
Abstract
Angiomyolipoma is a benign, mesenchymal, hamartomatous lesion often described in the kidney and may be associated with tuberous sclerosis. Nasal angiomyolipoma is an extremely rare tumor with fewer than 20 cases reported in the literature. We report a case of angiomyolipoma arising in the right nasal vestibule in a 68-year-old male with mild, recurrent right-sided epistaxis, and nasal obstruction. With the exception of arterial hypertension, the patient did not have any comorbidities. Gross examination showed a well-circumscribed, lobulated mass. On the microscopic level, it was composed of mature smooth muscle cells, thick-walled blood vessels of varying sizes, and islands of mature adipose tissue. Angiomyolipoma should be considered as a differential diagnosis for unilateral nasal masses, especially those situated in the nasal vestibule.
Introduction
Angiomyolipoma is a benign, vascular, mesenchymal hamartomatous tumor, composed of blood vessels, smooth muscle cells, and mature adipose tissue. 1 This lesion most commonly occurs in the kidney. Less commonly, it can be found in the gastrointestinal tract, liver, adrenal gland, lung, heart, oropharynx, and skin. 1,2 Nasal cavity and paranasal sinuses are extremely rare sites of primary localization of angiomyolipoma and only 19 cases of nasal origin have been reported in the literature. 1,2 We present a case of a patient with angiomyolipoma arising from the right nasal vestibule.
Case Presentation
A 68-year-old male presented with mild, spontaneous, recurrent right-sided epistaxis, and nasal obstruction for 7 months. Rhinoscopy revealed a round, red and smooth surface lesion in the lateral part of the right nasal vestibule. The patient did not have comorbidities other than arterial hypertension. A computed tomography (CT) scan showed a 15 × 10 mm well-vascularized mass of soft tissue, arising from the right lateral nasal vestibule, without signs of bone erosion (Figure 1). After the surgical excision and separation from the skin ellipse, gross examination demonstrated a tan-pink, lobulated, and partly hemorrhagic round soft tissue lesion that measured 14 × 10 × 9 mm. Histopathological analysis showed no surface epithelial lining in the lesion. The mass was well-circumscribed and contained an admixture of thick-walled blood vessels of varying sizes, islands of adipose tissue, and mature spindled smooth muscle cells. There were no signs of cell atypia in the lesion (Figure 2A and B). Immunohistochemical analysis showed diffuse smooth muscle actin positivity while the melanocytic marker HMB-45 was negative. Follow-up at 6 and 12 months showed no evidence of residual and/or recurrent disease.
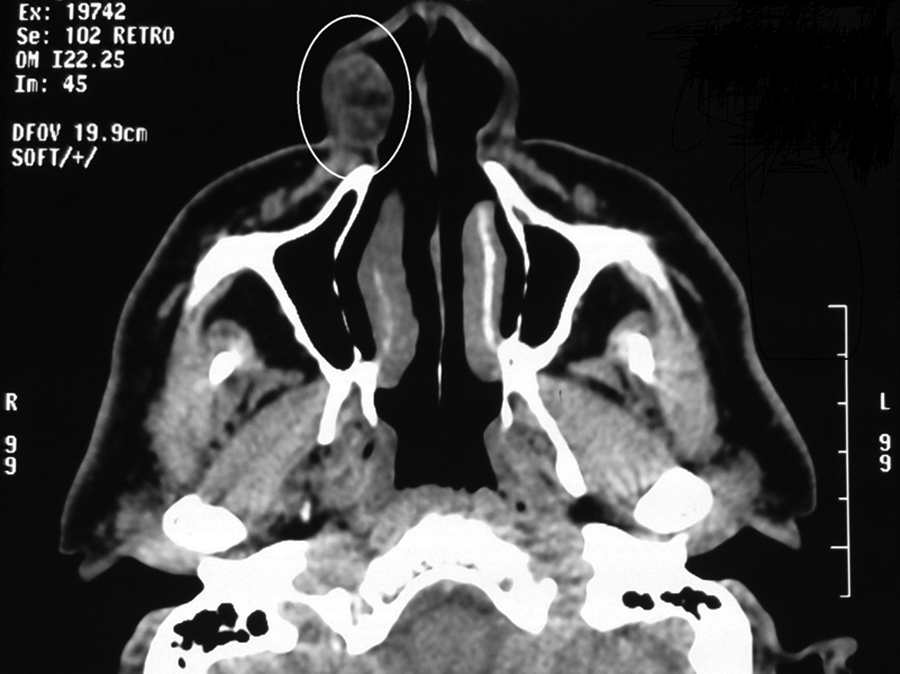
Computed tomography (CT) scan showing a soft tissue, well-vascularized mass, arising from the right lateral nasal vestibule, with dimensions of 15 × 10 mm, without signs of bone erosion.
