
Abstract
Necrotizing tracheitis is a rare condition, mainly seen in immunocompromised patients, that may lead to pseudomembrane formation, airway obstruction and in severe cases, tracheal perforation. We present a case of a 32-year-old male with poorly controlled diabetes who presented with productive cough, dysphagia, and respiratory distress. Bronchoscopy revealed extensive tracheal necrosis along a 4-5 cm segment of cartilaginous trachea and was complicated by tracheal perforation with false passage into the anterior mediastinum. Once the airway was re-established, a multidisciplinary team discussed options for definitive airway management, including tracheal reconstruction, pulmonary stent, or tracheostomy. Ultimately, a distal XLT tracheostomy was placed. Microbiology specimens of the tracheal tissue were positive for Actinomyces. The patient was started on long-term antibiotics and diabetes management. At three-month follow-up, the trachea was patent with near complete mucosalization of the previously necrotic segment. An area of proximal tracheal stenosis was successfully managed with a customized tracheal T-tube. In conclusion, this is a case of necrotizing tracheitis complicated by tracheal perforation. Successful treatment required a multidisciplinary team for airway management as well as medical treatment of immunocompromising risk factors and antimicrobial therapy. This enabled timely healing of the trachea and a durable airway.
Introduction
Necrotizing tracheitis is a rare, but life-threatening condition of the central airway that may lead to pseudomembrane formation, airway obstruction, and in severe cases, tracheal perforation. 1 This condition is primarily seen in immunocompromised patients and the most commonly reported etiologies include fungal organisms, mainly Aspergillus species as well as various bacteria.2-4 Due to persistent airway inflammation and tissue friability along with immunocompromising risk factors, necrotizing tracheitis presents a particular challenge in airway management. Here, we present a case of necrotizing tracheitis secondary to Actinomyces species, which was complicated by tracheal wall perforation, requiring a multidisciplinary effort for airway management.
