
Abstract
Large cell neuroendocrine carcinoma (LCNEC) of the larynx is an exceedingly rare cancer of the head and neck that is difficult to diagnose. Few case reports of laryngeal LCNEC exist within the literature, and it was not until recently that LCNEC was recognized as a discrete subtype of neuroendocrine carcinoma. Given its recent recognition as a distinct subtype, histologic characteristics distinguishing LCNEC from other poorly differentiated carcinomas remain under investigation. Various reports have shown genetic alterations such as p53 and/or p16 overexpression, which are typically associated with infection by human papilloma virus (HPV). However, some reports have shown p53 and/or p16 overexpression in HPV negative samples. In this case, we discuss a 67-year-old patient with a history of extensive alcohol and tobacco use with a newly diagnosed T4N0M0, high grade, LCNEC of the subglottic larynx. Tumor pathology demonstrated positive staining for typical neuroendocrine (NE) markers like synaptophysin and chromogranin A; however, there was diffuse CK34βE12 and p16 expression. LCNEC is a newly classified subtype of poorly differentiated neuroendocrine (NE) tumors, and the diagnosis requires consideration of the clinical presentation, microscopic features, and immunostaining markers.
Introduction
Large cell neuroendocrine carcinoma (LCNEC) of the larynx is a rare tumor of the head and neck with a reported overall average incidence of .0117 per 100,000 people from 1973 to 2011. 1 Laryngeal LCNEC presents later in life with studies reporting an average age at diagnosis between 60 and 68 years and typically in an advanced stage.1,2 The 5-year disease specific survival for all laryngeal neuroendocrine carcinomas have been reported as low as 30.2%. 1 Laryngeal LCNEC is a rare, morbid condition, which necessitates rapid, accurate diagnosis for determining prognosis and guiding treatment.
LCNEC is a new variant of poorly differentiated neuroendocrine carcinomas that was recently defined in the 2017 World Health Organization (WHO) classification of head and neck tumors. 3 The histologic and immunohistochemical patterns of LCNEC are still evolving. Synaptophysin and chromogranin-A are well established NE markers that are also found in laryngeal LCNEC. In our case, the patient’s tumor stained positively for CK34βE12 and p16 in addition to the typical NE markers. We report this case to discuss the diagnostic challenge of LCNEC particularly in tumors that express atypical cellular markers.