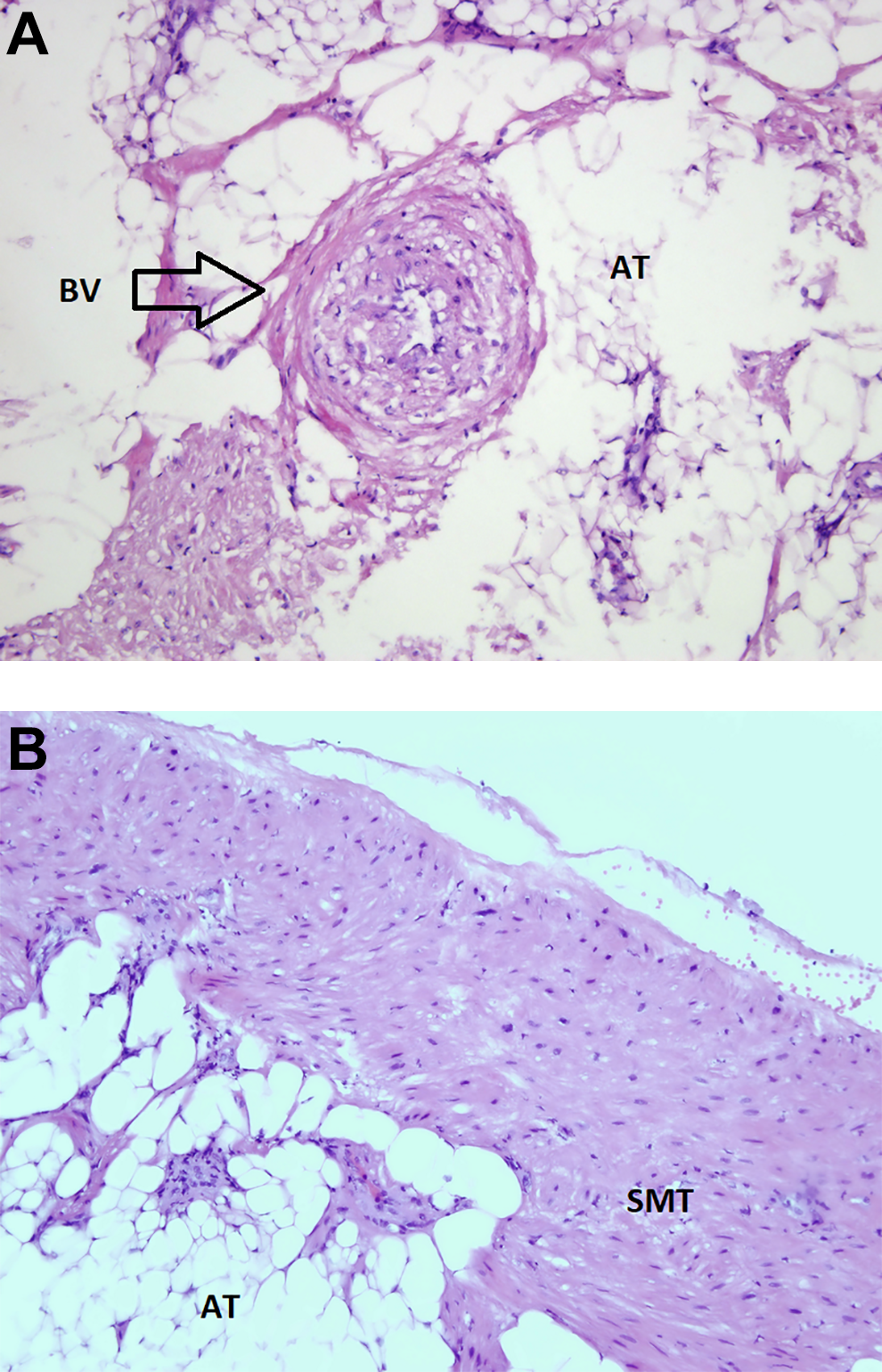
Histopathological analysis showing the presence of varying-sized thick-walled blood vessels (arrowhead), islands of mature adipose tissue (A) and mature, spindled smooth muscle cells, without signs of atypia (B). AT indicates adipose tissue; BV, blood vessels; SMT, smooth muscle tissue (hematoxylin & eosin staining, magnification ×200).
