
Abstract
Thyroidectomy is a safe procedure that is frequently performed for benign or malignant thyroid disease. Complications after thyroidectomy occur in approximately 3%–5% of patients. Tracheal perforation is a very rare post-thyroidectomy complication, and delayed tracheal perforation without intraoperative tracheal injury is even rarer; only 25 case reports have been published globally, with varied management. We present the case of a 36-year-old man presenting with dyspnea and cough 2 weeks after left thyroidectomy. A defect measuring approximately 2 cm was confirmed on the anterior wall of the trachea by computed tomography and flexible laryngoscopy. The patient’s symptoms improved with conservative treatment including systemic steroids, and surgical treatment was not required. Even in the absence of unusual intraoperative events, delayed tracheal necrosis and perforation should be considered as possible postoperative complications following thyroidectomy.
Introduction
Thyroidectomy is a safe procedure that is commonly performed for both benign and malignant thyroid diseases. 1 Complications occur in only about 3%–5% of patients after thyroidectomy, with tracheal perforation occurring in approximately 0.06% of cases. 2 Tracheal perforation related to thyroidectomy is usually detected during surgery, and recovery without major complications is possible with appropriate management. However, delayed tracheal perforation without an intraoperative tracheal injury is an extremely rare but life-threatening condition, with only about 25 cases reported worldwide. We present a case of delayed tracheal perforation in a 36-year-old male patient 2 weeks after a left thyroidectomy, accompanied by a literature review.
Case Presentation
A 36-year-old male patient underwent left thyroidectomy for a 4.0 × 3.5 cm follicular neoplasm at the Department of Surgery, Chungnam National University Hospital. The patient was discharged without any unusual issues 3 days after the surgery, and a pathological examination revealed minimally invasive follicular thyroid carcinoma. Microscopically, invasion of the lymphatic vessels was noted. Two weeks after the surgery, the patient complained of worsening dyspnea when lying down, sore throat, and coughing, and a wheezing sound was noted during inhalation. The patient visited the pulmonology department of the hospital, but no relevant findings were observed on chest radiography and pulmonary function tests.
