
Abstract
Hamartomas, as non-true tumors, are commonly found in the lungs, digestive tract, and kidneys, and there are few clinical reports on nasal cases. Nasal histiocytosis accompanied by lymphatic lesions is a common feature of nasal hamartoma. Three patients with nasal cavity hamartoma were treated in our department, including 1 male and 2 females, with nasal obstruction or epistaxis. The imaging (computed tomography, magnetic resonance imaging) of 2 patients showed a soft tissue mass in the nasal cavity and no erosion of bone, while in 1 patient, the imaging was inconclusive. The excised material in all patients was found to be a soft mass. The 3 cases showed the same pattern under histological examination, and all 3 patients were diagnosed with nasal cavity respiratory epithelial adenomatoid hamartoma (REAH). Nasal hamartoma is a rare disease with nonspecific clinical manifestations and imaging features and is often misdiagnosed. Only by a better understanding of this disease can the rate of correct clinical diagnosis be improved.
Background
Hamartoma was first described by Albrecht in 1904, but since then, it remains controversial whether hamartomas should be classified as true benign tumors. Some believe that hamartomas belong to the category of deformities rather than tumor lesions and that they are physiological lesions caused by the wrong combination and arrangement of normal tissues during growth and development.1-3 Since hamartomas are different from classical tumors with unlimited proliferation, metastasis, and malignant transformation, there are some difficulties in their clinical diagnosis and treatment. In addition, hamartomas have also been reported in neonates and infants, making it more difficult to clinically analyze their pathological characteristics. 4 Hamartomas often occur in the lungs, digestive tract, skin, liver, breast, hypothalamus, and kidneys but are rarely reported in the head and neck.1,5 Based on the particularity of hamartomas, they are prone to a misdiagnosis or even a failed diagnosis, especially in areas such as the nasal cavity and middle ear where they rarely occur. Standard methods in the diagnosis of hamartomas include magnetic resonance imaging (MRI), computed tomography (CT), and histopathological examinations6,7 and are the basis of a reasonable treatment plan. We report the diagnosis and treatment of 3 patients with nasal hamartoma and review the literature on the clinical diagno-sis, histopathological features, and treatment of nasal hamartoma.
Case Presentation
Case 1: A 41-year-old man presented to the local hospital due to increasing nasal obstruction and right nasal bleeding for the past 20 days. The clinical diagnosis was inverted papilloma. The patient was admitted to our hospital. Phy-sical examination revealed a yellow-white, soft mass in the right nasal cavity with superficial mucosal erosion without contact bleeding that caused the nasal septum to shift to the left. CT without contrast medium showed a unilateral mass in the right nasal cavity that prolapsed into the postnasal space and mucosal inflammation of both nasal cavities and maxillary and ethmoid sinuses (Figure 1A and B). Our initial diagnosis was chronic sinusitis and a right nasal mass. Nasal biopsy was performed under local anesthesia, and histopathological examination showed chronic inflammatory changes in the right nasal cavity with active interstitial tissue hyperplasia with mucoid degeneration (Figure 2A and B). Then, the lesion was endoscopically removed under local anesthesia. The operative specimen showed chronic inflammation of the right nasal mucosa with formation of respiratory epithelial adenomatous hamartoma (Figure 2C and D). The diagnosis of respiratory epithelial adenomatoid hamartoma (REAH) was confirmed.
