
Abstract
Objectives:
To examine the success and limitations of office removal of nasal foreign bodies (FBs) in a pediatric population.
Methods:
Children presenting to an academic pediatric outpatient department were identified from a computerized collection of office notes. FB removal was performed via: (1) preprocedure discussion with shared decision-making, (2) topical anesthesia and vasoconstriction of the nose, (3) restraint in supine position with a trained second person holding the head, and (4) FB removal using an operative microscope with instrumentation. Removal was considered a failure if subsequent removal under general anesthesia was required.
Results:
Among 547 consecutive children presenting with head and neck FBs during a 22 year period, exactly 100 had nasal FBs. Forty-four percent had previous attempts at FB removal in an emergency department or pediatricians’ office. Ninety-six percent of FBs were successfully extracted in the office. Four percent required removal in the operating room. No complications were reported. Children with neurodevelopmental disorders were no more likely to experience failed removal ([0/4] vs [6/96], P = .61). The most common FBs were beads (19%), plastic (12%), and foam rubber (10%).
Concluearsion:
This protocol resulted in a high rate of successful nasal FB removal, even in children with prior failed attempts with no significant nasal injuries. This approach should be considered by otolaryngologists who care for children.
Level of Evidence:
3 – retrospective review.
Introduction
An estimated 30 000 to 40 000 children present annually to emergency departments in the United States with nasal foreign bodies (FBs). 1 While many can be removed in the primary care or emergency setting, referral to an otolaryngologist is common after failed attempts, multiple FBs, or challenging FB types such as button batteries or magnets. 2 Much attention in the literature has focused on technique, 3 choice of instrumentation, 4 and criteria for referral to an otolaryngologist especially for difficult FBs, 5 or following failed initial attempts at extraction. Less is known about the best way to manage these FBs, once the otolaryngologist is consulted.
Some authors advocate early procedural sedation or general anesthesia for these children,2,6,7 While these methods result in high rates of removal and few complications, they require specialized resources and are associated with higher costs, monitoring requirements, and procedural risks.
The senior author (G.I.) was trained to remove pediatric nasal FBs in the office setting and has employed a consistent protocol over 2 decades. We review the details of this technique and its safety and effectiveness in clinical practice and compare these results to similar published series.
Materials and Methods
Procedure
In-office FB removal followed a standardized protocol:
A complete head and neck history and physical examination were performed, with anterior rhinoscopy used to identify the FB and assess for mucosal trauma from prior attempts.
Pre-procedure discussion with the child and caregivers emphasized the brief nature of the restraint and the potential need for a second attempt in the OR if unsuccessful.
A mixture of topical lidocaine (2%) and oxymetazoline (0.025%) was applied to the children’s noses, either with an atomizer (prior to COVID-19) or a saturated wad of cotton to achieve topical anesthesia and vasoconstriction.
Most children were placed supine on an examination table in a Velcro papoose or with a parent securing the wrists.
A trained nurse or medical assistant stabilized the child’s head throughout the procedure (Figure 1).
Removal was performed under direct binocular vision with an operating microscope. Instruments included right-angle hooks for smooth spherical FBs (Figure 2A and B), alligator forceps or bayonet forceps for soft or irregularly shaped objects, and suction for friable or moist FBs. We did not use positive-pressure exhalation (Mother’s kiss) or balloon catheter extraction.

Child restrained in supine position using the combination of a papoose and head control by an assistant.