The patient visited the otorhinolaryngology department of the hospital and underwent a computed tomography scan of the neck. A tracheal defect measuring approximately 6 × 20 mm was observed in the second and third trachea ring positions, which were expected to correspond to the site of thyroid lobectomy (Figure 1A). Flexible laryngoscopy revealed a defect in the anterior wall of the trachea, approximately 3 cm below the subglottis (Figure 1B). The patient had severe obesity (body mass index, 40.12 kg/m2), hypertension, and severe uncontrolled diabetes (hemoglobin A1c, 10.5%), but no other underlying diseases. Further tests, including blood tests and electrocardiography, showed no abnormalities. Based on the patient's clinical course, symptoms, and the results of laboratory and imaging tests, a diagnosis of dyspnea due to delayed tracheal perforation after thyroid surgery was made. Initial neck CT and flexible laryngoscopy image. (A) Axial CT scan. 20 × 6 mm sized linear tracheal wall defect (white arrow) in the anterior tracheal wall. (B) Laryngoscopy image. A tracheal wall defect (black arrow) on the left anterior tracheal wall.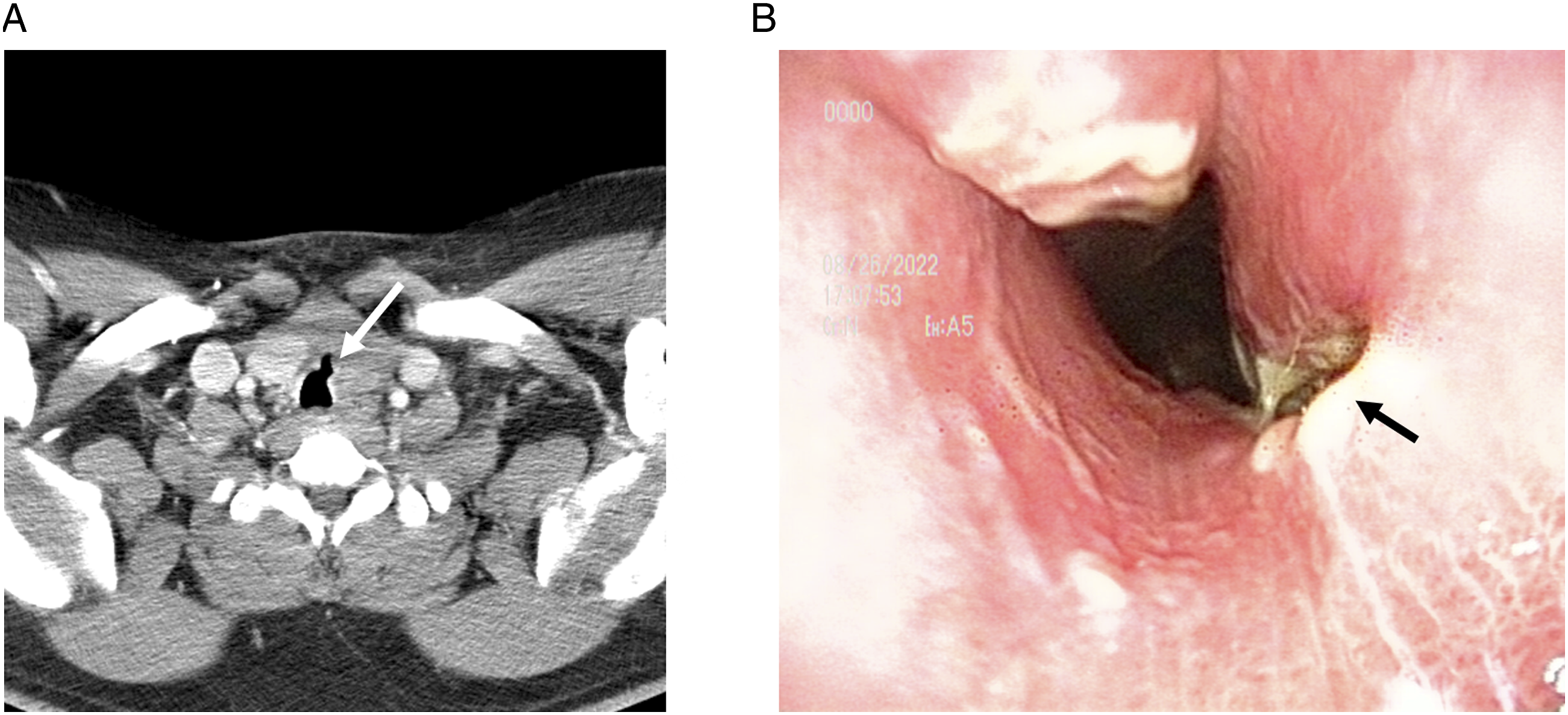
A conservative therapy plan was made, and the patient was admitted to the hospital. The patient was informed about the possibility of an emergency tracheostomy or surgery if symptoms worsened or oxygen saturation decreased. During the hospital stay, the patient received conservative therapy including fasting and bed rest, nebulizer low-oxygen therapy, prophylactic antibiotics, and low-dose steroid therapy, accompanied by close monitoring of his blood glucose levels. From the sixth day of hospitalization, no choking sounds were heard during breathing, and the patient’s breathing discomfort improved. The patient was discharged without worsening symptoms on the ninth day of hospitalization.
After 3 weeks, the patient visited the outpatient clinic and underwent flexible laryngoscopy, which showed no anterior wall defect in the trachea, although some mucosal swelling caused tracheal stenosis. A computed tomography scan taken 1 month after the discharge showed a significant decrease in the size of the previously observed tracheal defect. The patient has been symptom-free and under outpatient follow-up for 3 months.