Discussion
Vascular tumors of the nasal cavity and paranasal sinuses are relatively rare. The best known is angiofibroma, but lobular capillary and cavernous hemangioma, hemangiopericytoma, and angioleiomyoma can also be found in the medical literature. 1,2 In this article, we describe an extremely rare vascular hamartomatous tumor originating from the nasal vestibule. Only 5 similar cases had previously been reported. 1 -5 Angiomyolipoma represents a part of the group of perivascular epithelioid cell tumors (PEComas) including histologically similar lesions occurring in a variety of cutaneous, visceral, and soft tissue sites. 6 Although angiomyolipoma is a benign lesion, there is evidence in the literature of malignant transformation of angiomyolipoma primarily localized in the kidney and liver. 7,8 This rare tumor may appear as a sporadic lesion or associated with a tuberous sclerosis complex. Tuberous sclerosis is associated with about 20% of renal and about 15% of hepatic angiomyolipomas. 9,10
About 80% of patients with nasal angiomyolipoma are male and between 29 and 88 years of age. 1 -5 Watanabe and Suzuki proposed the classification of angiomyolipomas into 2 clinicopathological types: the mucocutaneous type, originating from the skin, nasal cavity, oropharynx, and larynx, and the hepatorenal (PEComatous) type. 11 Histopathologically, the mucocutaneous type is composed of spindled and mature smooth muscle cells, has no epithelioid morphology, and, as was the case with our patient’s tumor demonstrates no immunoreactivity to the melanocytic marker HMB-45. In contrast, in the hepatorenal type, smooth muscle cells are usually epithelioid and positive to melanocytic markers. 11 Clinically, the mucocutaneous type of angiomyolipoma is different from the hepatorenal type in that the epithelioid structure in tissue of the latter exhibits the potential for malignant transformation. 11 Fortunately, according to the most comprehensive review of the literature published by Wang et al, 1 only 2 cases of nasal angiomyolipoma had the histological characteristics of PEComatous angiomyolipoma. Finally, mucocutaneous angiomyolipoma tends to occur in older men and is not found to be associated with tuberous sclerosis, whereas hepatorenal angiomyolipoma is more frequently associated with tuberous sclerosis as a result of mutation in the TSC1 or TSC2 genes. 1,5
In the differential diagnosis of nasal angiomyolipoma, one should keep in mind the fact that this lesion is histologically a form of mesenchymal hamartoma. Accordingly, nasal chondromesenchymal hamartoma should first be considered as a benign lesion composed of mesenchymal elements including smooth muscle, adipose, and cartilaginous tissue. 12 According to some authors, the term “mucocutaneous angiomyolipoma” should be ignored, as this tumor is actually an angioleiomyoma with adipocyte differentiation. 13 D’Aguanno et al 13 found that the presence of mature adipocytes in the tissue of an otherwise typical nasal angioleiomyoma is not a rare occurrence. In fact, they argue that the term “angiomyolipoma” is incorrectly used to describe nasal angioleiomyoma with adipocyte differentiation. These authors suggest that angiomyolipoma is a completely different entity, since angiomyolipoma tissue cells express melanocytic and myogenic markers, whereas angioleiomyoma tissue has no such immunoreactivity. 13
Conclusion
Angiomyolipoma of the nasal cavity is an extremely rare benign tumor not associated with tuberous sclerosis. It is distinct from the PEComatous type of angiomyolipoma most commonly encountered in the kidney and liver. Nasal angiomyolipoma should be considered as a differential diagnosis for unilateral nasal masses, especially those situated in the nasal vestibule.
Footnotes
Author’s Note
The patient’s permission was obtained.
Acknowledgments
This investigation was conducted as a part of scientific project of the Military Medical Academy Faculty of Medicine, Belgrade, Serbia (MFVMA02/19-21/).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.