
Abstract
Microwave ablation (MWA) is a relatively new, well-tolerated, minimally invasive approach, developed in recent years as an alternative to surgery for low-risk papillary thyroid microcarcinoma (PTMC). We describe an 81-year-old patient with unifocal PTMC who refused active surveillance and underwent percutaneous MWA. Two weeks after the procedure, the patient presented dyspnea and cough, and delayed tracheal perforation was confirmed by computed tomography. Conservative therapy was chosen as the initial treatment, and the tracheal defect was confirmed healing successfully 1 month later. Radiologists should be aware of the possibility of delayed tracheal perforation following MWA even in the absence of unusual intraoperative events.
Keywords
Introduction
Papillary thyroid microcarcinoma (PTMC) is defined as papillary thyroid carcinoma with a size of ≤10 mm, which accounts for an increasing proportion of thyroid cancer cases in recent decades.1,2 Thyroid lobectomy is recommended as the first-line management for low-risk PTMCs in accordance with the 2015 American Thyroid Association guidelines. 3 Owing to the indolent course of PTMC, active surveillance (AS) has been proposed as a treatment option for these patients. 4 However, many patients experience greater anxiety and psychological burden during AS for PTMC, which may greatly impact their quality of life. 5 Recently, microwave ablation (MWA) has been applied to treat low-risk PTMCs and has been reported to have favorable clinical outcomes with low morbidity rates.6-8 Although complications associated with MWA are generally minor and transient, it is not without life-threatening risks. Here, we report a case of delayed tracheal perforation in a female patient 2 weeks after a MWA for PTMC.
Case Report
The patient, an 81-year-old woman, presented with a unifocal PTMC (diameter 5 × 3 × 3 mm) in the left lobe. She refused thyroid lobectomy and AS and underwent ultrasound-guided MWA at an outside hospital. No intraoperative complications were reported. The patient was discharged on the third postoperative day without any exceptional conditions. Two weeks after the treatment, the patient was brought to the emergency department of our hospital with complaints of coughing, stridor, and worsening dyspnea when lying down. Physical examination did not detect swelling or subcutaneous emphysema in her neck or face. A computed tomography (CT) scan showed a defect in the left lateral trachea below the level of the cricoid cartilage (Figure 1A). The patient was admitted to our department, and conservative therapy was initiated. Conservative treatments include bed rest, nebulizer low-oxygen therapy, nutritional support, prophylactic administration of antibiotics, and low-dose corticosteroid therapy. Flexible bronchoscopy was performed on the second day following admission and revealed a clear mucosal necrosis measuring an area of 0.6 cm2 in diameter on the left lateral wall of the second-third tracheal ring (Figure 1B). The patient was informed of the possibility of an emergency tracheostomy or surgery if symptoms worsened or oxygen saturation decreased. After 7 days of conservative treatment, the patient’s symptoms were relieved, and her breathing discomfort was improved. The patient was discharged without worsening symptoms on the 10th day of hospitalization. One month later, a second CT scan revealed a significant decrease in the size of the tracheal defect (Figure 2A). A repeated flexible bronchoscopy was also performed, which showed no significant defect in the tracheal wall, despite a mild mucosal swelling (Figure 2B). Follow-up at 2 months showed a definitive recovery of the patient.
