
Abstract
Keywords
An 85-year-old male presented to an otolaryngology office with hoarseness, stridor, and shortness of breath. He had been evaluated by 2 outside otolaryngologists for a 4-year history of hoarseness. He was referred for consideration for speech therapy regarding hoarseness, vocal fold edema, and a questionable right vocal fold polyp. The patient reported that his symptoms had worsened progressively over the prior 6-12 months. He had no history of head and neck cancer, recent intubation, autoimmune conditions, head and neck trauma, or smoking. The patient had a history of prostate carcinoma treated with radical prostatectomy, radiation therapy, and hormone therapy 18 years prior to our initial consultation.
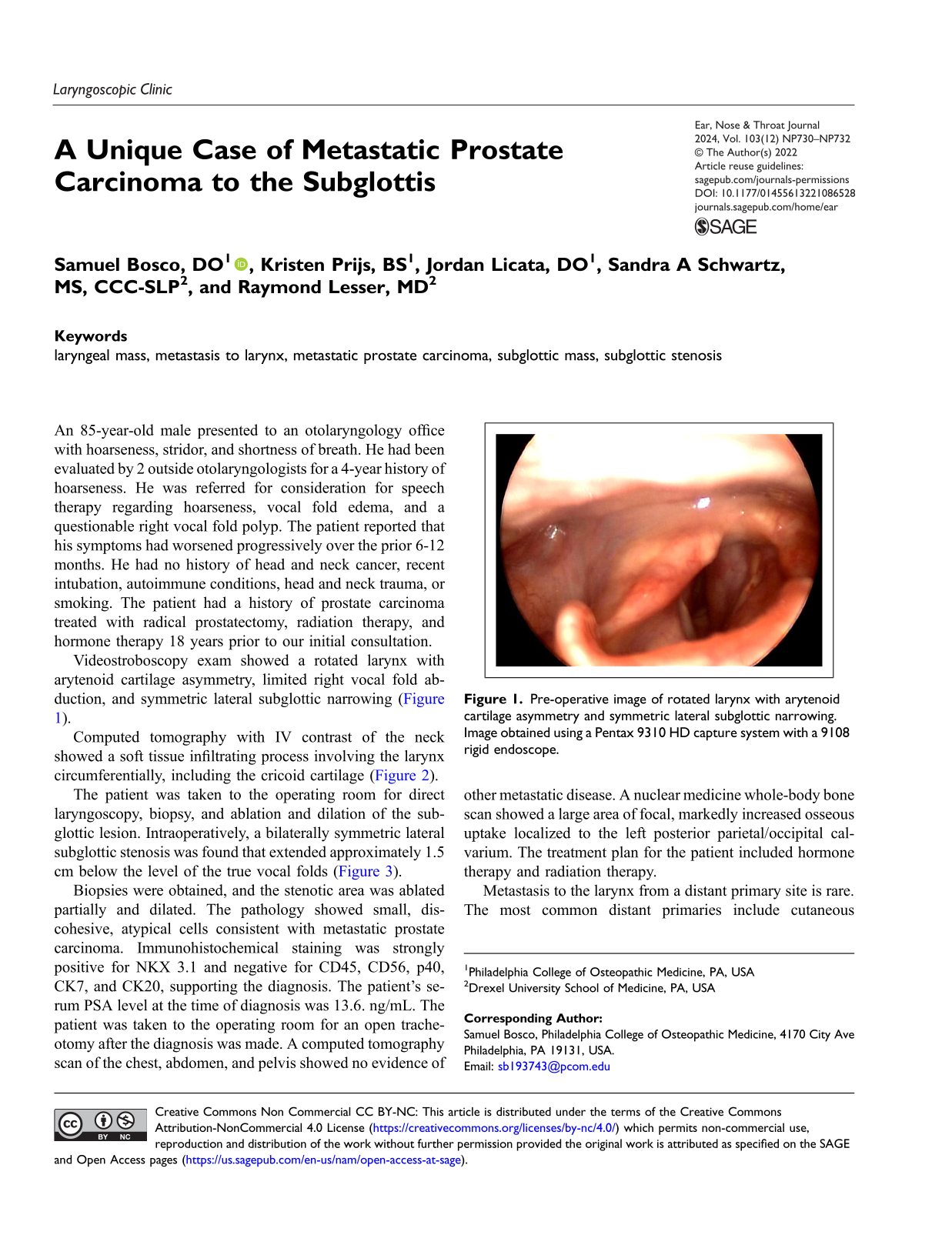
Videostroboscopy exam showed a rotated larynx with arytenoid cartilage asymmetry, limited right vocal fold abduction, and symmetric lateral subglottic narrowing (Figure 1). Pre-operative image of rotated larynx with arytenoid cartilage asymmetry and symmetric lateral subglottic narrowing. Image obtained using a Pentax 9310 HD capture system with a 9108 rigid endoscope.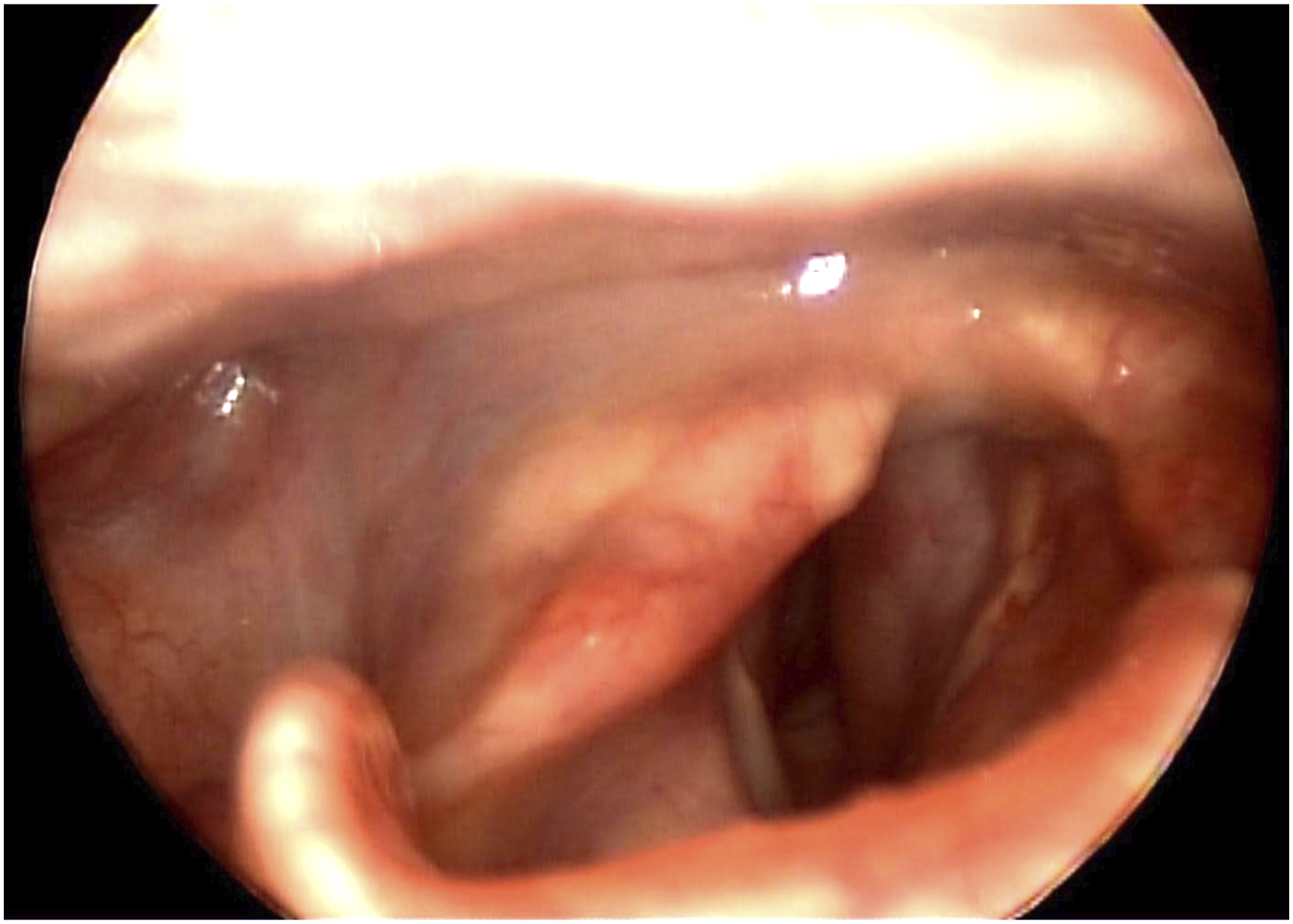
