
Abstract
Tracheal perforation is an extremely rare and potentially dangerous complication of a partial thyroidectomy. The current case represents a unique presentation of delayed tracheal perforation following an uncomplicated thyroid isthmusectomy for tissue diagnosis of an aggressive appearing thyroid mass in the setting of high-dose steroid administration and recent intubation and self-extubation. While conservative management of tracheal perforation can sometimes be appropriate, our patient was successfully managed via primary closure and infrahyoid muscle transposition flap to cover a 5 mm right lateral tracheal wall defect. We recommend caution be exercised following thyroid surgery in the setting of intubation and high-dose steroids.
Introduction
Delayed tracheal perforation after thyroidectomy is an exceedingly rare complication that has only been reported twice after hemithyroidectomy 1,2 and several times after total thyroidectomy. 3 -9 In the present report, we describe a case of tracheal perforation presenting 9 days postoperatively after partial thyroidectomy (isthmusectomy) in a patient being treated with high-dose steroids. We also discuss a number of potential pathophysiologic mechanisms underlying the development of postoperative tracheal perforation.
Case Report
A 50-year-old man with a remote history of a pituitary adenoma resection presented to an outside hospital with dyspnea, stridor, and altered mental status. He was found to have a rapidly enlarging thyroid mass compromising his airway, for which he underwent endotracheal intubation in the operating room. He was then transferred to our institution, a tertiary medical center, for further care of a presumed invasive thyroid cancer. Upon arrival, he was noted to be severely hyponatremic, hypothermic, bradycardic, and hypotensive. He was diagnosed with myxedema coma and adrenal insufficiency, and treated with levothyroxine, triiodothyronine, desmopressin, and stress-dose hydrocortisone. A computed tomography (CT) scan of the neck revealed a heterogeneous thyroid mass measuring 6.5 cm × 4.3 cm × 7.8 cm with possible erosion of the thyroid cartilage and abutment of the left common carotid artery (Figure 1). A fine needle aspiration (FNA) and core needle biopsy revealed rare foci of atrophic thyroid epithelium in a background of chronic inflammation. His differential diagnosis included fibrosing thyroiditis or thyroid malignancy. He self-extubated 5 days after intubation but was successfully stabilized on high-flow oxygen. Given the diagnostic uncertainty and