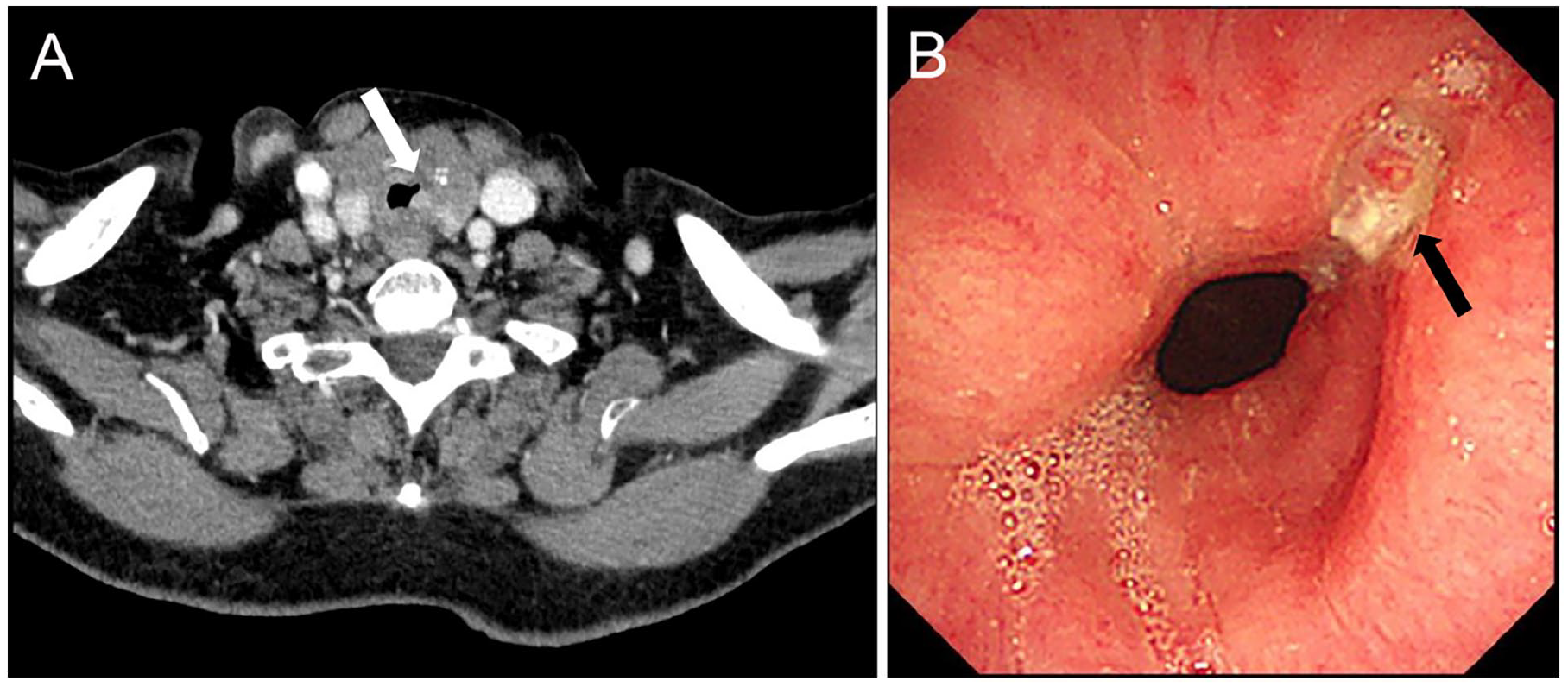
Initial neck CT and flexible laryngoscopy image. (A) Axial CT scan. A left lateral tracheal defect (white arrow). (B) Laryngoscopy image. A left lateral tracheal necrosis (black arrow) measuring an area of 0.6 cm2 in diameter on the second-third tracheal ring. CT, computed tomography.