Computed tomography with IV contrast of the neck showed a soft tissue infiltrating process involving the larynx circumferentially, including the cricoid cartilage (Figure 2). Computed tomography with IV contrast of the neck in an axial plane at the level of the cricoid cartilage. (A) Subglottic mass with circumferential soft tissue fullness. (B) Bilateral cricoid cartilage sclerosis with surrounding ill-defined soft tissue margins. (C) Patchy right thyroid cartilage sclerosis, also with adjacent soft tissue haziness. (D) Right greater than left subglottic fullness with severe narrowing and leftward deviation.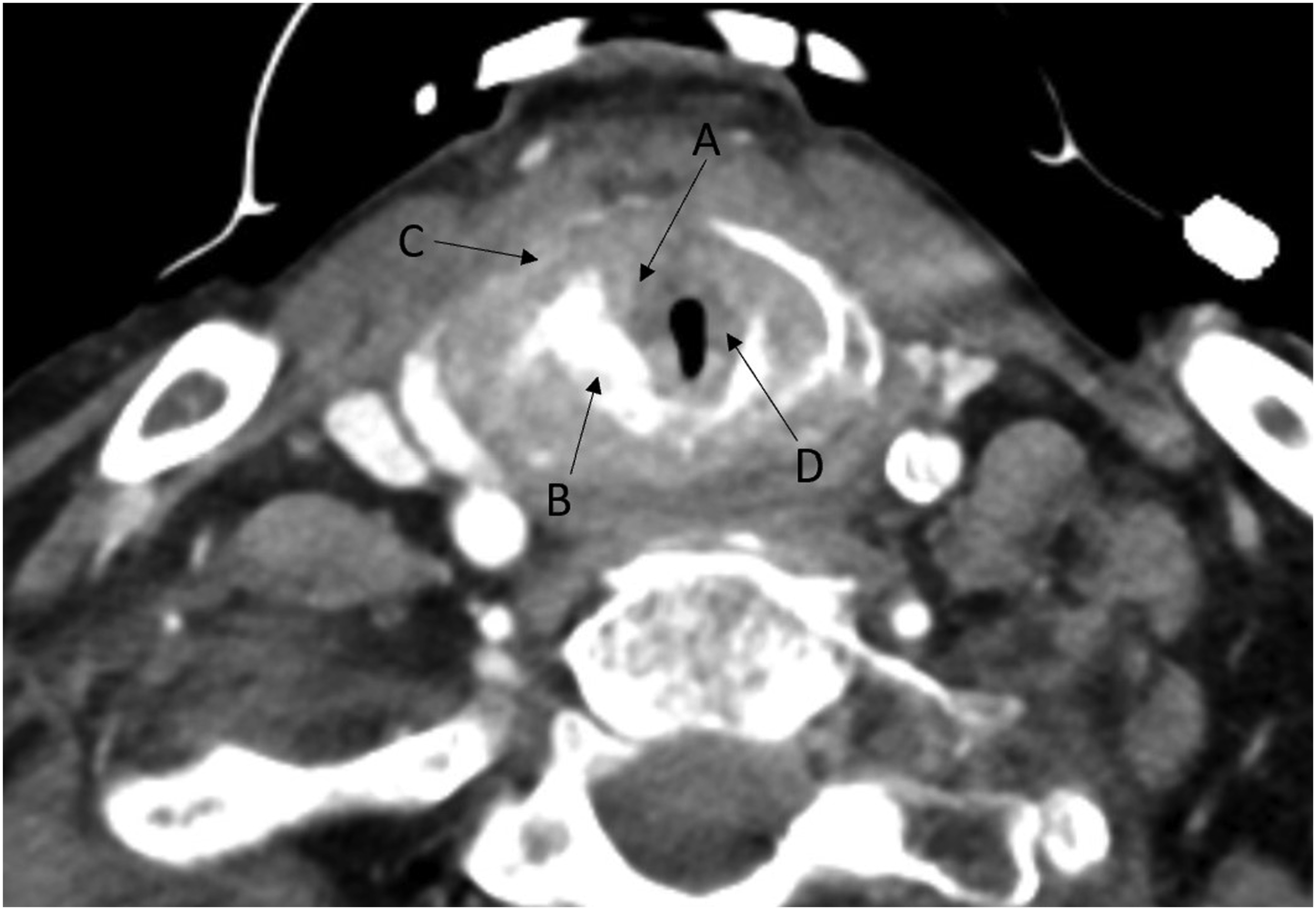
The patient was taken to the operating room for direct laryngoscopy, biopsy, and ablation and dilation of the subglottic lesion. Intraoperatively, a bilaterally symmetric lateral subglottic stenosis was found that extended approximately 1.5 cm below the level of the true vocal folds (Figure 3). Intraoperative image of larynx using a 0-degree rigid endoscope. (A) True vocal folds, (B) subglottic fullness and narrowing, and (C) endotracheal tube.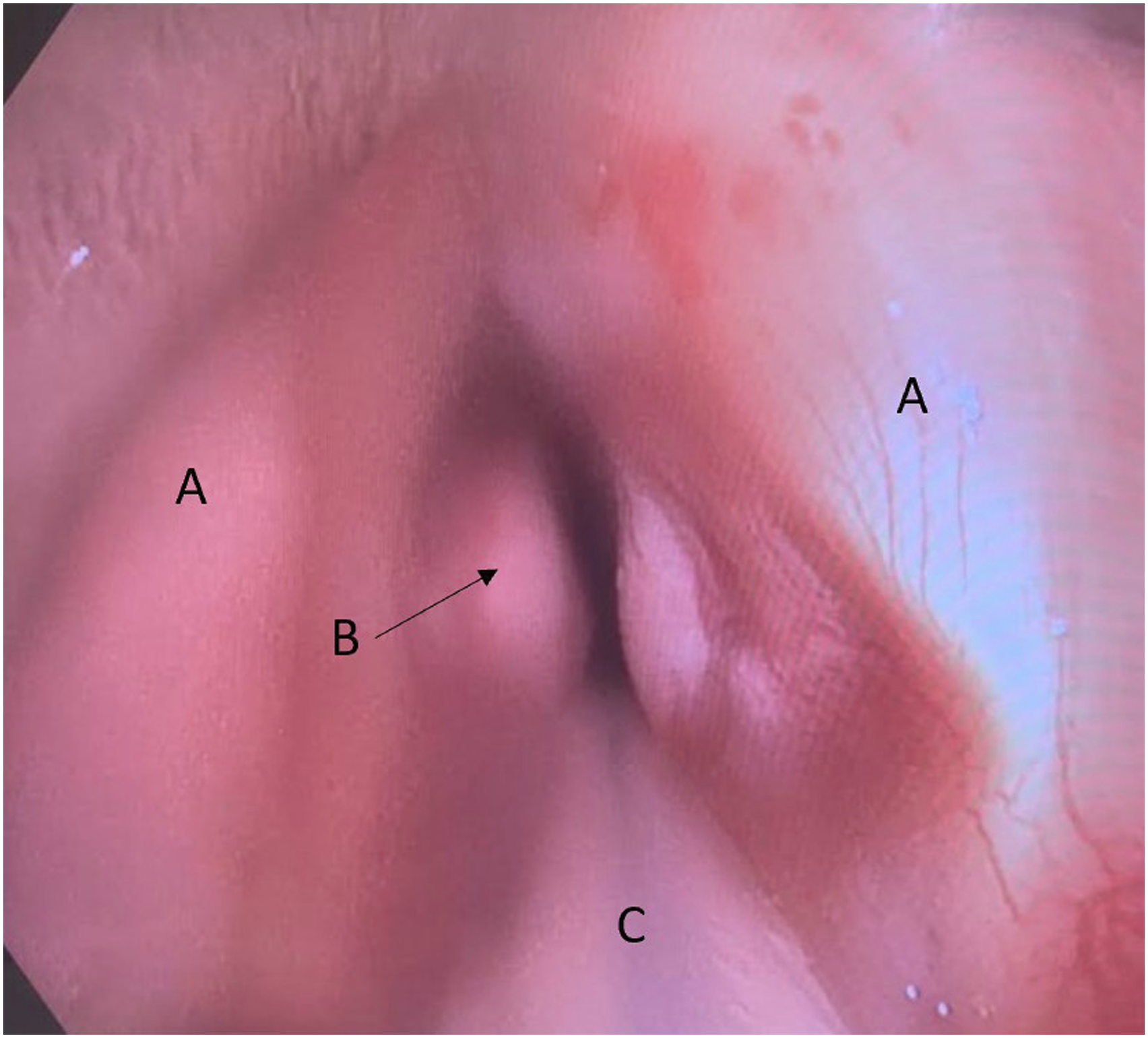