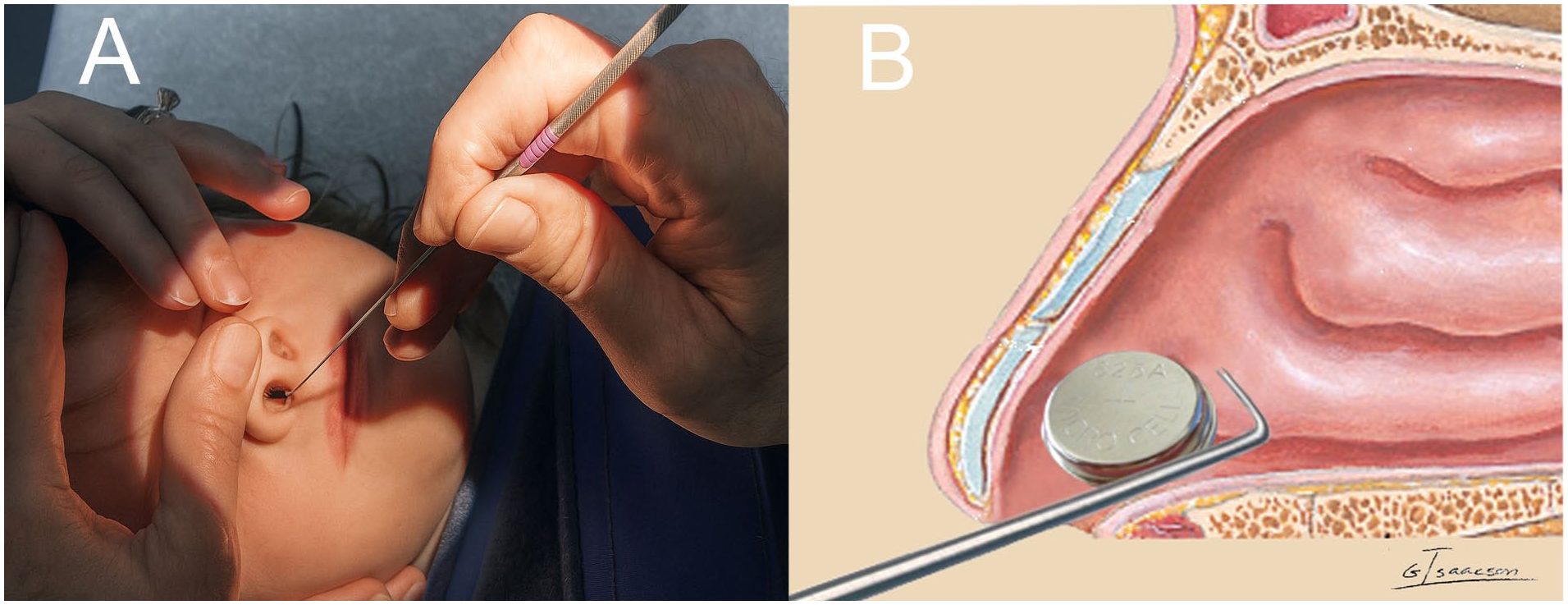
(A) Direct visualization with an operating microscope. The surgeon’s hands are free to allow exposure and removal of the FB. (B) A right-angle Gross hook is passed beyond the FB to facilitate removal. FB, foreign body.
Data Collection and Analysis
This minimal risk retrospective study was approved by the Temple University IRB (protocol 31341). The senior author’s collection of office notes and operative reports from 2001 to 2023 was queried using the Find feature of Microsoft Word®. Keywords included “bead,” “body + remove,” “button + battery,” “foreign body + microscope,” “foreign,” “insect,” “magnet,” “putty,” and “wood + remove.” Collected variables included patient age, sex, behavioral comorbidities, FB type, success of removal, and complications.
Failure was defined as the need for removal under sedation or general anesthesia. Statistical analysis was performed using chi-square tests with significance set at P < .05.
Results
Success Rate, Complications, and Reasons for Unsuccessful Removal
Among 547 consecutive children presenting with head and neck FBs during the 22 year period, exactly 100 had nasal FBs. Forty-four out of 100 (44%) had previous failed removal attempts in a pediatrician’s office, urgent care center, or emergency department (Figure 3A). Ninety-six out of 100 (96%) were successfully removed in our office. Four out of 100 (4%) required removal under anesthesia (Figure 3B). No major complications occurred such as septal perforations, retained FBs, or significant infections.
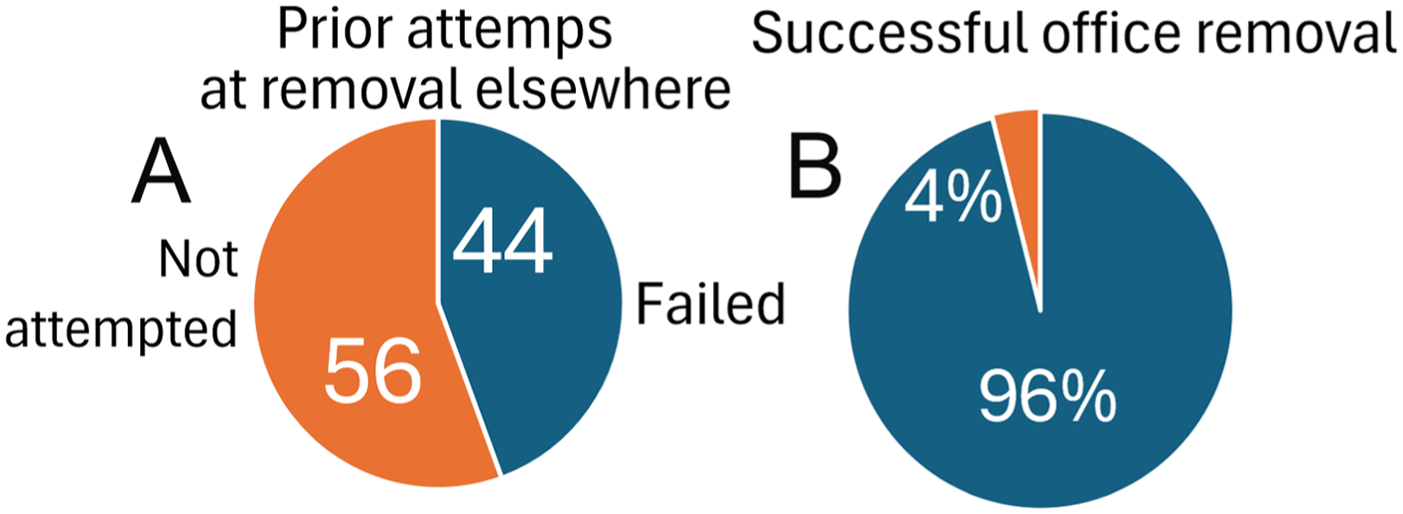
(A) Forty-four out of 100 (44%) had previous failed removal attempts in a pediatrician’s office, urgent care center, or emergency department. (B) Ninety-six out of 100 (96%) were successfully removed in our office. Four out of 100 (4%) required removal under anesthesia.