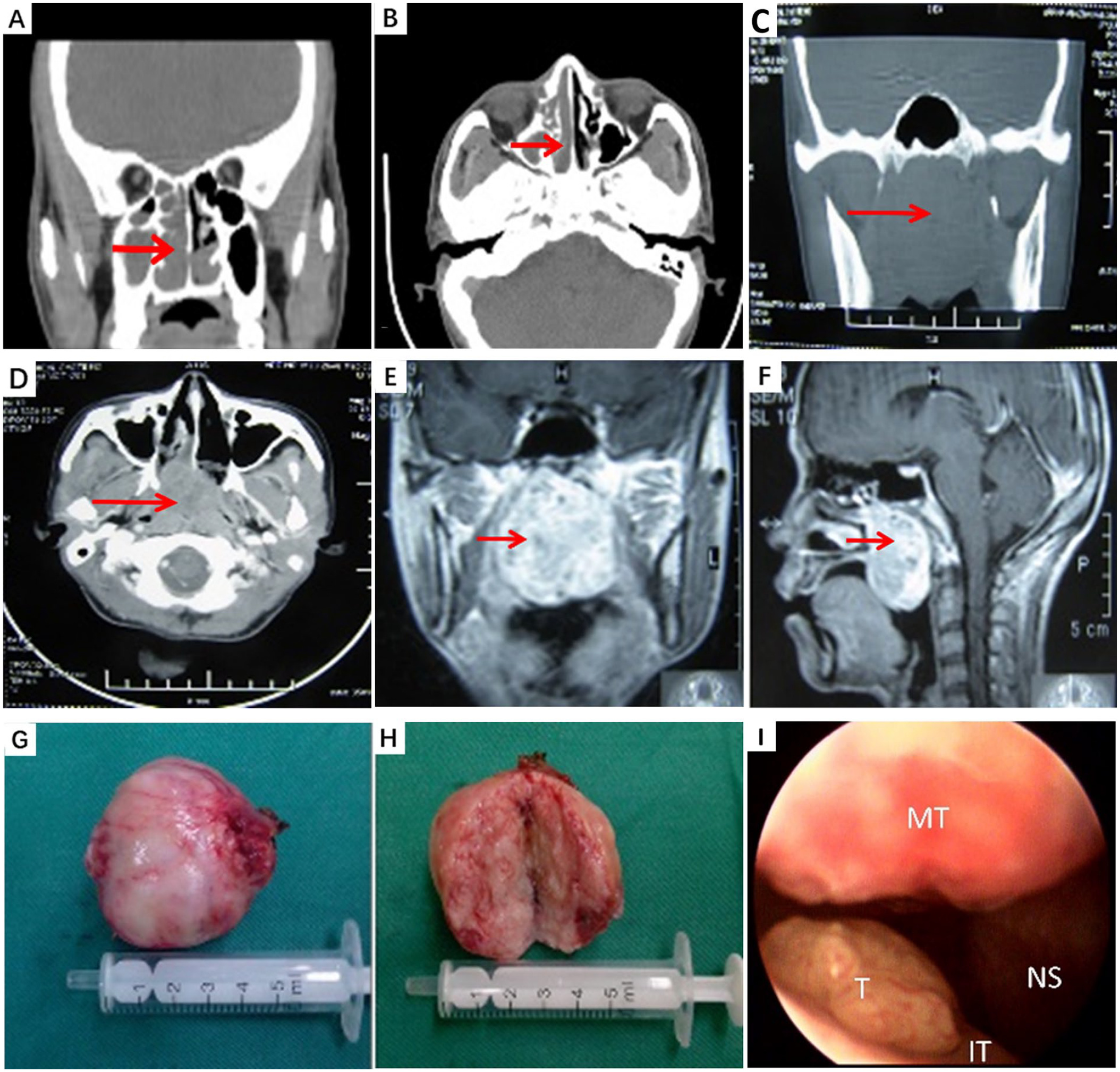
(A and B) Imaging manifestations of case 1. (C-H) Imaging manifestations and gross specimen of case 2. (I) Nasal endoscopy manifestation of case 3. Coronal (A) and Axial (B) CT demonstrate a soft tissue density mass filling out the right nasal cavity. Coronal (C) and Axial (D) CT demonstrate an oval mass filling the nasopharynx and extending into the nasal cavity. Axial (E) and Sagittal (F) MRI T2WI demonstrate an oval mass filling out the nasopharynx descending to pharynx (As indicated by the arrows). (G) and (H) Gross specimen presenting a well-circumscribed reddish mass. (I) The tumor (T) is located at the posterior part of right inferior turbinate (IT), middle turbinate (MT), nasal septum (NS).
