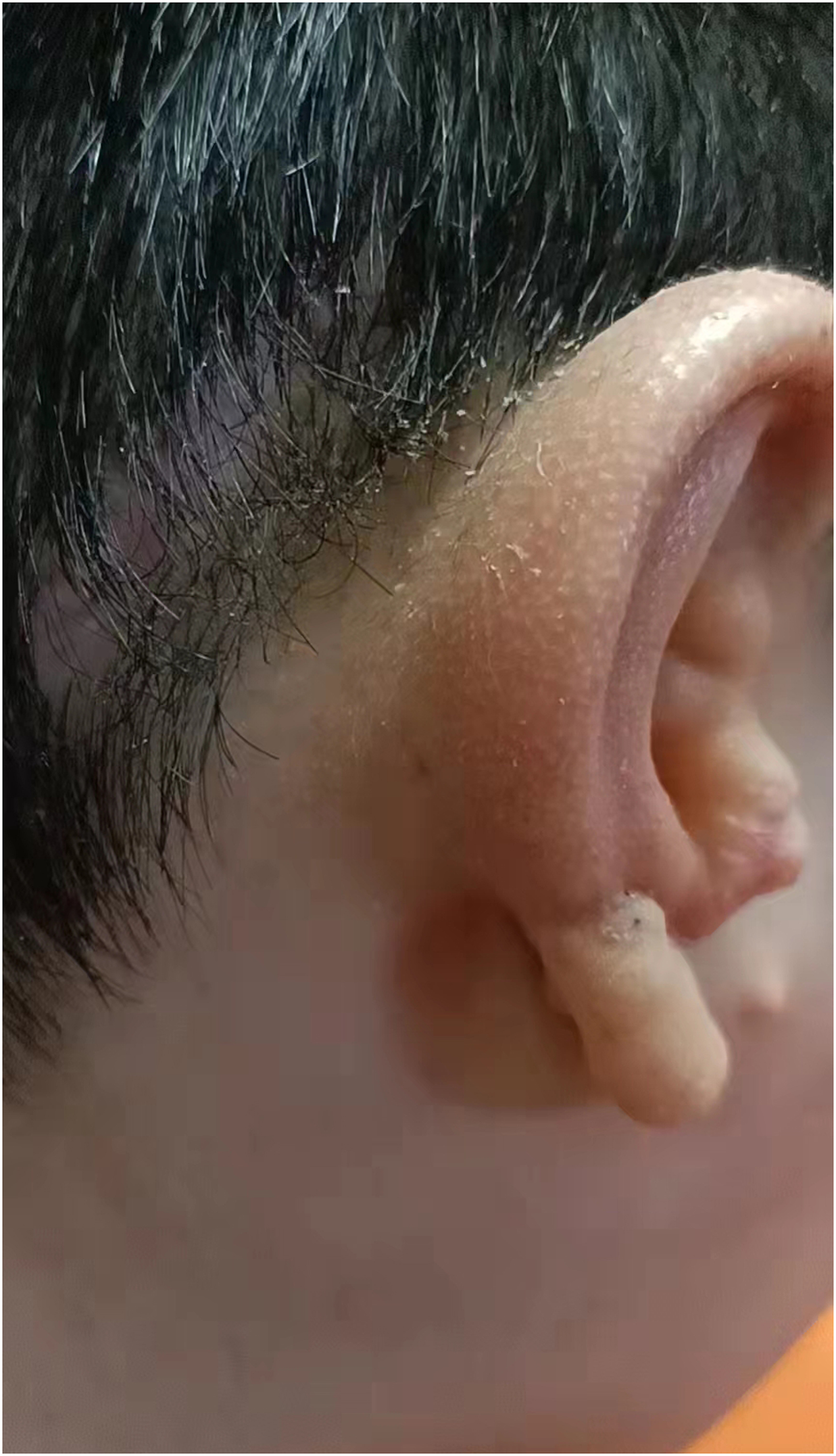
Posterior view of a typical patient 2 years after auricle reconstruction.
Discussion
At present, auricle reconstruction with expanded flap combined with autologous costal cartilage transplantation is the mainstream surgical method for congenital microtia in China.
8
The operation is divided into 3 stages: the first stage is to prepare the expanded flap by embedding the skin expander behind the ear; the second stage is to use the patient's autologous costal cartilage to make auricle framework and cover it with the expanded flap to form the reconstructed auricle; and the third stage is to repair the shape of reconstructed auricle.
9
Among them, the key point and difficulty of surgery is to use the patient’s autologous costal cartilage to make the auricular framework. The morphology and stability of the auricular framework are directly related to the morphology of the reconstructed auricle. However, at present, there is no unified standard for the fabrication of autologous costal cartilage auricular framework, and the fabrication of auricle framework is greatly influenced by the experience and technique of the surgeons.
