
Abstract
Objective:
Accidental pharyngeal fishbone ingestion is a common complaint in ear, nose, and throat clinics. Approximately two-thirds of the accidentally ingested fishbones can be removed using tongue depressors and indirect laryngoscopy. However, the remaining third is challenging to identify and remove using these methods. These difficult fishbones require identification and removal via more advanced approaches. Video-guided laryngoscope is used to deal with difficult fishbones in our center. This study aimed to explore the risk factors for difficult fishbones.
Methods:
A prospective study was performed at a teaching hospital on 2080 patients. Univariate and multivariate analyses were performed to identify the risk factors.
Results:
The common fishbone locations were the tonsils (39.8%; defined as STEP-I), tongue base (37.1%), vallecula (13.3%; STEP-II), and hypopharynx (9.8%; STEP-III). With increasing STEP level, the ratio of difficult fishbones correspondingly increased (Z = 13.919, P < .001), and the proportions were 21.1%, 41.9%, and 70% in STEP-I, II, and III, respectively. In particular, fishbones in STEP-III (vs STEP-I) had a higher risk of difficult fishbones (odds ratio [OR]: 11.573, 95% CI: 7.987-16.769). Complaints of neck pain (yes vs no), foreign body sensation (yes vs no), and shorter length of fishbones always had a lower risk of difficult fishbones (OR: 0.455, 95% CI: 0.367-0.564; OR: 0.284, 95% CI: 0.191-0.422; OR: 0.727, 95% CI: 0.622-0.85). Missing teeth (yes vs no), swallowing behavior after fishbone ingestion (yes vs no), and male patients (vs female) had a higher risk of difficult fishbones (OR: 1.9, 95% CI: 1.47-2.456; OR: 1.631, 95% CI: 1.293-2.059; OR: 1.278, 95% CI: 1.047-1.56).
Conclusions:
Neck pain, foreign body sensation, fishbone length, patient age and sex, tooth status, and swallowing behavior after fishbone ingestion are independent risk factors for difficult fishbones.
Keywords
Introduction
Accidental fishbone ingestion is one of the most common causes of foreign bodies in the pharynx. 1 Some fishbones are complicated to remove as they are difficult to locate. A few studies have been conducted to assess the factors that help to locate fishbones. 2,3 However, the characteristics of such fishbones are seldom mentioned. These fishbones always require identification and removal by more advanced approaches. In the author’s center, 36.4% of fishbones that could not be located by utilizing tongue depressors and indirect laryngoscopy examinations were detected by video laryngoscopy examination. We defined these as difficult fishbones. This study aimed to explore the risk factors of difficult fishbones by univariate and multivariate analyses.
Patients and Methods
Participants
This prospective study was conducted in the emergency department of the hospital specializing in otolaryngology and eye diseases in China in 2015. The inclusion criteria included patients who complained of “accidental fishbone ingestion,” in whom the fishbones were detected and removed from the pharynx.
The exclusion criterion was the fishbones in the esophagus (proven by computed tomography scan). The questionnaire was completed by the doctors. The variables assessed in the questionnaire included the patients’ sex, age, missing teeth and dentures, clinical symptoms, the type of fishbone, the length of the fishbone, talking or laughing during eating, swallowing behavior after fishbone ingestion, location, methods of fishbone removal, and frequency of fishbone ingestion within 3 years. The study protocol was approved by the Ethics Committee of the Eye, Ear, Nose, and Throat Hospital, Fudan University (approval number: 2015038).
Variables Definition
The binary dependent variable was difficult for fishbones. The “difficult fishbone group” was defined as fishbone removal under video-guided laryngoscope, and the “no difficult fishbone group” was defined as fishbone removal using tongue depressors and indirect laryngoscopy.
Fishbone length and patient’s age were continuous variables. Variables such as neck pain, foreign body sensation, swallowing behavior after fishbone ingestion, dentures, missing teeth, and talking or laughing during eating fish were defined binary variables. The time of fishbone ingestion was a continuous variable divided into ≤7 days and >7 days.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation for normally distributed variables and as medians (interquartile ranges) for variables that followed a nonparametric distribution. Categorical variables were compared using the χ2 test. Quantitative continuous variables were compared using nonparametric tests for non-normally distributed variables. The χ2 goodness-of-fit test was used to compare frequency distribution differences. Bonferroni correction was applied, as noted for multiple comparison corrections. When analyzing the trends of binary variables with grade variables, the χ2 trend (Cochran-Armitage) test (CATT package in R language) was used. Univariate and multivariate analyses were performed using a binary logistic regression model.
