
Abstract
Otitis media with effusion is a common cause of diminished hearing in children younger than 12 years. Hypertrophy of adenoids is one of the commonest etiologies of this condition. It has been mentioned that with increased size of the adenoid tissue, the more likely the incidence of fluid in the middle ear. The aim of this study was to find whether there is a correlation between adenoid size, tympanometric findings, and type of fluid in the middle ear irrespective of disease duration. This is a prospective study done on 100 pediatric patients (12 years and less) presented with chronic otitis media with effusion (COME) and adenoid hypertrophy from July 2015 till July 2017. Cases with tympanometry evidence of COME (B, Cs) and adenoid hypertrophy seen by nasal endoscopy were included. Adenoid size was graded and correlated with the type of tympanometry and type of fluid in the middle ear. Sixty male children and 40 female children were involved. Age ranged from 3 to 12 years with a mean of 7.19 ± 2.489 years. Highly significant relation existed between grade 4 adenoid hypertrophy and mucoid nature of middle ear fluid (P value = .000). There is a highly significant relation between adenoid hypertrophy grade Ⅳ and type B tympanometry. There is a highly significant relation between adenoid size and nature of middle ear fluid irrespective of the duration of complaints, where grade Ⅳ adenoid hypertrophy showed more increase in middle ear effusion viscosity making adenoid size a very important predictor for the tympanometry type and the nature of the fluid in the middle ear.
Introduction
Otitis media with effusion (OME) is defined as the presence of fluid in the middle ear with the absence of criteria of acute middle ear infections. 1 Serous or mucoid fluid tends to accumulate in the middle ear due to negative pressure. Otitis media with effusion is one of the most common causes of diminished hearing. Prevalence of OME ranges from 1.3% to 31.3%, depending on the research methodology, racial, and environmental factor. 2
Adenoid hypertrophy and Eustachian tube dysfunction are known etiological factors for OME. 3 Adenoid acts as a reservoir for bacteria as well as a mechanical barrier that blocks the Eustachian tube lumen leading to formation of negative pressure in the middle ear resulting in middle ear effusion. 4
Different studies showed that the risk of OME increases with increasing nasopharyngeal obstruction and adenoid size seen either by X-ray or nasoendoscopy findings or both. 5,6 Different endoscopic grading systems for adenoid hypertrophy have been introduced in the literature depending on its relation to the choanae, 7 Vomer, 8 or torus tubarius, vomer, and soft palate. 9
Middle ear effusions are classified into different categories according to their viscosity. Differentiation between serous and mucoid types of effusion is usually done in the clinical practice. It was found that serous effusion contains more bacteria than the mucoid effusion. 10 Serous type is usually more easily treated than the mucoid type which usually needs surgical interference.
This study aims at finding whether there is a correlation between increasing adenoid size in cases of OME and the type of fluid in the middle ear in pediatric population aged 12 years and less which can help in suggesting the proper way of management.
Methods
This is a prospective study done in our hospital from July 2015 till July 2017 on 100 patients with chronic otitis media with effusion (COME) documented with a tympanometry test result of either type B or type Cs and adenoid hypertrophy documented by endoscopic examination by 2.4-mm fiber optic scope after application of 0.5% of the xylocaine topical nasal spray. Local ethical committee approval was obtained, and informed consent had been taken from all patients’ guardians. A grading system for adenoid size had been used in this study, depending on the adenoid relation to torus tubarius, vomer, and soft palate when at rest. 9
According to this protocol, 4 grades of adenoid hypertrophy had been documented, where grade Ι represents no relation between the small adenoid and any of the structures mentioned, grade Ⅱ represents relation with torus tubarius only, grade Ⅲ represents relation with torus tubarius and vomer, while grade ΙV represents that adenoid has relation with torus tubarius, vomer, and soft palate.
Diagnosis of OME was based on clinical findings of dull retracted unilateral or bilateral ear drum/s and unilateral or bilateral type B and Cs tympanometry. Type C was considered as no fluid in the middle ear. Tympanometry in this study has been performed with an impedance audiometer A756 screening (Italy, 2006 model).
In order to avoid disease duration bias, a fixed duration of—no response to medical treatment— 3 months had been used in all cases irrespective of the adenoid size.