Discussion
Thyroidectomy is commonly performed worldwide and has a low rate of complications (less than 3%–5%). 2 Delayed tracheal perforation without an intraoperative tracheal injury is a rare complication, with only about 25 cases reported worldwide. The risk factors for delayed tracheal perforation related to thyroidectomy include female sex and toxic thyroid nodules, particularly if the nodules are large and compress the trachea for a long time, causing the tracheal wall to weaken. Prolonged high steroid doses before surgery,3 –5 previous radiation therapy, 2 and other factors such as high pressure during the procedure, damage to the trachea from the suction tube, and blood flow interruption during the coagulation process with an electrocautery device can also increase the risk of tracheal perforation. 3
After surgery, repeated coughing or infections due to blood clots can become risk factors. 1 In this particular case, the risk factors may have been the large (4.0 × 3.5 cm) thyroid nodule and the use of an electrosurgical device. The patient’s uncontrolled diabetes may also have caused delayed wound healing and inflammation, resulting in the occurrence of delayed tracheal perforation.
Previously Reported Cases of Delayed Tracheal Perforations After Thyroidectomy.
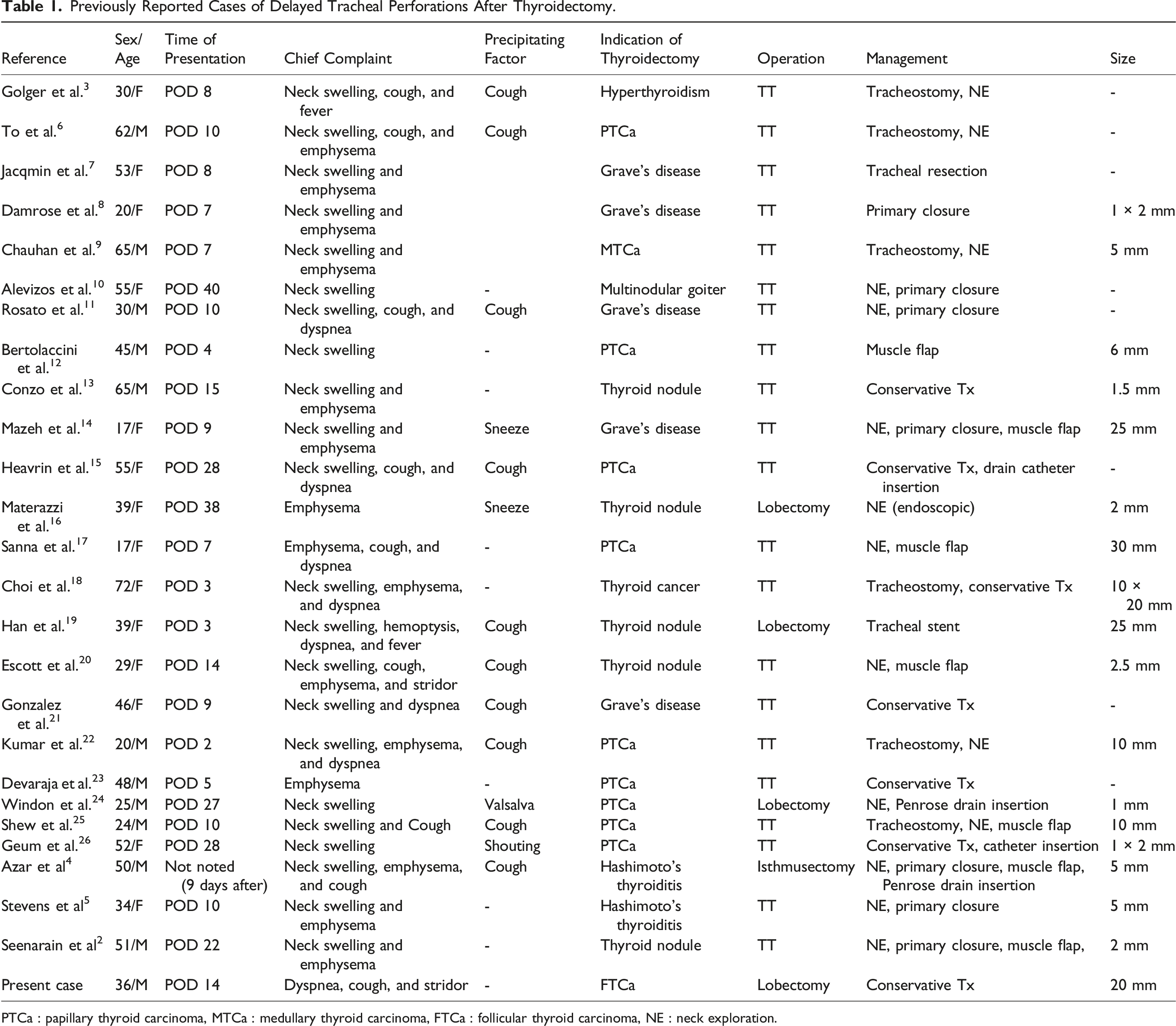
PTCa : papillary thyroid carcinoma, MTCa : medullary thyroid carcinoma, FTCa : follicular thyroid carcinoma, NE : neck exploration.