Case report
A 67-year-old male presented to the emergency department with a two-week history of progressive stridor and hoarse voice. He reported an extensive drinking and smoking history, 1–2 packs per day for at least 20 years. The otolaryngology—head and neck surgery team was consulted for evaluation. Physical examination demonstrated moderate coarse dysphonia and biphasic stridor unimproved with the use of steroids. Flexible laryngoscopy examination did not show any obvious glottic lesions but there was some limited abduction of the vocal folds. The subglottis was not well visualized. CT neck with contrast was performed and showed a soft tissue mass at the left subglottis, with erosion of the cricoid cartilage and narrowing of the subglottic airway (Figure 1A). Given the patient’s presentation, he was taken urgently to the operating room for awake tracheostomy, direct laryngoscopy, and biopsy. Intraoperative findings included a large, friable left subglottic mass lesion extending from 10 mm below the superior surface of the left true vocal cord to 22 mm inferior. (Figure 1B). (A) Axial CT image showed tumor erosion of the anterior margin of the left cricoid cartilage; (B) Tracheoscopy image demonstrating tumor extension into the subglottic larynx.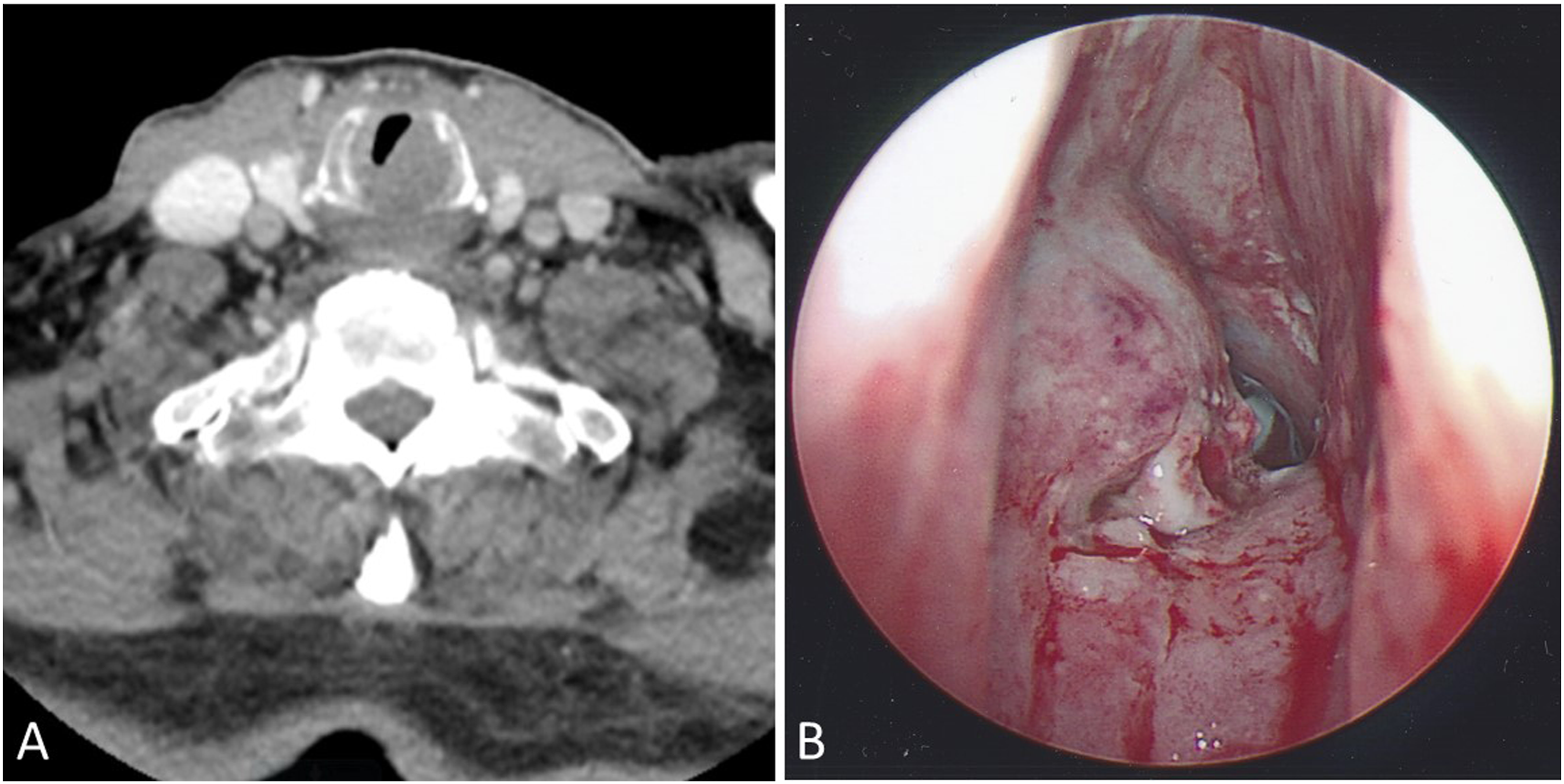
Ultimately, pathologic analysis of the specimen revealed a poorly differentiated neuroendocrine carcinoma, high-grade, large cell type. There was comedonecrosis and high mitotic activity. The tumor cells were positive for CK34βE12, synaptophysin, chromogranin A, and CD56 (Figures 2A-D). P40 was negative. Ki-67 exhibited a high proliferation index (>80%). P16 immunostaining showed strong, diffuse signal. Final staging was consistent with a T4aN0M0 poorly differentiated neuroendocrine tumor, high-grade, large cell type. Treatment options including surgical resection with total laryngectomy and medical treatment with chemoradiation were discussed. The patient elected for chemoradiation therapy and was treated with three cycles of carboplatin and etoposide therapy and 30 Gy at 200 cGy/fraction/day for 6 weeks. Unfortunately, the patient developed extensive local recurrence at one-year post-treatment, and the patient chose to enter hospice care. (A) H&E stain showed tumor cells with cribriform pattern; (B) Synaptophysin IHC stain with diffused positivity; (C) Chromogranin IHC stain with patchy positivity; (D) CD 56 IHC stain with diffused positivity.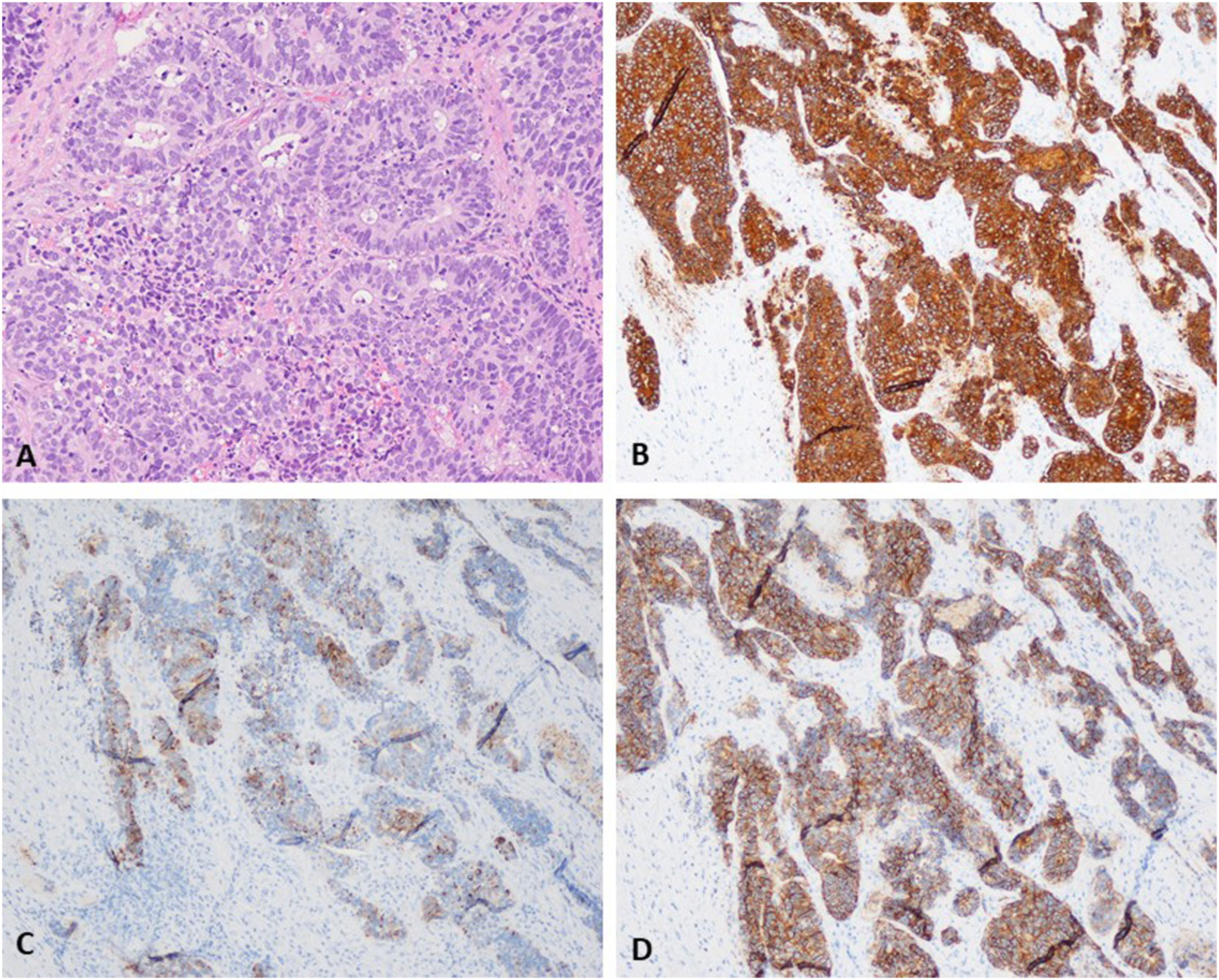