inconclusive histopathology from his FNA, he underwent an uncomplicated isthmusectomy on hospital day 12 for tissue diagnosis. His regimen of 100 mg hydrocortisone every 8 hours was tapered down to 10 mg daily prior to surgery. Pathology revealed densely fibrotic tissue and chronic inflammation, consistent with a fibrous variant of Hashimoto’s thyroiditis. After an uneventful postoperative recovery, the patient was discharged the following day on a regimen of 20 mg of prednisone daily.
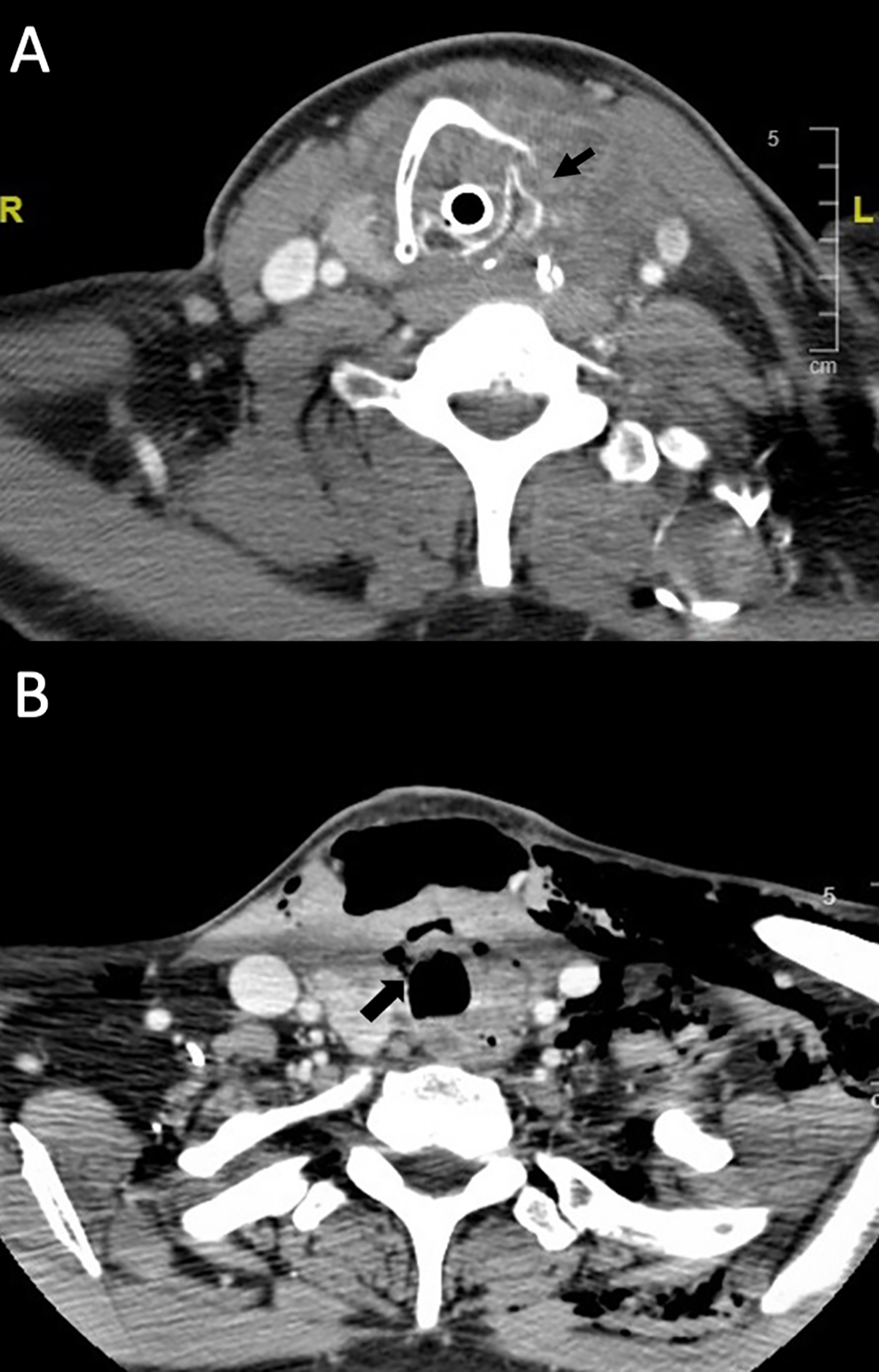
A. Axial CT image on initial presentation demonstrating a large, heterogeneous mass involving the isthmus and thyroid gland bilaterally, concerning for primary thyroid cancer. Malignancy was suspected due to possible erosions of the thyroid cartilage (arrow). B. Axial CT scan on postoperative day 9 following an uncomplicated isthmusectomy for tissue biopsy, demonstrating a right lateral tracheal defect (arrow) with associated extensive subcutaneous emphysema. CT indicates computed tomography.
Nine days after discharge, the patient presented with neck stiffness, swelling, and tenderness along his incision site, reportedly after an episode of coughing. He was afebrile, well-appearing, and breathing comfortably. Physical examination demonstrated extensive crepitus of the bilateral neck and face, with an area of swelling anterior to the trachea that grew with the Valsalva maneuver. Flexible laryngoscopy revealed fibrinous exudate at the right lateral tracheal wall. CT neck imaging implicated a right lateral tracheal defect leading to subcutaneous emphysema (Figure 1). He was taken to the operating room for endoscopic examination and repair of the tracheal defect. On examination of the cervical trachea, several superficial mucosal ulcerations were noted along with a fibrinous exudate within a 5 mm right tracheal defect between tracheal rings 1 and 2, corresponding to CT imaging and findings on prior laryngoscopy (Figure 2). The previous neck incision was opened, and the tracheal defect was closed primarily using 3-0 vicryl sutures. Fibrin tissue sealant and an infrahyoid muscle transposition flap were applied to buttress the defect. A Penrose drain was placed, the neck was closed in layers, and a pressure dressing was applied to the neck. The drain was removed after 3 days and the patient was discharged after an uncomplicated postoperative course. Five months later, the patient returned with an enlarging ipsilateral neck mass causing dyspnea, and was ultimately diagnosed with diffuse large B-cell thyroid lymphoma.