Statistical significance was set at P < .05. IBM SPSS for Windows (version 22.0; IBM Corp) was used for the analyses. The effect size was calculated using the R language with the “pwr” package.
Results
STEP Anatomical Division
A total of 2080 patients diagnosed with accidental pharyngeal fishbone ingestion were included. The patients’ mean age was 50 (34-60) years, and the maximum and minimum ages were 92 and 11 years, respectively. We designated the locations of the fishbones in the tonsils as STEP-I (39.8%), tongue base and vallecula as STEP-II (50.4%), and hypopharyngeal as STEP-III (9.8%; Figure 1A). The tonsils were divided into the upper, lower, anterior, and posterior surfaces (Figure 1B). The anatomical locations of the ingested fishbones in the hypopharynx were subdivided into the piriform fossa, hypopharyngeal lateral wall, postcricoid region, and posterior pharyngeal wall.
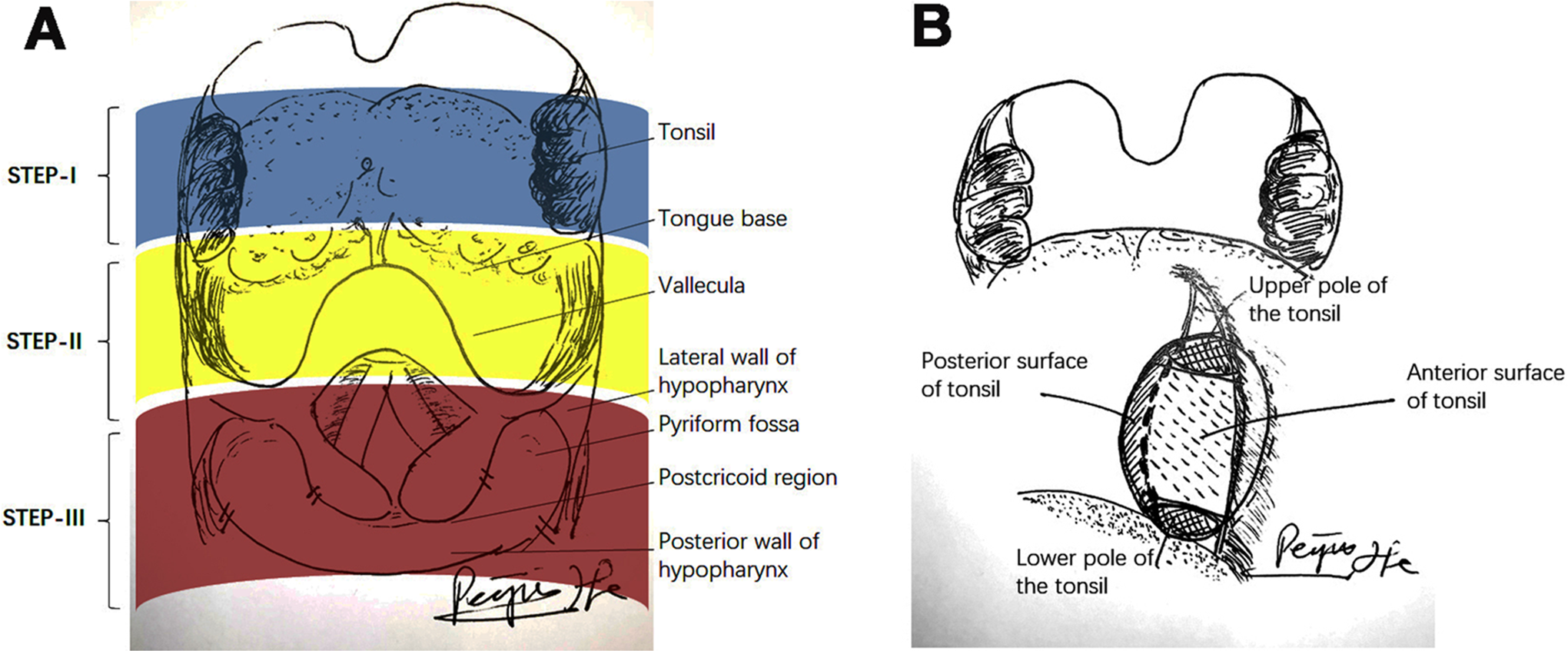
A, Level of anatomy: STEP-I tonsil, STEP-II tongue base, and STEP-III hypopharynx. B, Schematic diagram shows the upper and lower pole and anterior and posterior surface of tonsil.