Case Report
A 32-year-old male with poorly controlled diabetes mellitus type I and a history of polysubstance abuse presented with productive cough, hoarseness, dysphagia, and respiratory distress. The patient had recently been admitted for diabetic ketoacidosis with unstable blood glucose ranging from 29 to 324 mg/dL. On admission, CT imaging revealed severe tracheal stenosis and pseudomembrane formation (Figure 1) and bronchoscopy demonstrated malodorous tissue with loss of tracheal wall integrity concerning for necrotizing tracheitis. Due to concerns for an unstable airway, the patient required urgent debridement, intubation, and transfer to a higher level of care. Computed tomography imaging on initial presentation showing necrotizing tracheitis with pseudomembrane formation.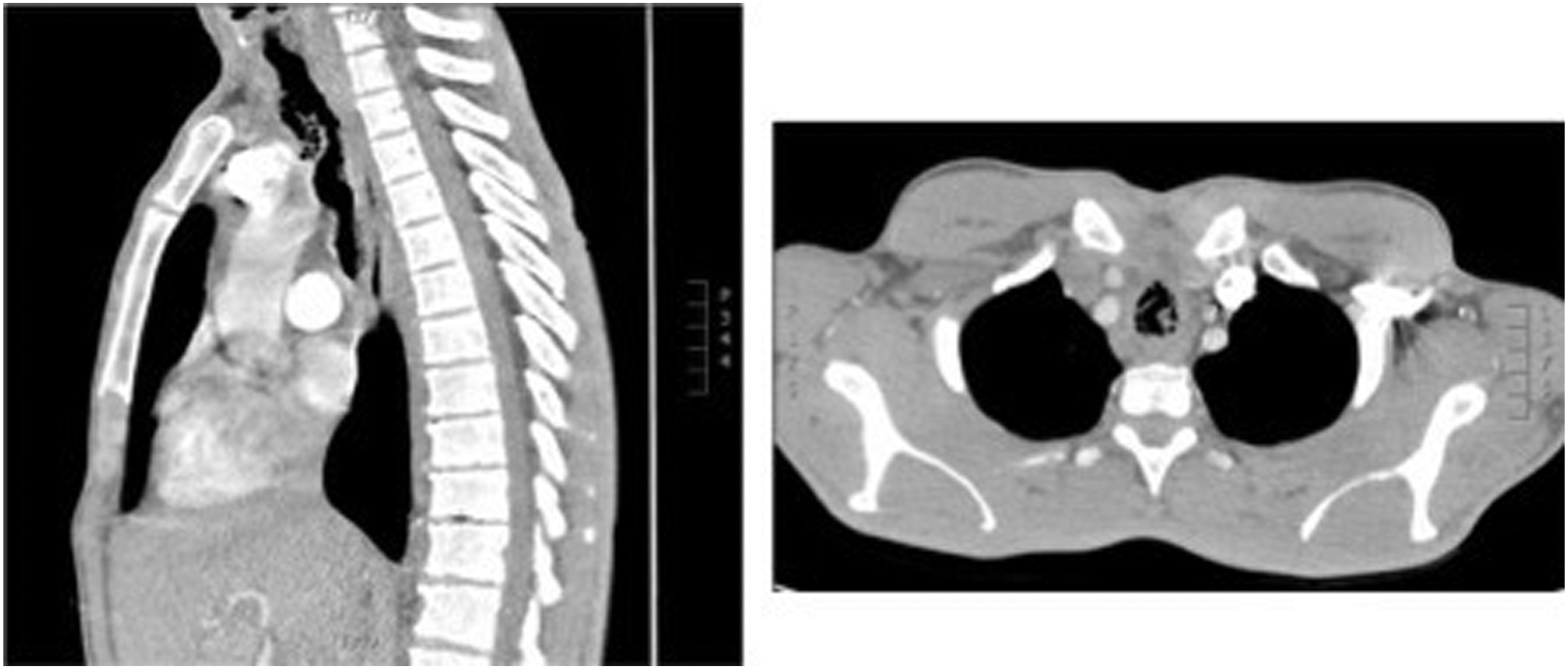
Upon transfer to our institution, initial bronchoscopy discovered a significant tracheal perforation of the anterior and lateral tracheal wall. Subsequent re-intubation resulted in false passage into the mediastinum, prompting emergent airway response. The patient required fiberoptic guided intubation to avoid false passage. Once the airway was stabilized, bronchoscopy was performed 3 days later demonstrating extensive tracheal necrosis along a 4–5 cm segment approximately 4 cm above the carina with complete involvement of cartilaginous trachea (Figure 2). Biopsies showed necrotic cartilage with mixed bacteria and fungi; Actinomyces and Candida were initially identified. A multidisciplinary team discussed options for airway management, including tracheal reconstruction, pulmonary stent, or tracheostomy. Ultimately, a