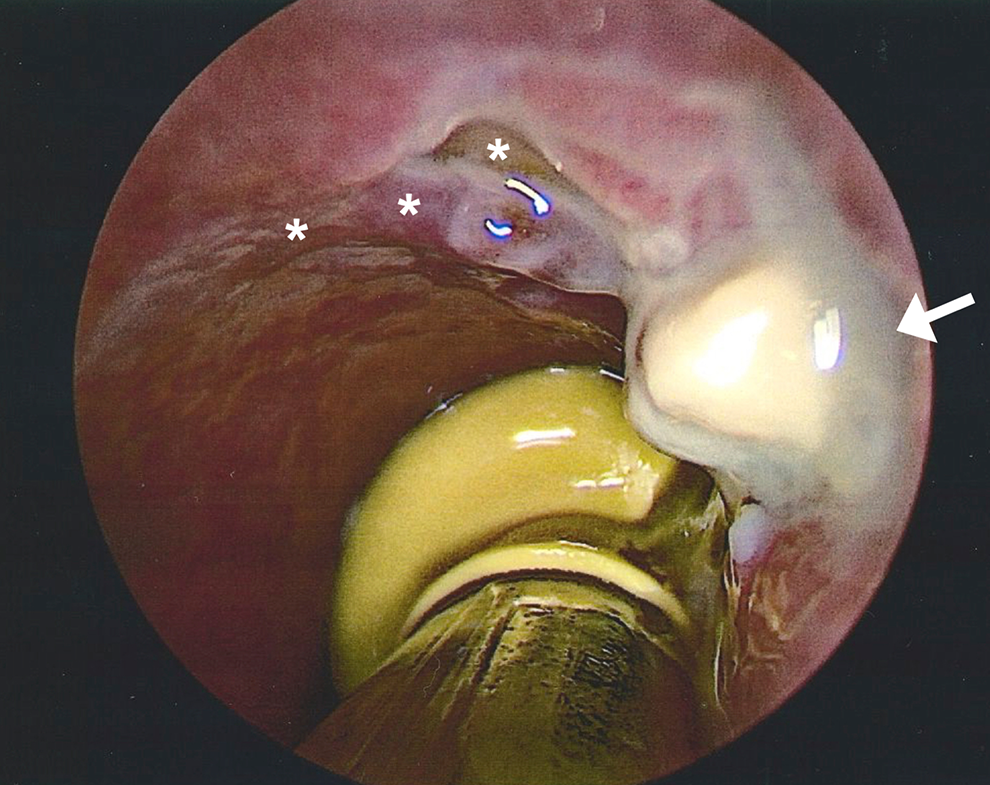
Intraoperative endoscopic view of the cervical trachea revealing fibrinous exudate at the site of a 5 mm right tracheal wall defect between tracheal rings one and two (arrow). Asterisks indicate mucosal ulceration involving the entire anterolateral quadrant of the trachea leading to the area of perforation (arrow), suggesting preexisting injury from prior intubation.
Discussion
This case represents a unique complication of partial thyroidectomy. Delayed tracheal perforation is defined as presentation days to weeks after an inciting trauma. Patients can present with subcutaneous emphysema, as in this case, or with respiratory distress secondary to tracheal deviation, pneumothorax, or cardiorespiratory distress. 1 This complication has been reported several times after total thyroidectomy, 3 -9 and only twice following hemithyroidectomy. 1,2 This is the first reported case of delayed tracheal perforation following thyroid isthmusectomy.
Iatrogenic tracheal injury is most commonly incurred at the posterolateral trachea. 10 Suture ligation of vessels surrounding the ligament of Berry or use of electrocautery adjacent to the trachea results in devascularization, ischemia, and necrosis, ultimately presenting as delayed tracheal injury. 10 Bilateral blood supply to the trachea may be protective of this damage in partial thyroidectomy, while a total thyroidectomy poses a greater risk of violating collateral vasculature. In our case, the anterolateral trachea was affected. While the perforation was within the lateral extent of the resection, the isthmusectomy was performed using ultrasonic shears, as opposed to monopolar electrocautery, to avoid direct heat transfer to the trachea. No tracheal injury was noted at the end of the procedure.
Tracheal perforation after thyroidectomy has been reported to present 4 to 27 days postoperatively. 1,4 Perforation typically occurs secondary to elevated subglottic pressure through a weakened portion of the trachea, generally following exercise, coughing, or sneezing where subglottic pressure is markedly elevated. 1 Many aspects of our patient’s hospital course likely contributed to weakening of the tracheal wall. Our patient was on high-dose steroids, with an underlying inflammatory process and possible associated lymphoma at that time. While corticosteroids are used to inhibit inflammation, they also decrease the immune response to insults and delay wound healing. Additionally, our patient remained intubated for 5 days, which subjects the tracheal wall to endotracheal tube cuff pressure, prior to self-extubating, which can also cause significant tracheal mucosal injury. The intubation and extubation coupled with the adjacent isthmusectomy while on high-dose steroids seemingly weakened the tracheal wall to such an extent that perforation occurred subsequent to his coughing episode. These findings suggest that surgeons should exercise increased caution when performing thyroid surgery in the setting of high-dose steroid use.
Delayed tracheal perforations may be managed conservatively or surgically depending on the severity of presentation. Well-appearing patients with a stable air pocket may avoid surgery by having a Penrose drain and compressive dressing placed at bedside. 1 Any concern for airway compromise or evidence of large perforation should prompt operative management. Surgical repair may involve closing the defect with absorbable suture and/or utilizing rotational muscle flaps for larger defects. 7,8
Conclusion
While uncommon, delayed tracheal perforation after thyroid surgery is a serious complication that surgeons should be aware of, especially in the setting of high dose steroid administration. Conservative versus operative management can be successful depending on the defect size and patient’s stability.
Footnotes
Authors’ Note
This study was deemed exempt by the Institutional Review Board at the University of California, Los Angeles, due to the deidentified nature of the report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant No. RO1 DC011300 from the National Institutes of Health.