Risk factors of Difficult Fishbone Analysis
Univariate analysis of difficult fishbone analysis
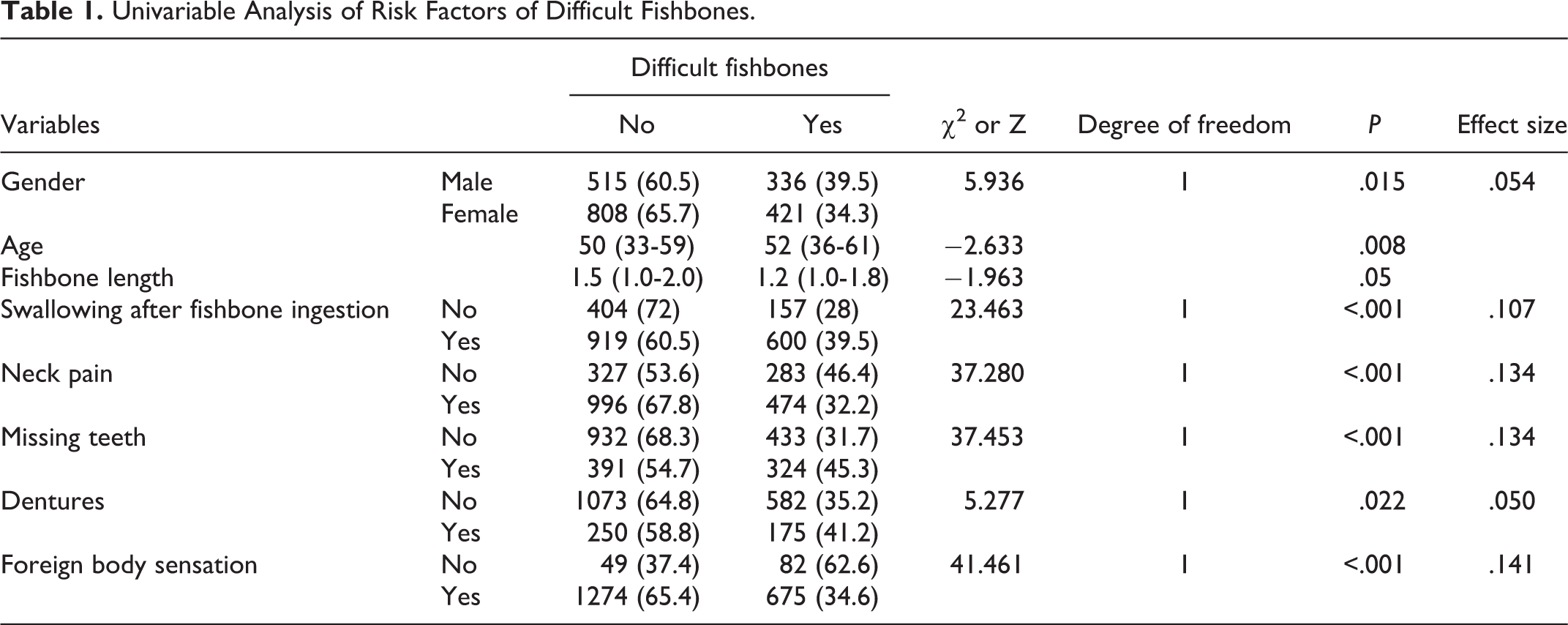
The clinical characteristics were different between the video-guided and nonvideo-guided laryngoscope groups (Table 1). The proportion of male patients was higher (P = .015) in the former than that in the latter group. Compared with the latter group, the patients were older (P = .008), and correspondingly, the proportion of missing teeth and dentures was higher (P < .001, P = .022) in the laryngoscope group. A higher ratio of swallowing behavior after fishbone ingestion was found in the former than in the latter group. Swallowing behavior after fishbone ingestion was correlated with a higher ratio of video-guided laryngoscopy (P < .001), and a lower ratio of neck pain and foreign body sensation was observed in the video-guided laryngoscope than in the other group (P < .001).