All the cases were subjected to adenoidectomy and myringotomy with or without ventilation tube insertion. Correlation between the type of tympanometry result and adenoid size had been studied as well as relation between the type of fluid in the middle ear observed during the surgical procedure and adenoid size. For clinical purposes, we categorized the fluid in the middle ear into 2 types: serous where the fluid is thin and mucoid where the fluid is thick, heavy, and sticky.
Inclusion Criteria
Pediatric population aged 12 years or less.
No recent upper respiratory tract infection.
Proof of middle ear effusion documented by tympanometry type B or Cs.
Adenoid hypertrophy documented by the endoscopic examination.
Patients whose guardians gave the consent for surgery and study.
Exclusion Criteria
Refusing consent for the study.
Any contraindication for surgery as cleft palate or blood dyscrasias.
Statistical Analysis
Quantitative data were presented as mean, standard deviation, and percentage; χ2 test was used to compare between the different grades of adenoid hypertrophy. Statistical significance was determined as P < .05 using SPSS, version 21 (SPSS Inc, Chicago, Illinois). We used phi coefficient to detect the strength of correlation, where values between 0.3 and 0.7 represented a weak positive correlation and values between 0.7 and 1.0 represented a strong positive correlation.
Results
This is a prospective study that has been done in our hospital in the period from July 2015 till July 2017. It included 100 pediatric patients aged 12 years and less. All the cases had unilateral or bilateral type B or Cs as seen from the tympanometry done repeatedly during the medical treatment period for their condition. All the cases had adenoid hypertrophy, which had been graded according to the endoscopy grading system used.
Age of included patients ranged from 3 to 12 years with a mean age of 7.19 ± 2.489 years. There were 40 females and 60 males included in the study. Type C tympanometry was found in 12 of 100 right ears and 2 of 100 left ears. Type Cs tympanometry was found in 50 of 100 right ears and 25 of 100 left ears.
The most frequent tympanometry type was type B which was encountered in 38 of 100 right ears and 73 of 100 left ears. Unilateral disease was encountered in 14 cases, while bilateral disease was found in 86 cases. In this study, grade Ι adenoid hypertrophy was not encountered, while grades Ⅱ, Ⅲ, and ΙV presented in 29, 19, and 52 cases, respectively.
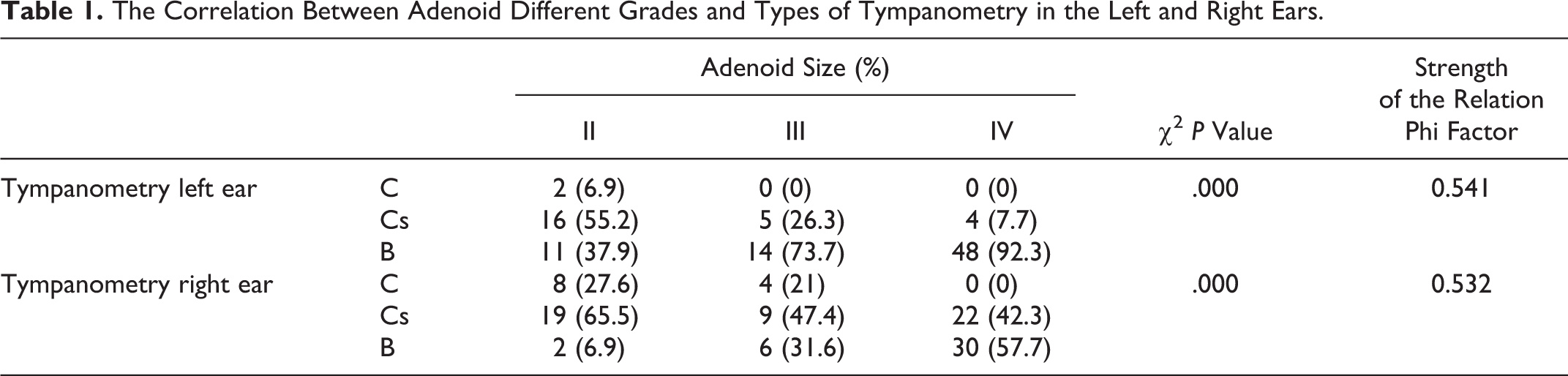
In this study, we found 34 cases with serous middle ear effusion, despite the tympanometry type and 66 cases with mucoid middle ear effusion. Adenoid grade ΙV showed a highly significant correlation with type B tympanometry, and with increasing the size of adenoid, there was a noticeable change in tympanometry result from C to Cs then B curves (Table 1; Figures 1 and 2).