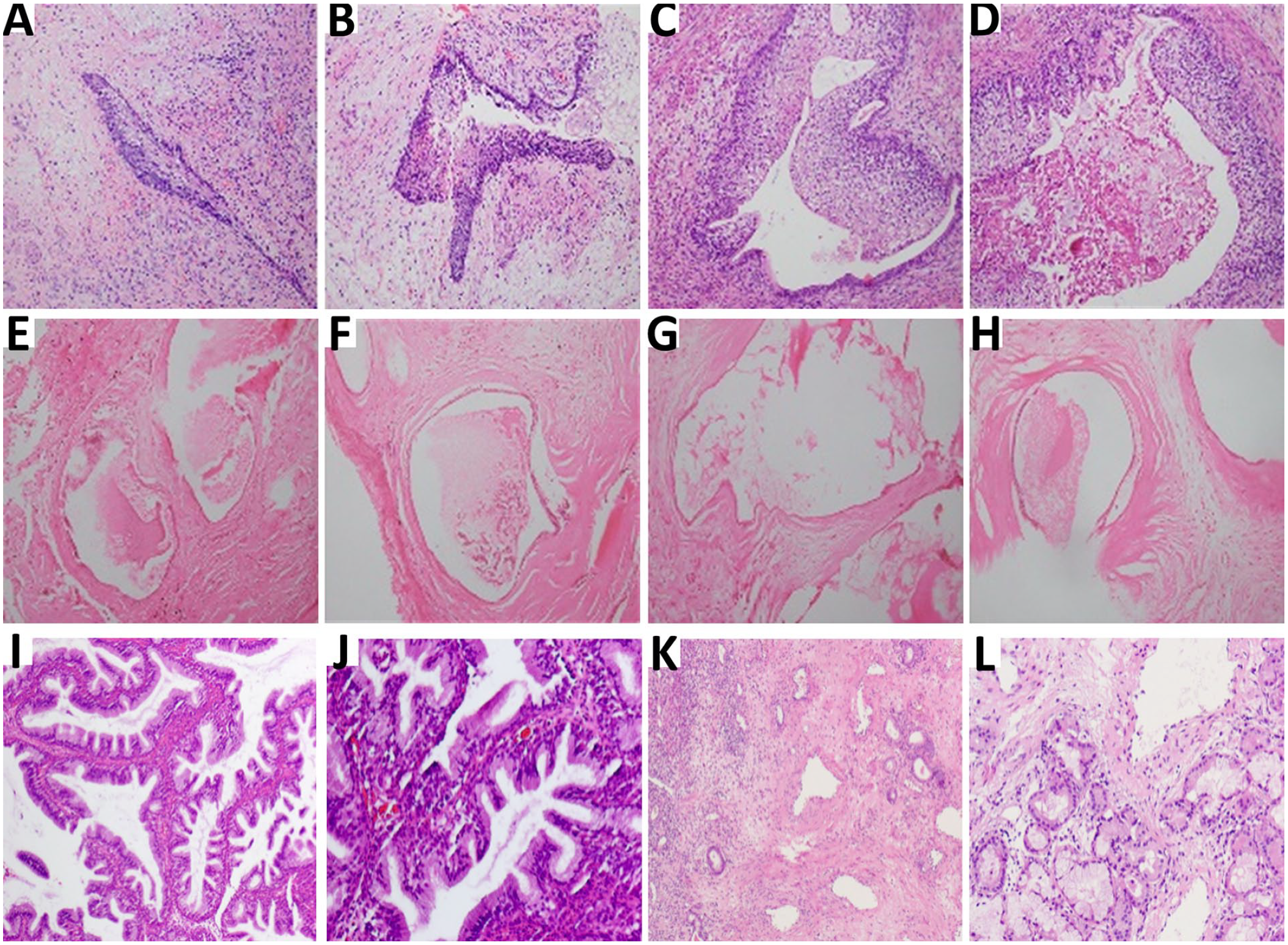
(A-D) Pathological findings of case 1. (E-H) Pathological findings of case 2. (I-L) Pathological findings of case 3. (A) and (B) Biopsy specimens show active interstitial tissue hyperplasia with mucoid degeneration. (C) and (D) Histopathology shows glands hyperplasia. The lesion is covered with pseudostratified columnar epithelium. (E) and (F) Biopsy specimens show fibrous connective tissue hyperplasia and glands dilatation. (G) and (H) Histopathology shows glandular proliferation with cystic dilatation and interstitial collagen hyperplasia. (I) and (J) Biopsy specimens show sinonasal glandular proliferation. (K) and (L) Histopathology shows glandular proliferation, composed of small to medium-sized glands separated by stromal tissue.