Discussion
Neuroendocrine tumors of the head and neck are rare; the larynx is the most common site, though they make up only 1% of tumors in this region with the most common site being the supraglottis. 4 There are only three prior cases of large cell neuroendocrine carcinoma of the subglottis published in the literature.2,5,6 The median age of presentation for these tumors is in the sixth decade of life, and there is a male preponderance for most subtypes. 2 Most of those diagnosed with large cell neuroendocrine carcinoma of the larynx present with stage IV disease, and over 90% of laryngeal neuroendocrine tumors occur in smokers. 3 Survival for large cell neuroendocrine carcinoma is poor, with a three-year overall survival of only 11% and 5-year survival of 15.3%, which is significantly lower than the other histologic grades of laryngeal neuroendocrine tumors.2,4,7 In addition, the recurrence rate for large cell neuroendocrine tumors is reported as high as 81%. 2
Classification of these tumors is based on histologic factors including differentiation grade and cell size. The WHO updated their classification in 2017 to include three general types: well-differentiated (representing low-grade or grade 1), moderately differentiated (representing intermediate-grade or grade 2), and poorly differentiated (representing small cell and large cell types and high-grade or grade 4 carcinoma).2,3 The LCNEC variant of poorly differentiated laryngeal tumors must be further characterized by certain required criteria: tumor cells containing large cytoplasm, patterns of neuroendocrine differentiation (nesting, trabecular formation, peripheral palisading), mitotic activity greater than 10/10 per high power field (HPF), and confirmatory immunohistochemical staining for chromogranin A, synaptophysin, and/or CD56.3,7 Large cell neuroendocrine tumors also tend to have more necrosis, mitoses, and abundant cytoplasm than lower grade laryngeal carcinomas.3,8
The differential diagnosis of a laryngeal carcinoma includes neuroendocrine carcinoma, basaloid squamous cell carcinoma, solid adenoid cystic carcinoma, metastasis from another primary site, and medullary thyroid carcinoma. 7 Most of these conditions carry specific immunohistochemical staining and/or histologic patterns associated with the diagnosis. Appropriate classification of laryngeal tumors is important for establishing prognosis and guiding treatment. 