Univariable Analysis of Risk Factors of Difficult Fishbones.
The necessity for fishbone removal using a video-guided laryngoscope differs from the anatomical distribution of the fishbones (χ2 = 195.989, degree of freedom = 2, P < .001, effect size = 0.307). In general, as the fishbones’ ingestion location became deeper, the removal proportion using the video-guided laryngoscope assistance was also increased (Z = 13.919, P < .001), and the proportions were 21.1%, 41.9%, and 70% in STEP-I, STEP-II, and STEP-III, respectively. The removal rate was high at specific anatomic locations. For the fishbones in STEP-I, we observed that the fishbones in the tonsil’s posterior surface were the most difficult to remove, and 40.4% of them were removed with video-guided laryngoscope assistance (Figure 2A). Moreover, for the fishbones in STEP III, particularly in the pyriform fossa, 83.3% of the bones were removed with the assistance of a video-guided laryngoscope, respectively. The bones in the vallecula and tongue base were relatively easy to remove (Figure 2B).
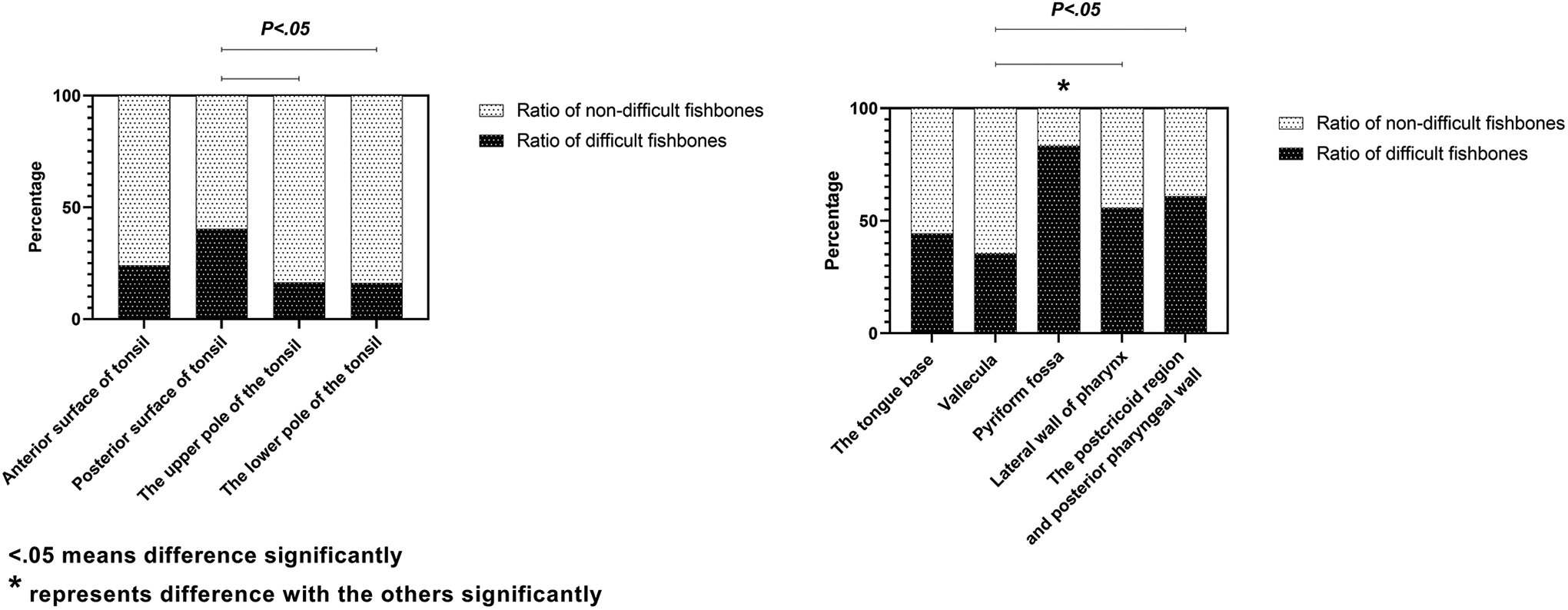
A, The ratio of fishbones removal with the video-guided laryngoscope assistance in sublocations of STEP-I. B, The ratio of fishbones removal with the video-guided laryngoscope assistance in sublocations of STEP-II and STEP-III.