Biopsies were obtained, and the stenotic area was ablated partially and dilated. The pathology showed small, discohesive, atypical cells consistent with metastatic prostate carcinoma. Immunohistochemical staining was strongly positive for NKX 3.1 and negative for CD45, CD56, p40, CK7, and CK20, supporting the diagnosis. The patient’s serum PSA level at the time of diagnosis was 13.6. ng/mL. The patient was taken to the operating room for an open tracheotomy after the diagnosis was made. A computed tomography scan of the chest, abdomen, and pelvis showed no evidence of other metastatic disease. A nuclear medicine whole-body bone scan showed a large area of focal, markedly increased osseous uptake localized to the left posterior parietal/occipital calvarium. The treatment plan for the patient included hormone therapy and radiation therapy.
Metastasis to the larynx from a distant primary site is rare. The most common distant primaries include cutaneous melanoma and renal cell carcinoma. Metastasis to the larynx from prostate carcinoma is less common, with only 6 reported cases in the English-language literature since 1988. 1 Metastatic prostate cancer elicits osteoblastic reactions and sclerotic changes, and bone is a frequent site of spread. 2 The larynx is the least frequently reported site of metastasis of prostate carcinoma. 3 There have been a number of proposed mechanisms for spread of abdominal cancer to the larynx, including spread via interconnections between supraclavicular nodes and subglottic lymphatic vessels, and spread via the paravertebral plexuses.4,5
Metastatic prostate cancer to the larynx typically first involves the laryngeal skeleton, resulting in pathologic ossification. This often results in prolonged periods of clinical silence and may explain partially the rarity of the clinical diagnosis. It is often not until the carcinoma spreads to the soft tissues of the larynx partially that symptoms arise, including dysphagia, dyspnea and hoarseness. 6 Postmortem studies have demonstrated that the incidence of metastatic prostate cancer to the larynx is higher than clinical experience suggests, explained by frequent lack of growth and absence of symptoms.4,6,7
Diagnosis is confirmed by biopsy and immunohistochemical staining. NKX 3.1 is a highly sensitive and specific tissue marker of metastatic prostate adenocarcinoma. 8 Management of metastatic prostate carcinoma may include a combination of orchidectomy and hormone therapies, radiation therapy, and other palliative therapy. Chemotherapy trials have shown prostate cancer cells to be relatively resistant. 9 Due to the insidious and often silent nature of these metastases, by the time patients are diagnosed, their prognosis is usually poor. 1
Although rare, metastatic prostate carcinoma to the larynx should be considered in the differential diagnosis of any male over the age of 45 years presenting with a laryngeal mass involving the laryngeal skeleton, and especially in those with a history of prostate carcinoma. This case highlights the importance of performing a thorough investigation of upper airway symptoms in patients with prior malignancies. Maintaining a high index of suspicion in selected patients will facilitate more timely diagnosis and treatment. Diagnosis should be confirmed with immunohistochemical staining, and management should be determined in concert with oncologic and urologic consultation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.