The Correlation Between Adenoid Different Grades and Types of Tympanometry in the Left and Right Ears.
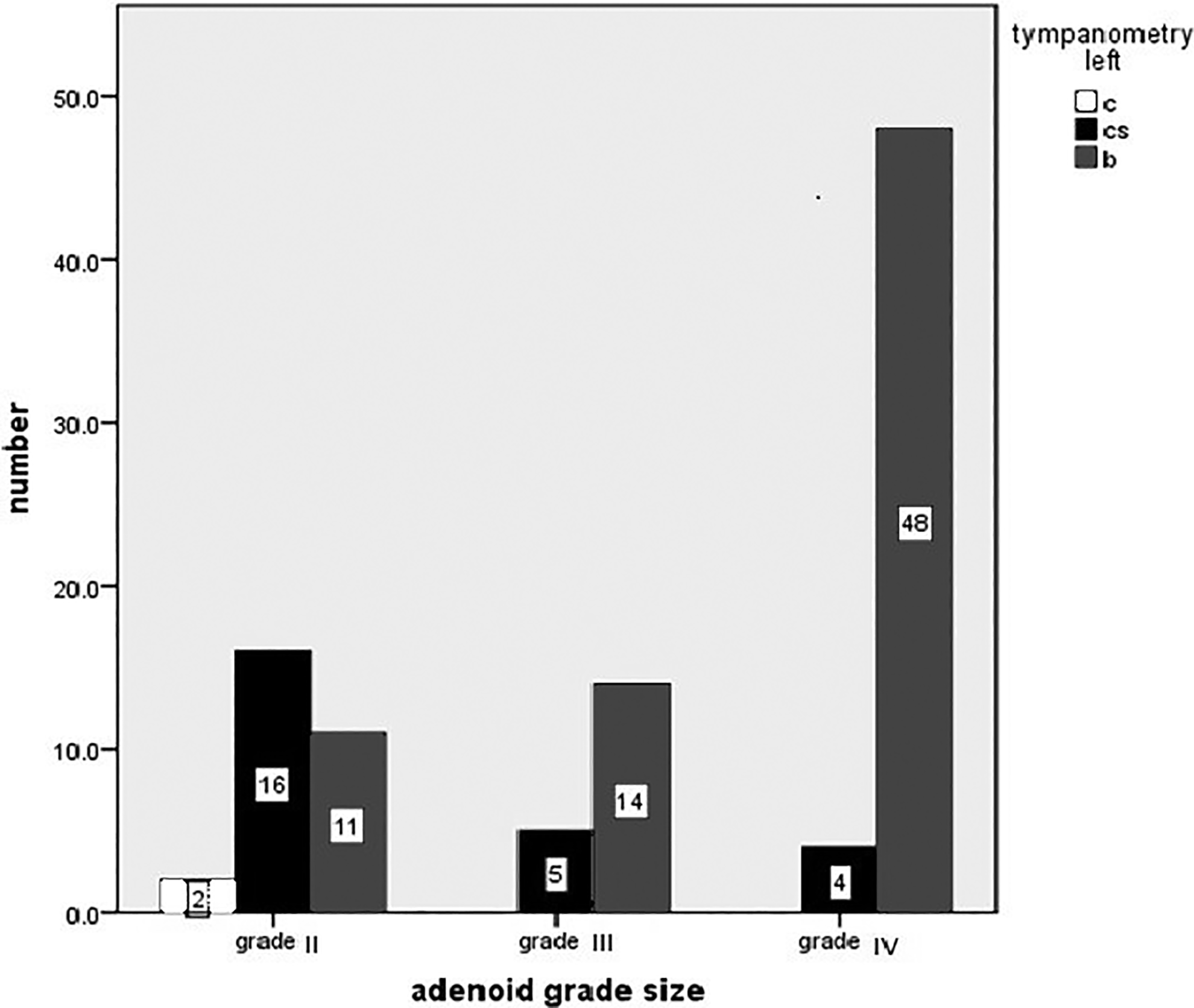
Correlation between adenoid size and tympanometry results in the left (Lt) ear.