Multivariate analysis of risk factors of difficult fishbones
Multivariate analysis revealed sex, swallowing behavior after fishbone ingestion, missing teeth, STEP, fishbone length, neck pain, and foreign body sensation as independent risk factors for difficult fishbones (Figure 3). Complaints of neck pain (yes vs no; odds ratio [OR]: 0.455, 95% CI: 0.367-0.564), foreign body sensation (yes vs no; OR: 0.284, 95% CI: 0.191-0.422), and shorter length of fishbones (OR: 0.727, 95% CI: 0.622-0.85) produced a lower risk of difficult fishbones. Sex (male vs female; OR: 1.278, 95% CI: 1.047-1.56), swallowing behavior after fishbone ingestion (yes vs no; OR: 1.631, 95% CI: 1.293-2.059), missing teeth (yes vs no; OR: 1.9, 95% CI: 1.47-2.456), and STEP-II-III (vs STEP-I) had a higher risk of fishbone difficulty. The fishbone in STEP-III was often challenging to detect and remove and require the assistance of a laryngoscope (OR: 11.573, 95% CI: 7.987-16.769).
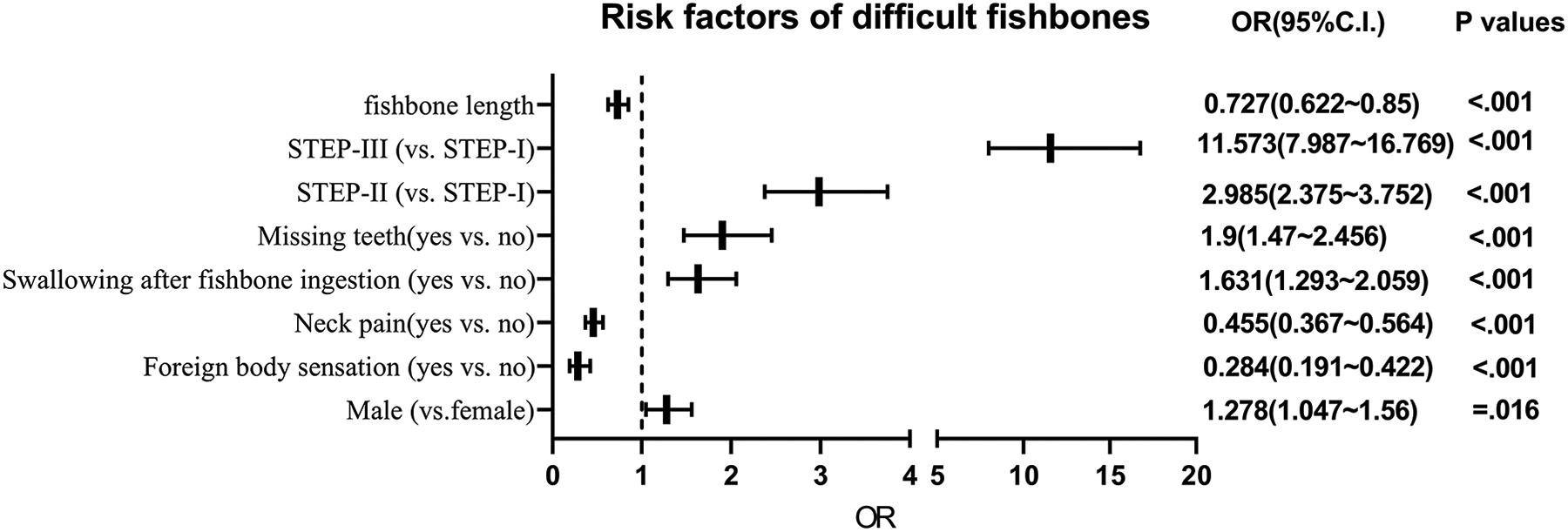
Multivariable analysis of risk factors of difficult fishbones.