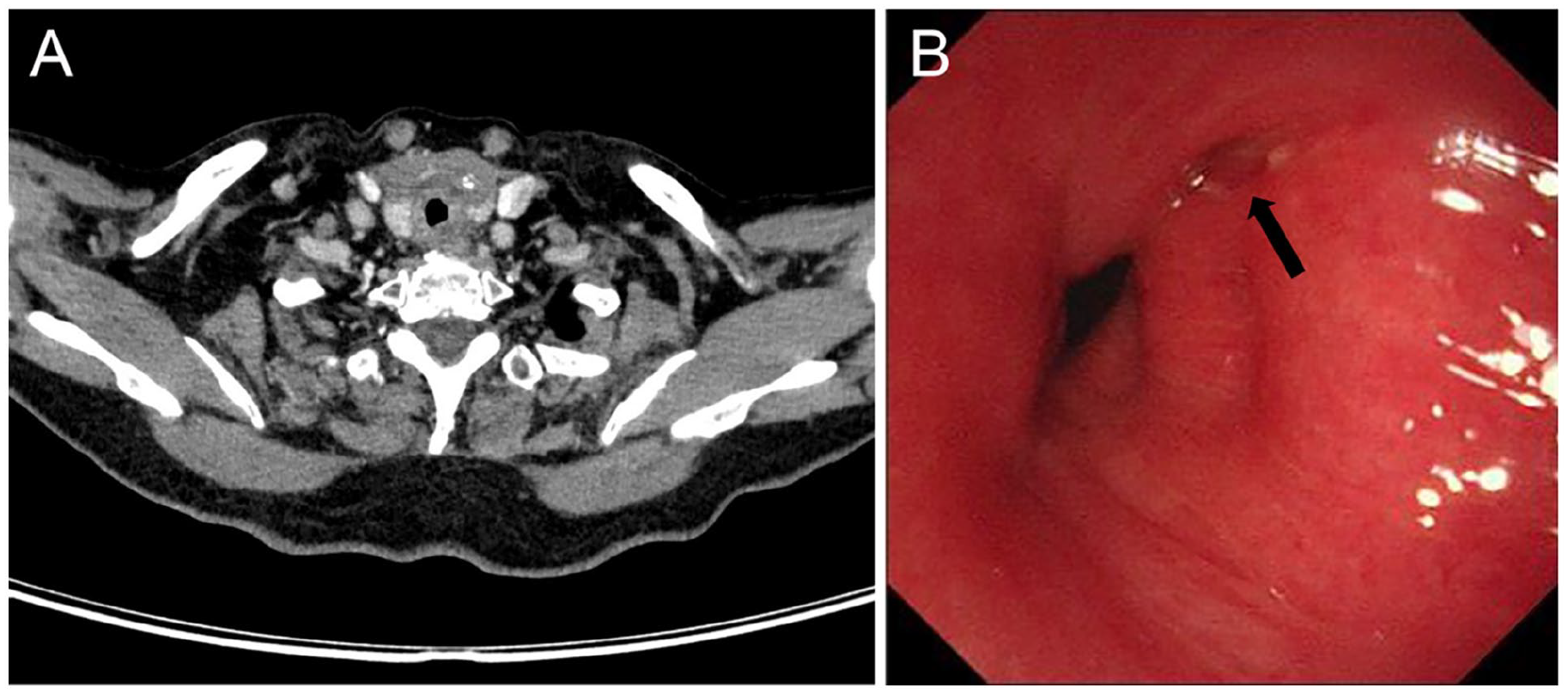
Neck CT and flexible laryngoscopy image 1 month later. (A) Axial CT scan. No significant defect was found on the tracheal wall. (B) Laryngoscopy image. The tracheal stenosis was confirmed to have healed with a mild mucosal swelling (black arrow). CT, computed tomography.
Discussion
Percutaneous thermal ablation techniques, such as MWA, radiofrequency ablation, and laser ablation, have been used mainly for the treatment of benign thyroid nodules as alternatives to surgery. 9 Recently, thermal ablation has also been employed in the treatment of low-risk PTMCs who are not eligible for surgery.10-12 However, thermal ablation techniques carry the risk of unintended injury to surrounding structures. The most commonly reported complications after thermal ablation include hematoma, infection, changes in voice due to recurrent laryngeal nerve (RLN) damage, and thermal injury to surrounding tissue (e.g., trachea, esophagus, or skin).13,14 Delayed tracheal perforation after thermal ablation is rare and has only been described in sporadic reports.15-17 Although rare, it remains a significant concern. This case highlights the potential risk of exceptional tracheal injury associated with MWA for thyroid cancer.