Among the 4 FBs that could not be removed, 3 were impacted (2 beads) or hooked (1 vegetable stem) in the posterior nasal cavity or choana. One child would not tolerate any nasal manipulation.
FB Type
The most common FBs were beads (19%), pieces of plastic (12%), and foam rubber (10%). Other FBs of lower frequency included toys (Lego®, GI Joe statue, plastic heart, Play-doh®), vegetative FBs (carrot, popcorn, cherry pit, peanuts, seeds), household items (paper, cotton, pipe cleaner, rubber bands, coin). A single button battery and a pair of high-power magnets were removed. There were no chronic rhinoliths, insects, or other live foreign bodies in the series (Figure 4).
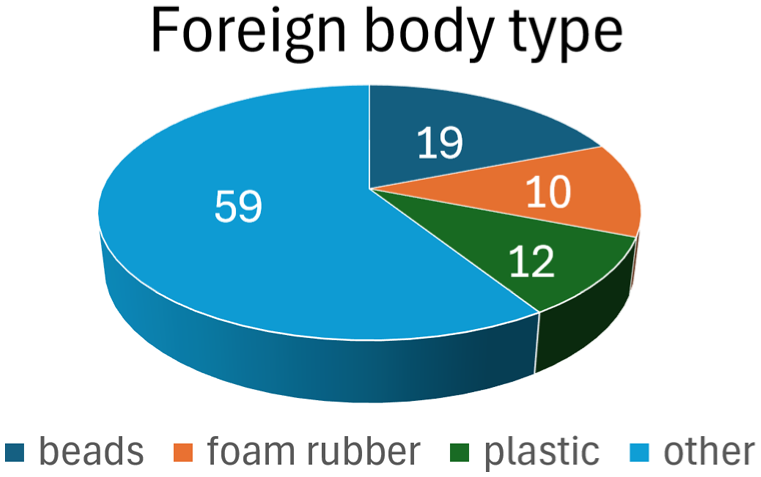
Foreign body types. The most common FBs were beads (19%), pieces of plastic (12%), and foam rubber (10%). Other FBs of lower frequency included toys (Lego®, GI Joe statue, plastic heart, Play-doh®), vegetative FBs (carrot, popcorn, cherry pit, peanuts, seeds), household items (paper, cotton, pipe cleaner, rubber bands, coin).
Demographics
Age
Within the successful removal group, the mean age was 3.7 years (median 3 years, range 1-15 years). Within the unsuccessful removal group, the mean age was 3.5 years (median 3.5 years, range 3-5 years). The 2 groups were not statistically different in age (P = .89).
Sex
The successful removal group was 51% male and 49% female. The unsuccessful removal group was 25% male and 75% female. While these proportions appear different, they are not statistically distinct (P = .61).
Neurodevelopmental disorders
In the successful removal group, 6/96 (6%) of patients had a documented diagnosis of autism spectrum disorder or attention-deficit hyperactivity disorder. In the unsuccessful removal group, 0/4 of patients were diagnosed with autism spectrum disorder (P = .61).