definitive airway was established 1 week after presentation with placement of a distal XLT tracheostomy which was confirmed to extend beyond the necrotic segment. Microbiology specimens were positive for Actinomyces, Candida, and superinfection with methicillin sensitive Staphylococcus aureus (MSSA). Medical treatment with strict glucose control and long-term antibiotics were provided with significant improvement of symptoms. The patient was discharged 17 days after tracheostomy after successful exchange to a cuffless tube. Post-intubation bronchoscopy demonstrating 4–5 cm segment of necrotic trachea.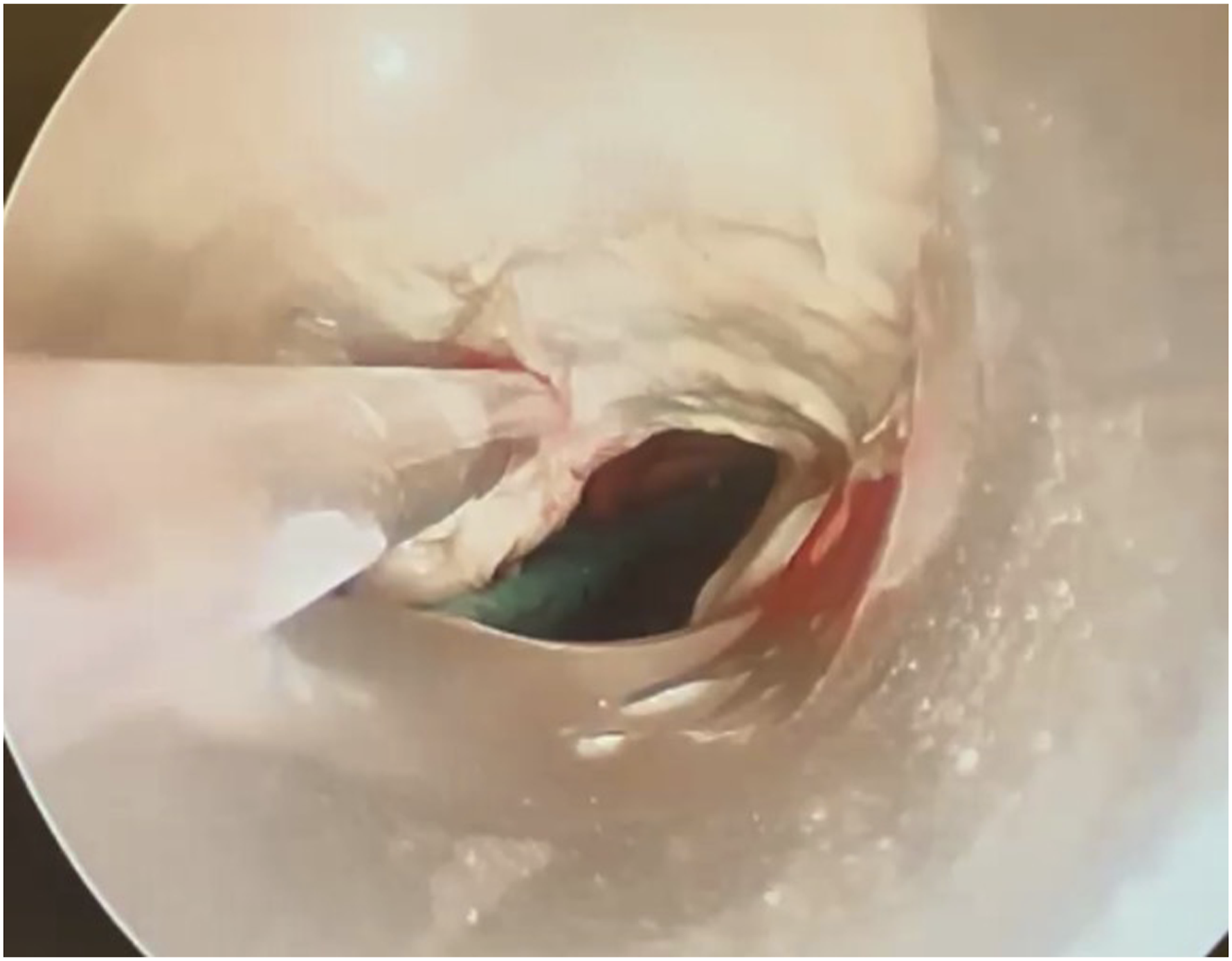
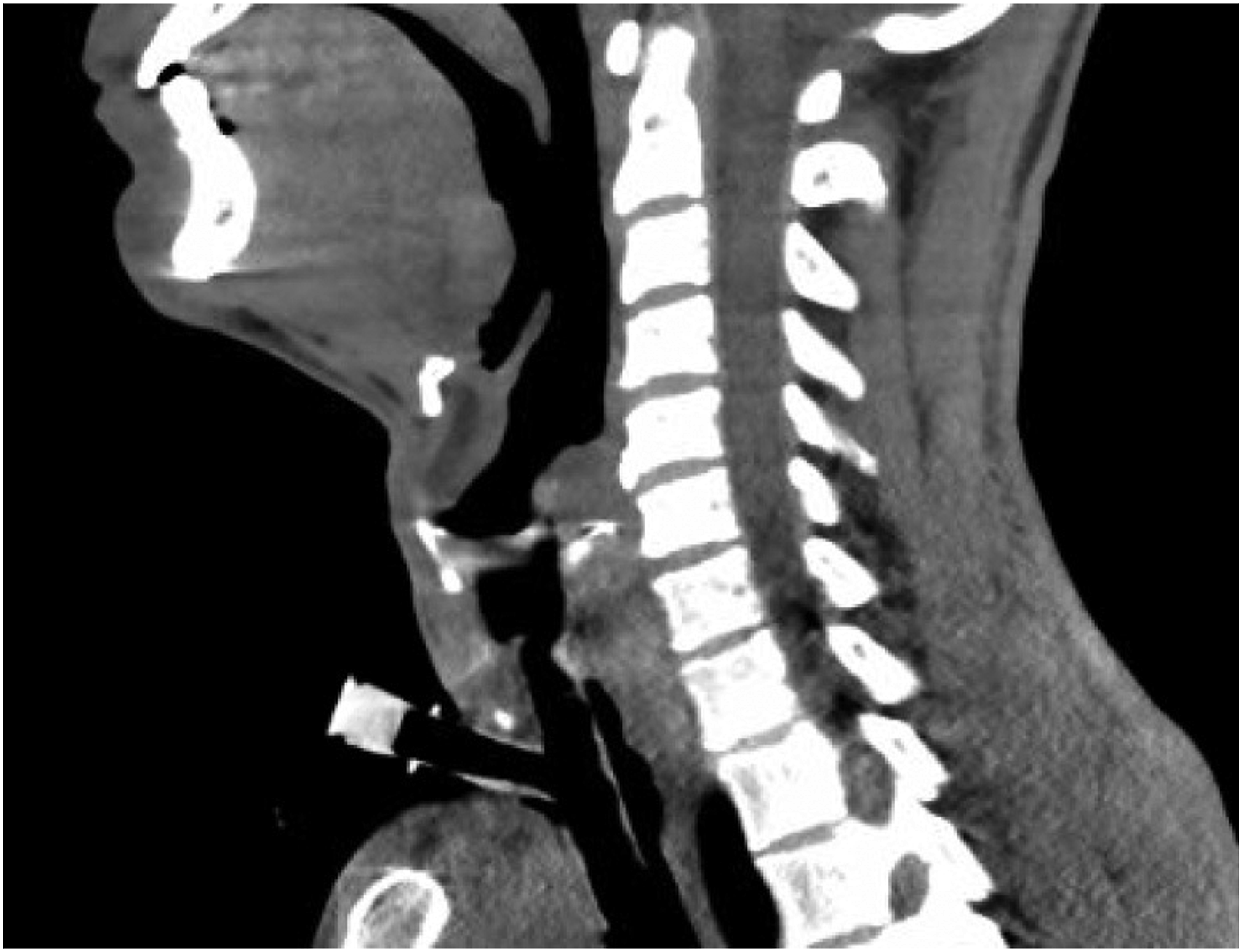
Three months after discharge, bronchoscopy showed a patent trachea with near complete mucosalization of the previously necrotic segment (Figure 3). However, the patient was noted to have an area of persistent proximal tracheal stenosis. To address this, a personalized T-tube (Hood Laboratories) was designed using CT imaging, measuring 2.0 cm proximally and 1.5 cm distally, and placed bronchoscopically to maintain patency of the stenotic segment (Figure 4). This personalized T-tube is presently in place, with the most recent bronchoscopy demonstrating improved airway epithelialization without recurrent tracheal stenosis. Currently, discussion regarding future management is centered on possible tracheal resection and reconstruction to facilitate decannulation. Bronchoscopy at three-month follow-up showing improved airway epithelialization. Airway management with custom T-tube bypassing proximal stenosis, with proximal extent 15 mm below glotti.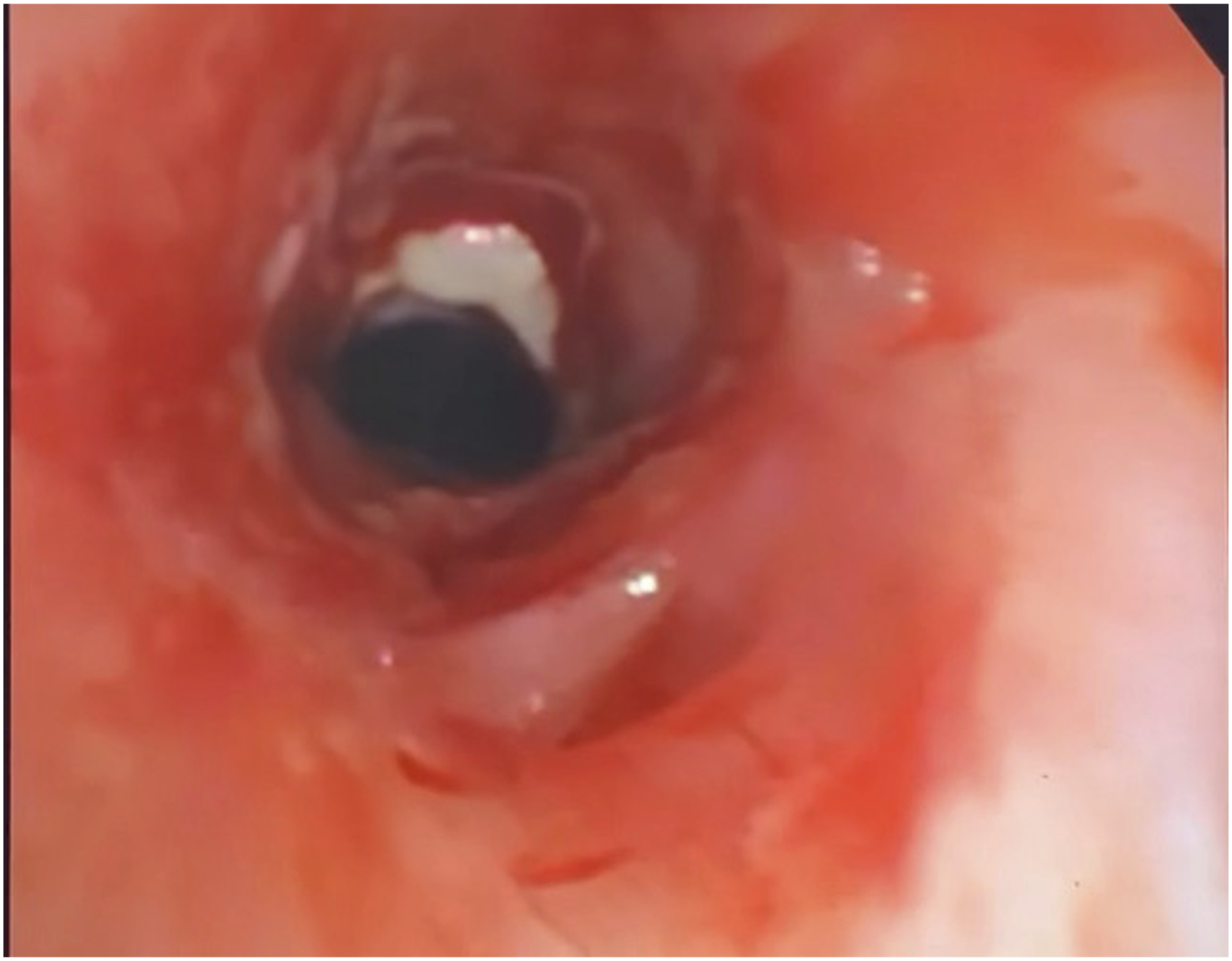
Discussion