10
Therefore, we invented the novel method of making auricle framework. This novel method uses the 6th, 7th, and 8th costal cartilage, carving each costal cartilage separately into the parts needed to assemble the auricle framework, which assembled like Lego building blocks. And triangular structure and mortise-tenon joint structure are used to increase the stability of auricle framework (Figure 9). Triangular structure and mortise-tenon joint structure are used to increase the stability of auricle framework. (A): mortise-tenon joint structure. (B): triangular structure.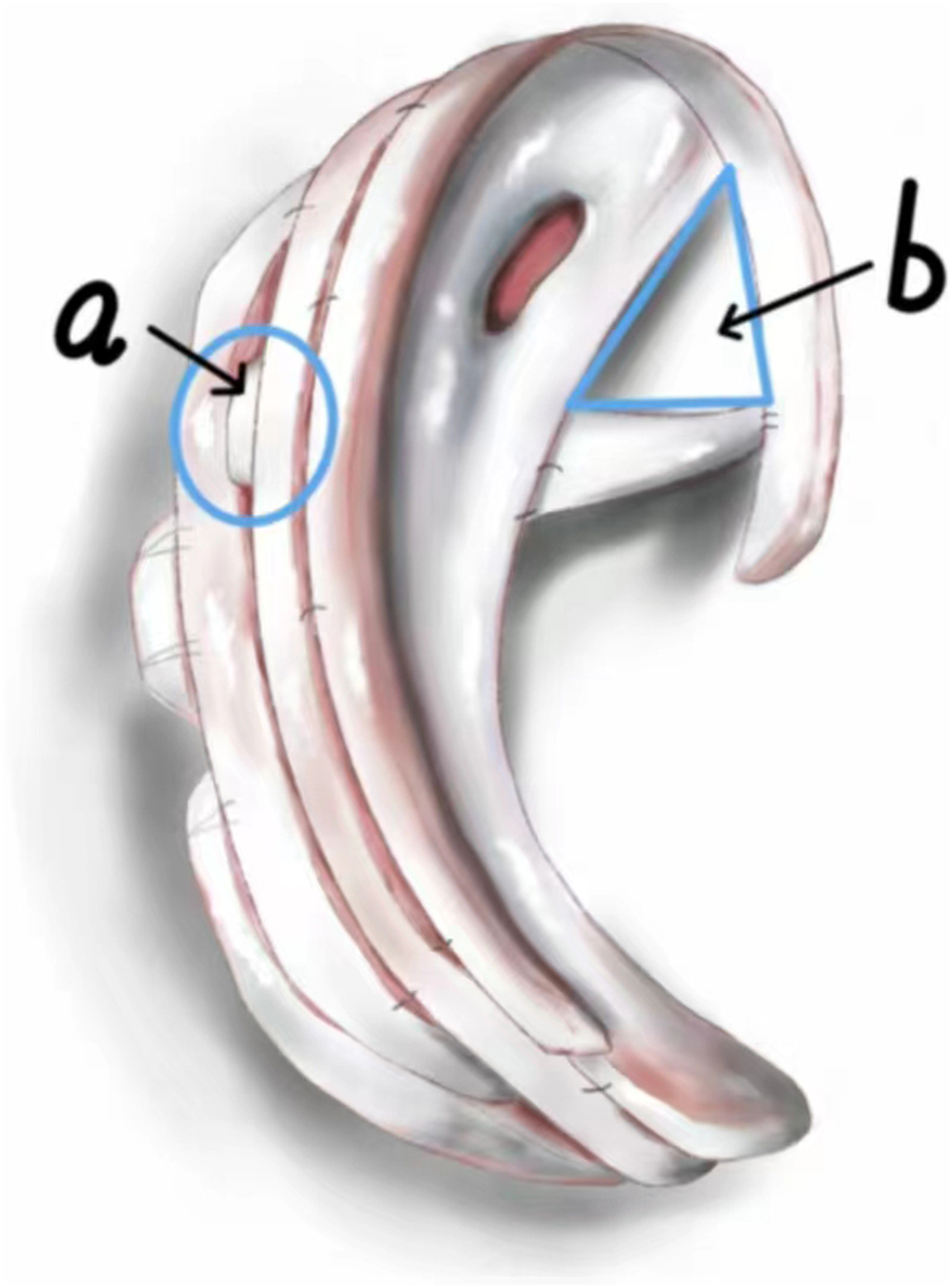
In the previous study, we invented the biplane skin expansion technique, which can effectively expand the skin behind the ear. 9 The skin expander makes the area of the skin behind the ear larger and the thickness thinner, and the shape of the ear is more realistic and beautiful after covering the auricle framework. In this study, we found that the auricle framework made by the novel method had a better three-dimensional sense, the shape of reconstructed auricle was realistic, and the subunits of the reconstructed auricle were beautiful in shape. Moreover, auricle framework had strong stability and no postoperative complications of absorption and deformation. Although postoperative complications such as postoperative infection, framework exposure, postoperative hematoma, and scar hyperplasia occurred in the patients in this study, none of them had anything to do with auricle framework itself. And patients and their families have a high satisfaction rate with the symmetry of reconstructed auricle and the aesthetics of reconstructed auricle. Therefore, we believe that the novel method of making auricle framework has a significant therapeutic effect and can be used as a unified standard for plastic surgeons to make auricle framework using autologous costal cartilage. We suggest that plastic surgeons should master the biplane skin expansion technique and this novel method of making auricle framework, and that the combination of these two methods can achieve significant surgical results.
This novel method of making auricle framework has obvious advantages and disadvantages. The advantages are to make the auricle framework more standardized, easier to master, be popularized, and applied. We used the 6th costal cartilage to make the scapha and the upper foot and lower foot of the antihelix, the 7th costal cartilage to make the helix and antihelix of the auricle framework, and the 8th costal cartilage to make the earlobe part of the auricle framework. The remaining costal cartilage fragments were used to raise the auricle framework to make the auricle framework more stereoscopic. The disadvantages of this method are that the operation of taking the patients’ costal cartilages increases the trauma of the patients’ bodies and prolongs the time of surgery and anesthesia. If the operation is not done properly, pneumothorax, hemothorax, and other serious complications may occur.
In conclusion, this novel method of making auricle framework is more standardized, easier to be mastered by plastic surgeons, and more conducive to the clinical application of plastic surgery. Through this study, we believe that this novel method we invented has significant therapeutic effect and can be used as a unified standard for plastic surgeons to make auricle framework using autologous costal cartilage.
Footnotes
Acknowledgments
The authors thank all the patients for their participation and permission in this study. We acknowledge TopEdit LLC for the linguistic editing and proofreading during the preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that supports the findings of this study are available in the supplementary material of this article.