Case 2: A 34-year-old woman presented with an 8-year history of right nasal obstruction. There was no associated epistaxis or rhinorrhea. She had been diagnosed and treated for chronic sinusitis at a local hospital, but the symptoms were not relieved. Physical examination revealed a large, pale red and soft mass in the nasopharynx with a clear boundary and no contact bleeding. It occluded the nasopharynx and grew anteriorly to the end of the middle turbinate, down to the oropharynx. CT revealed soft tissue mass shadows and sheet-like enhancement in the nasopharynx without skull base erosion or thickening of the mucosa in the posterior wall of the nasopharynx (Figure 1C and D). MRI demonstrated a well-demarcated oval mass approximately 5 cm in diameter in the nasopharyngeal space. It showed an isointense signal on T1-weighted images and an iso- or slightly hyperintense signal on T2-weighted images. The lesions presented asymmetric hyperintensity, and there was no finding of invasion into the adjacent tissues (Figure 1E and F). Endoscopic transnasal biopsy was performed under local anesthesia. The histopathological evaluation revealed chronic inflammatory changes (Figure 2E and F). The tumor was completely excised via an endoscopic transnasal approach under local anesthesia (Figure 1G and H). The final histopathological examination revealed REAH (Figure 2G and H).
Case 3: A 53-year-old female patient was referred to our outpatient clinic presenting with repeated right nasal bleeding for 3 years, which gradually progressed. No other complaints were present. Nasal endoscopy revealed a papillary mass on the posterior part of the right inferior turbinate with smooth surface mucosa and contact bleeding (Figure 1I). An endonasal endoscopic excisional biopsy of the mass was carried out. Histopathological examination showed no malignancy, and a histopathological diagnosis of REAH was made (Figure 2I and J). An enhanced CT scan showed slight thickening in the bilateral posterior ethmoid sinus mucosa and right maxillary sinus mucosa. The tumor which was found to be located in the nasal cavity was excised via an endoscopic transnasal approach under local anesthesia. The final histopathological examination showed a benign lesion, the morphology of which was consistent with “respiratory epithelial adenomatous hamartoma changes” (Figure 2K and L).
Discussion
Hamartoma is essentially a disordered tissue induced by abnormal differentiation of the body. 8 Usually, hamartomas are different from true neoplasms. Hamartomas are by definition benign and slow-growing, and are often asymptomatic. Hamartomas can be divided into 2 types, mesenchymal and epithelial, according to their pathogenic characteristics. The incidence of epithelial hamartomas is higher than that of mesenchymal hamartomas. 9 Hamartomas can occur in various tissues and organs, among which the lungs, kidneys, and digestive tract are the most common.5,10 The head and neck region is a rarely involved site, and only a few cases have been reported. According to the literature, some authors, such as Wenig, 11 have found a subgroup of hamartomas with a high incidence in the nasal cavity or nasopharynx which is named REAH; approximately 70% of hamartomas are located in the nasal cavity. The posterior end of the septum is more commonly involved unilaterally. However, in recent years, reports in the literature have shown that REAH is more common in the nasal septum and in the olfactory cleft area, and most tumors occur bilaterally. 12 All 3 cases in our report occurred unilaterally. The pathogenesis of this subgroup is not yet clear, and most authors believe that the development of REAH involves multiple inflammatory processes.13-15 The formation of REAH is related to allergic inflammation and chronic sinusitis. In this group, 1 patient had sinusitis, and 1 patient had allergic rhinitis. It was confirmed that allergic rhinitis, sinusitis, and nasal REAH are related. The routine diagnostics for hamartoma include histopathological analysis, MRI and CT imaging. 16 Because the diagnosis of hamartoma differs among different tissue types and different stages, hamartoma is prone to misdiagnosis, underdiagnosis, and overtreatment.