The potential cause of tracheal perforation following MWA is primarily the result of the unintentional spread of heat from the microwave energy to the tracheal wall, resulting in mucosal necrosis, submucosal edema, and even full-thickness damage to the tracheal wall. While the microwave probe is aimed at ablating the tumor tissue, the surrounding soft tissues, particularly those close to the thyroid gland, such as the trachea and esophagus, are at risk of thermal damage.18,19 The extent of thermal damage is influenced by several factors, including the tumor location, size of the lesion, power setting used during the procedure, and duration of ablation. 20 In particular, tumors located in the lower thyroid lobe or those located close to the trachea are more likely to result in thermal injury to the tracheal wall. Thermal injury can cause clinical manifestations such as coughing, stridor, subcutaneous emphysema, hemoptysis, and respiratory distress. Studies have shown that these symptoms are often delayed and appear several days to weeks after the procedure, which emphasizes the importance of careful postoperative monitoring.15-17 In this case, the procedure was uneventful and there were no early complications; however, the symptoms of tracheal injury became clinically evident 2 weeks after ablation. In a similar case reported by Di Renzo et al, the interval between ablation and identification of tracheal necrosis was 50 days. 17
The management of tracheal perforation depends primarily on the severity of the patient’s symptoms and the degree of tracheal damage. 21 Patients with small tracheal defects and mild respiratory symptoms can be conservatively treated with antibiotics, oxygen therapy, bed rest, and low-dose corticosteroid therapy. 22 As seen in this case, the patient’s symptoms improved significantly after 7 days of conservative treatment, and follow-up imaging revealed a marked decrease in the tracheal defect. However, cases of unstable or severe respiratory distress require immediate emergency interventions, such as a tracheostomy or surgical repair, to prevent life-threatening airway obstruction. If the inflammation is severe and primary suturing is not possible, a temporary tracheotomy can be performed to induce spontaneous healing. 23 Surgical repair may involve closing the defect with absorbable sutures and/or utilizing rotational muscle flaps (e.g., sternothyroid muscle) for larger defects.21,24-26 However, the key factors in the successful management of tracheal perforation are early detection and prompt intervention. Endoscopic evaluation, such as flexible bronchoscopy, plays a vital role in assessing the extent of the injury and guiding treatment decisions. Preventive strategies to minimize the risk of tracheal injury include a careful preoperative evaluation, proper tumor location, and meticulous thermal control during the procedure. Avoiding excessive power settings and maintaining an appropriate distance between the ablation zone and critical structures, such as the trachea, esophagus, and RLN, are crucial steps to reduce the risk of thermal damage.15,16 Additionally, the hydrodissection technique, which involves injecting a cooled solution of 5% dextrose between the tumor and surrounding structures, can be applied to reduce the risk of thermal spread and injury to the trachea and RLN. 27
Conclusion
This case highlights the potential risk of delayed tracheal perforation associated with MWA in thyroid cancer treatment. Radiologists and endocrinologists should be aware of this rare but severe complication, which requires timely detection and appropriate management to ensure favorable outcomes. Conservative management may be appropriate for patients with small tracheal defects and no or worsening respiratory distress.
Footnotes
Ethical Considerations
This case report was reviewed and approved by the Ethics Committee of West China Hospital, Sichuan University, China.
Informed Consent
The patient was informed about the publication of the report and has signed a consent form.
Author Contributions
Xiao Yang, original draft writing, collecting data, analysis and interpretation of data; Jingyi Wang, data curation, conceptualization, writing—review and editing; Qing Tang, visualization, writing—review and editing; Rixiang Gong, data curation, writing—review and editing; Tao Wei, data curation, writing—review and editing; Zhihui Li, conceptualization, supervision, project administration, final approval of the version to be published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data underlying this study are available from the corresponding author upon reasonable request.