Necrotizing tracheitis is a rare condition of the central airway that encompasses several entities that have been reported in literature, which include invasive fungal tracheitis, invasive tracheobronchitis, pseudomembranous tracheitis, and other related variations.3,5-7 These conditions present with similar symptoms of hoarseness, cough, dyspnea, and respiratory distress and they are all characterized by severe tracheal inflammation and distinct pseudomembrane formation. Necrotizing tracheitis is primarily seen in immunocompromised patients susceptible to invasive infection. The most common infectious causes of necrotizing tracheitis are fungi, primarily Aspergillus, and bacteria including Corynebacterium species, Staphylococcus aureus, Bacillus cereus, Mycoplasma pneumonia, and Pseudomonas aeruginosa.2-4,8-11 Less commonly, viruses such as Cytomegalovirus have also been reported. 12 Interestingly in the pediatric population, necrotizing tracheitis appears to be commonly caused by a superimposed infection of Influenza A and Staphylococcus aureus. 13 Non-infectious causes of necrotizing tracheitis that have been reported include endotracheal intubation and inflammatory bowel disease.14-16
Necrotizing tracheitis causes persistent airway inflammation and tissue friability, increasing the risk for emergent complications such as airway obstruction and tracheal perforation, both of which were seen in this case. Successful management of this patient’s airway required a multidisciplinary discussion. Pulmonary stent and tracheal resection/reconstruction were not ideal initial treatment options given the fragility of the tracheal wall and risk for erosion of the tracheal wall. Ultimately a safe and durable airway was achieved with a tracheostomy that was able to bypass the distal extent of the necrotic region until acute infection and underlying medical conditions were stabilized. Depending on the location and extent of necrosis, custom tracheostomies may be required to bypass unstable airway segments. More proximal injuries can be bypassed to stabilize the patient but there is a risk for proximal stenosis. As seen in this case, proximal tracheal stenosis resulted after