Currently, an increasing number of patients with nasal respiratory epithelioid hamartoma have been reported, but there are still few patients with nasal hamartoma compared with other hamartomas, which indicates that the number of publications of nasal hamartoma is much lower than that of other hamartomas.17,18 The clinical symptoms of nasal hamartoma are nonspecific; most manifest as nasal obstruction with a decreased sense of smell and may be accompanied by different degrees of epistaxis, nasal mucus secretion or suppuration, and symptoms such as polypoid hyperplasia.19-21 Nasal hamartomas often coexist with inflammatory nasal polyps, which increases the rate of misdiagnosis. In addition, the preclinical manifestations of nasal hamartoma are not obvious, and they do not easily attract attention. Surgical resection is the routine treatment for hamartomas in clinical practice, and endoscopic surgery is the first choice for patients with confirmed nasal hamartomas. Complete surgical resection of the tumor mass is associated with a reduced risk of recurrence and a favorable prognosis.22-24 Since hamartoma of the nasal cavity is a benign lesion, it is not appropriate to expand the excision of the tissue to protect the physiological function of the nasal cavity. However, incomplete surgical resection will increase the risk of recurrence.25-27 Therefore, systematic detection and evaluation of the pathology should be carried out before surgery to establish a surgical plan. Histopathological examination and analysis must be carried out after surgery. Thus, excessive treatment can be avoided, and the risk of recurrence can be reduced. The symptoms of the patients in our series were all similar to those of chronic rhinosinusitis, as shown by the CT scan in case 1. This is also reported in the literature.13,28,29 All our patients underwent nasal endoscopic surgery. The postoperative histopathological findings in all patients support the diagnosis of nasal hamartoma corresponding to the literature. 7
Since the symptoms of nasal cavity hamartoma are very similar to chronic sinusitis, such as impaired sense of smell and nasal obstruction, there are no specific characteristics on CT and MRI. However, imaging is important for determining the extent of the pathology. The location and extent of the disease are very important to determining the treatment plan. Histopathological analysis of surgical specimens plays a major role. The morphological features of the pathological manifestations are the proliferation and accumulation of glands covered by pseudostratified ciliated epithelial cells, with the epithelial cells showing no atypical or metaplastic changes. Nasal hamartoma needs to be differentiated from inverted papilloma, nasal polyps, and adenomas. In addition, inflammatory polyps show polypoid proliferation, edema, massive fibrocytes, and vascular proliferation, which are features that help differentiate them from hamartomas.5,30,31
In summary, we reported the characteristics of 3 rare cases of nasal hamartoma. Since nasal hamartoma is easily confused with nasal polyps, chronic mucosal inflammation, inverted papilloma, and other diseases, it is easily missed and misdiagnosed. There is also some risk of overtreatment. Therefore, increased awareness of the disease in clinical practice is necessary. Patients with nasal hamartoma have the following characteristics: imaging shows unilateral or bilateral maxillary sinus, ethmoid sinus, and olfactory fissure mucosal hyperplasia and tumor-like soft tissue mass of the nasal cavity. It is believed that with the continuous improvement of diagnostic methods and additional experience with this rare pathology, the rates of misdiagnosis in nasal hamartoma will decrease, and the probability of surgical recurrence can be reduced.
Footnotes
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
We have obtained the consent and the local research ethics committee approved the study.
Consent Statement
We have obtained the consent.