The treatment of tracheal defects depends on the severity of the patient’s symptoms and the size of the tracheal defect. 26 In patients with small defects and no or improving respiratory distress, conservative treatments such as antibiotics, high-pressure oxygen supply, bed rest, and low-dose steroid therapy may be used. 21 However, cases of unstable or severe respiratory distress necessitate prompt surgical treatment. 21 It is important to be prepared to perform emergency intubation or tracheotomy. When intubating, the tracheal tube should be positioned below the defect, and high cuff pressure should be avoided to prevent further worsening of the patient's condition. 8 If the defect is small and the inflammation is minimal, primary suturing is sufficient. 26 However, if the inflammation is severe and primary suturing is not possible, a temporary tracheotomy can be performed to induce spontaneous healing. 18 In cases of localized severe inflammation and non-circumferential defects, muscle flaps can be used to reinforce the defect; however, in cases of circumferential defects exceeding half of the trachea, tracheal resection and reconstruction or anastomosis may be necessary. 7 Other treatments include inserting a tracheal stent 19 or using conservative treatment by inserting a catheter or drain to remove air continuously flowing into the defect area, without cutting the skin, in cases with mild symptoms.15,24,26
This case report differs from most previously reported cases in the literature because the patient presented with respiratory distress as the main symptom after thyroid lobectomy, instead of neck swelling and subcutaneous emphysema. A significant defect with a linear dimension of about 2 cm was found in the anterior tracheal wall by computed tomography and flexible laryngoscopy, but there was no evidence of inflammation from serum tests, stable vital signs, and normal findings of artery blood gas analysis. The patient was treated with conservative therapy, including low-dose systemic steroids, without surgical intervention, and has shown improvement without worsening of symptoms.
In conclusion, thyroidectomy is considered a safe and low-risk surgical procedure, but there is a possibility of delayed tracheal perforation and necrosis as a surgical complication. To reduce the risk of this complication, it is crucial to identify high-risk patients before surgery, minimize the use of electrocautery near the trachea during surgery, and closely inspect the trachea for injury before completing the procedure. It is also important to instruct patients to avoid activities that may place significant pressure on the trachea, such as excessive coughing or sneezing, for at least a month after surgery. Furthermore, during follow-up visits, a comprehensive medical history and physical examination, taking into account potential complications, is necessary.
Footnotes
Author Contributions
Da Beom Heo: Writing: original draft, collecting data, formal analysis, and data curation. Hyo One Son: visualization, collecting data, and data curation. Han Wool John Sung: data curation, visualization, and collecting data. Bon Seok Koo: formal analysis, methodology, resources, and writing—reviewing and Editing. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the research fund of Chungnam National University.
Ethical Approval
This case report was approved by the Ethics Committee of the Chungnam National University Hospital.
Informed Consent
The patient was informed about the purposes of the report and has signed a consent form.