Discussion
Main Results of This Study
Based on the anatomical location of fishbone ingestion, the STEP level method was first proposed, which simplified the complicated locations and assisted in exploring the relationship between the fishbone location and clinical data. STEP, missing teeth, swallow behavior, sex, fishbone length, neck pain, and foreign body sensation were proven as independent risk factors for difficult fishbones. Additionally, the fishbones in STEP-I, those lodged in the posterior surface of the tonsil, were the most challenging to identify and remove. For all regions, the fishbones in the pyriform were the most difficult to identify and remove.
STEP Division in the Pharynx
To the best of our knowledge, this study was the first to divide the ingested fishbone positions into 3 levels: STEP-I, STEP-II, and STEP-III, for subsequent analysis. As the STEP level increased, the difficulty of fishbone removal also increased. The fishbones in STEP-I accounted for 39.8%, of which the fishbones on the posterior side of the tonsils were the most difficult to remove; fishbones in STEP-II accounted for 50.4%; fishbones in STEP-III accounted for 9.8%, and 70% of them needed to be removed with the assistance of a video-guided laryngoscope. This stratification simplified the complicated anatomy, which was helpful for the clinical analysis and exploration of rules.
Risk Factors of Difficult Fishbones
The proportion of difficult fishbones increased with STEP levels. Swallowing behavior may bring the fishbone to deeper parts, making it more challenging to remove the fishbone. It has been reported that patients younger than 10 years have a higher risk of having fishbones lodged in the tonsils, 2 resulting from the hypertrophy of tonsils in adolescents. Atrophy of tonsils and missing teeth and dentures 3 in elderly patients may be risk factors for fishbones lodged in STEP-II and STEP-III. Additionally, the locations of patients’ neck pain or pharyngeal foreign body sensation were associated with the ingested fishbone location. 4 In our study, the proportion of pharyngeal pain and foreign body sensation in difficult fishbones group was much lower than that in nondifficult fishbone group; therefore, the accurate fishbone could not be detected using the location of pharyngeal pain and foreign body sensation. Therefore, this may elucidate why the locations of neck pain were weakly related to the location of the foreign body in the throat. 5
Advantage of Fishbone Removal Using the Video-Guided Laryngoscope
Most fishbones can be removed using a tongue depressor, indirect laryngoscope, forceps, or angled forceps. 6 However, some fishbones are difficult to remove using these methods and require identification and removal via more advanced approaches. In this center, the video-guided laryngoscope was used, which can provide a good and stable field of vision, indicate the location of fishbones, and improve the detection and removal rate of fishbones. 1,7,8 The laryngoscope provides a magnified image of short fishbones 1 and can provide stable images even in some male patients with a high tongue base and heavy pharyngeal reflex. Among the fishbones in STEP-II and STEP-III, those in the pyriform had the highest removal rate under the video-guided laryngoscope. The laryngoscope has the advantage of removing the fishbones in the pyriform. 9 -11 Among the fishbones in STEP-I, those on the posterior side of the tonsils are difficult to identify and remove, and a video-guided laryngoscope can provide adequate vision.
Conclusions
Neck pain and foreign body sensation, fishbone length, patient’s age and sex, tooth status, and swallowing behavior after fishbone ingestion are all independent risk factors for difficult fishbones.
Footnotes
Authors’ Note
This study was approved by the Ethics Committee of Eye, Ear, Nose, Throat Hospital of Fudan University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Science and Technology Commission of Shanghai Municipality (CN) [grant number 19ZR1408100]; Science and Technology Commission of Shanghai Municipality of China (grant number 20Y11901900); Health and Family Planning Commission of Shanghai Municipality of China (grant number 2019SY059).