tracheostomy, likely due to loss of tracheal cartilage integrity causing luminal narrowing, and this was successfully managed with a personalized T-tube. Similar to previous reports, tracheostomy is an appropriate intervention in patients with respiratory failure secondary to necrotizing tracheitis, though custom tubes may be required depending on extent of disease. 2 Tracheostomy may serve as a bridge to future airway reconstruction or a definitive stable airway in patients who are not surgical candidates.
A major factor supporting recovery in this case was appropriate medical management of necrotizing tracheitis. In this case, the primary infectious etiologies were Actinomyces, Candida, and MSSA, which were appropriately treated with several months of antibiotic treatment. However, given that the majority of patients with necrotizing tracheitis are immunocompromised, management should also focus on treatment of underlying immunosuppression. Most reports of necrotizing tracheitis identify patients who are undergoing chemotherapy, organ transplant patients, or patients with other immunocompromising comorbidities. 1 In our case, the patient’s primary risk factor was likely his poorly controlled diabetes. Therefore, medical management was focused on strict blood glucose control both during hospitalization and upon discharge. Ultimately, this enabled appropriate healing of the trachea and prevention of further complications of his condition.
Conclusion
This is a case of necrotizing tracheitis in a patient with poorly controlled diabetes, complicated by tracheal perforation. Successful treatment required a multidisciplinary team for airway management as well as medical treatment of immunocompromising risk factors and antimicrobial therapy. Ultimately, tracheostomy and supportive medical management enabled timely healing of the trachea and a durable airway with customized T-tube.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.