8 Poorly differentiated laryngeal tumors tend to have a poor prognosis; however, non-LCNEC tumors like small cell neuroendocrine carcinoma (SCNEC) have lower disease specific survival compared to LCNEC (25 vs 76%). 9 Regarding treatment, high grade tumors, like LCNEC and SCNEC, are treated with multiple modalities: surgery, chemotherapy, and/or radiation therapy. 4 Lower grade tumors, like squamous cell carcinoma (SCC), are often treated with unimodal therapy like radiation therapy or endoscopic, organ-preserving resection. 10 Accurate histologic diagnosis distinguishing LCNEC from both low grade and other classically high grade tumors is critical for defining an accurate prognosis and treatment plan.
Interestingly, case reports describing large cell variants of neuroendocrine carcinoma have identified significant variability in immunohistochemical staining patterns.11-13 Some reports have shown p53 and/or p16 overexpression in cells with or without positive HPV markers, suggesting that p53 and p16 overexpression may occur from primary dysregulation rather than a HPV-mediated event.11-13 Another case report describes a laryngeal LCNEC with expression of calcitonin, the typical marker for medullary thyroid cancer, that spread aggressively within the neck. 14 In our case, we found p16 overexpression and CK34βE12 positivity within a laryngeal LCNEC. In the absence of known HPV positivity, we suspect p16 overexpression may have resulted from primary Rb dysregulation. CK34βE12 positivity is also a notable finding since this marker is typically associated with basaloid squamous cell carcinoma. Despite new classifications, it is important to acknowledge variability in laryngeal LCNECs, and the final diagnosis must account for clinical presentation, histology, and immunohistochemical features.
Conclusion
This is an unusual case of a large cell neuroendocrine carcinoma of the subglottic larynx. This case highlights the challenges in diagnosis and treatment of this rare malignancy. In addition to presenting this case, we highlight the classification and differing characteristics of neuroendocrine tumors of the larynx.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
This case was previously presented as a poster at the American Academy of Otolaryngology—HNS Meeting in September 2019.
Informed consent
Informed consent for patient information to be published in this article was not obtained because there is no identifying patient information.