Discussion
Despite the frequency of nasal FBs in children, no uniform management protocol exists. Primary care providers and emergency physicians commonly attempt removal using direct visualization and a variety of techniques, including forceps, hooks, suction, and positive pressure methods. Repeated failed attempts using these techniques can traumatize the nasal mucosa, cause bleeding, and complicate subsequent removal. Sedation-based series report high success with low complication rates, but these require greater resources, time, and expense than office removal. Our consecutive series demonstrates that with our standardized protocol involving proper restraint, topical anesthesia and vasoconstriction, head stabilization, and direct microscopic visualization, 96% of nasal FBs could be safely removed in the office without sedation. This protocol avoided the risks of general anesthesia for 96% of patients while yielding a success rate similar to the best series in the literature (Brown et al 6 95% success; Lou 8 92%; Jung et al 9 96%; Abou-Elfadl et al 10 92%; Jungbauer et al 11 81%-95%; Cetinkaya et al 12 87%).
We believe that adequate topical anesthesia and vasoconstriction are important to successful nasal FB removal. Without it, children cannot be faulted for resisting instrumentation as the nasal lining is richly innervated. In 1 reported series that did not take advantage of local anesthetics, only 57% of FBs were successfully removed by emergency physicians. 13
The operating microscope, used in all of our cases, provides true depth perception which is lacking when a monocular rhinoscope or a headlight is used. The microscope frees both hands during foreign body extraction enhancing control of the child’s head (Figure 2A). The improved illumination and magnification offered by an operating microscope allow accurate localization of foreign bodies and facilitate control of rigid instruments while avoiding contact with the nasal septum or turbinates. The right-angle, blunt Gross hook is a powerful tool for removal of spherical and other nongraspable FBs but can easily injure the septum if not directly visualized at all times (Figure 2B).
The use of physical restraint remains a topic of intense debate. In our experience, brief restraint for foreign body removal is generally well tolerated, especially when an informed, supportive parent is present throughout the procedure. Our protocol includes a discussion with the child and family about the need for restraint and shared decision-making. If a family opposes restraint in a papoose, hand and head holding with the child on a table (not an exam chair) can be a reasonable alternative. Only 1 child could not tolerate physical restraint in this series, and no parent or caregiver declined restraint after it was explained in detail.
Most practicing otolaryngologists do not have facilities for pediatric procedural sedation in their offices. While procedural sedation, especially in the emergency department, has demonstrated high rates of successful FB removal, the advantages of procedural sedation must be balanced with its drawbacks and risks. Sedation may require a period of separation of the child from parents and often the placement of an intravenous catheter. These can be traumatic even when oral amnestic medications are administered in advance. While procedural sedation is very safe when performed by highly trained personnel in tightly regulated environments, adverse events including vomiting, agitation, and hypoxia complicate up to 10% of inductions.14,15 Outside of the emergency department, procedural anesthesia is typically scheduled, so families face a delay in treatment, lost time from work and school, and added expense for FB removal in a sedation suite or surgical center.
Attempts to standardize and improve surgical care focus on safety and efficacy. Our rate of successful office removal of nasal FBs is comparable or better than series in the literature. In addition, 44% of FB removals were in children with previous failed attempts at extraction. Success rates are generally much lower for repeat attempts. 16 Part of the favorable safety profile of our multiyear series can be attributed to the universal use of head stabilization. Sudden movement of a child’s unrestrained head risks both intranasal injury and failed removal due to bleeding and/or agitation. It is not possible to predict which child will lose composure and jerk at a critical moment in FB removal, so a stable head, bimanual use of instruments, and control of the child’s hands should be considered for each procedure.
There are important limitations to our retrospective study. Even a fastidious keyword search of office notes might miss a portion of treated patients or skew the results compared to a prospectively designed study. Minor complications such as transient epistaxis may not have been consistently included in office or operative notes. Our single-surgeon pediatric-specialist results may not be generalizable to other physicians with different training or less frequent exposure to foreign body removal. The common use of physical restraint we employed might not be acceptable in other parts of the country or in other cultures worldwide. Finally, as this study is a retrospective case series, the only controls are similar published series. Thus, we cannot say which elements of the protocol (topical anesthesia, microscopy, restraint, or the experience of the operator) contributed to its success.
Conclusion
We have reviewed the results of a protocol for office removal of nasal FBs that includes consistent uses of an operating microscope, topical anesthesia, and vasoconstriction, restraint of the patient’s hands and head, and instrumentation rather than positive pressure or balloon catheters for FB extraction. This resulted in a high rate of successful FB removal, even in children with prior failed attempts. There were no significant nasal injuries in this 22 year experience that included children with attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder. This approach should be considered by otolaryngologists who care for children in the office setting.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. It was approved by the Temple University Institutional Review Board (protocol 31341) on February 5, 2024.
Consent to Participate
Written informed consent waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data from this study are available for review by interested researchers. The authors would be pleased to assist via the corresponding author’s email.