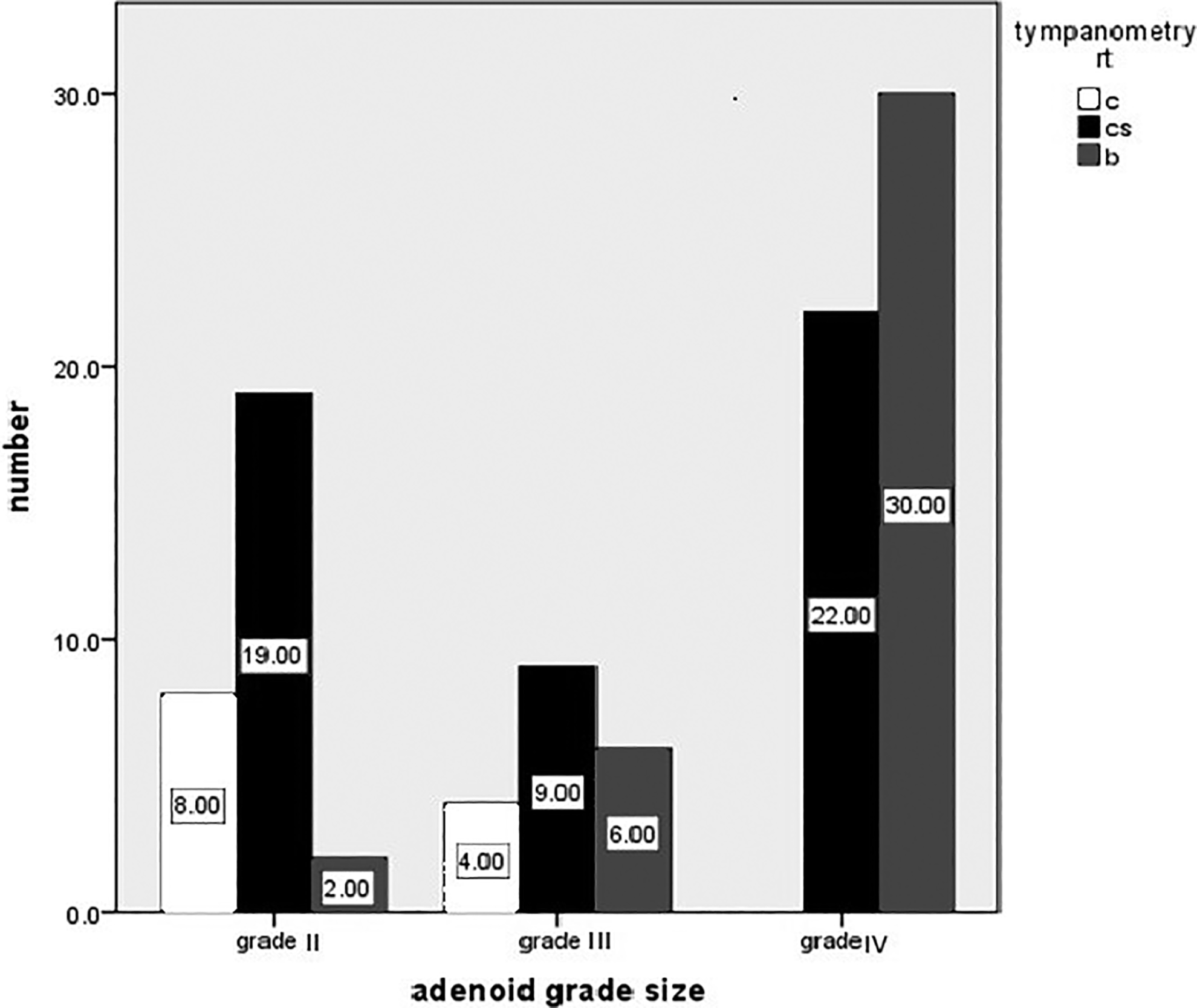
Correlation between adenoid size and tympanometry results in the right (Rt) ear.
In this study, there was a highly significant correlation between mucoid type of effusion and grade ΙV adenoid size. Also, it was noticeable that with increasing the adenoid size, there was a change in the fluid type from serous to mucoid type (P value = .000 and strong positive correlation seen by phi coefficient factor; Table 2; Figure 3).
The Relation Between Serous and Mucoid Middle Ear Effusion and Adenoid Size.

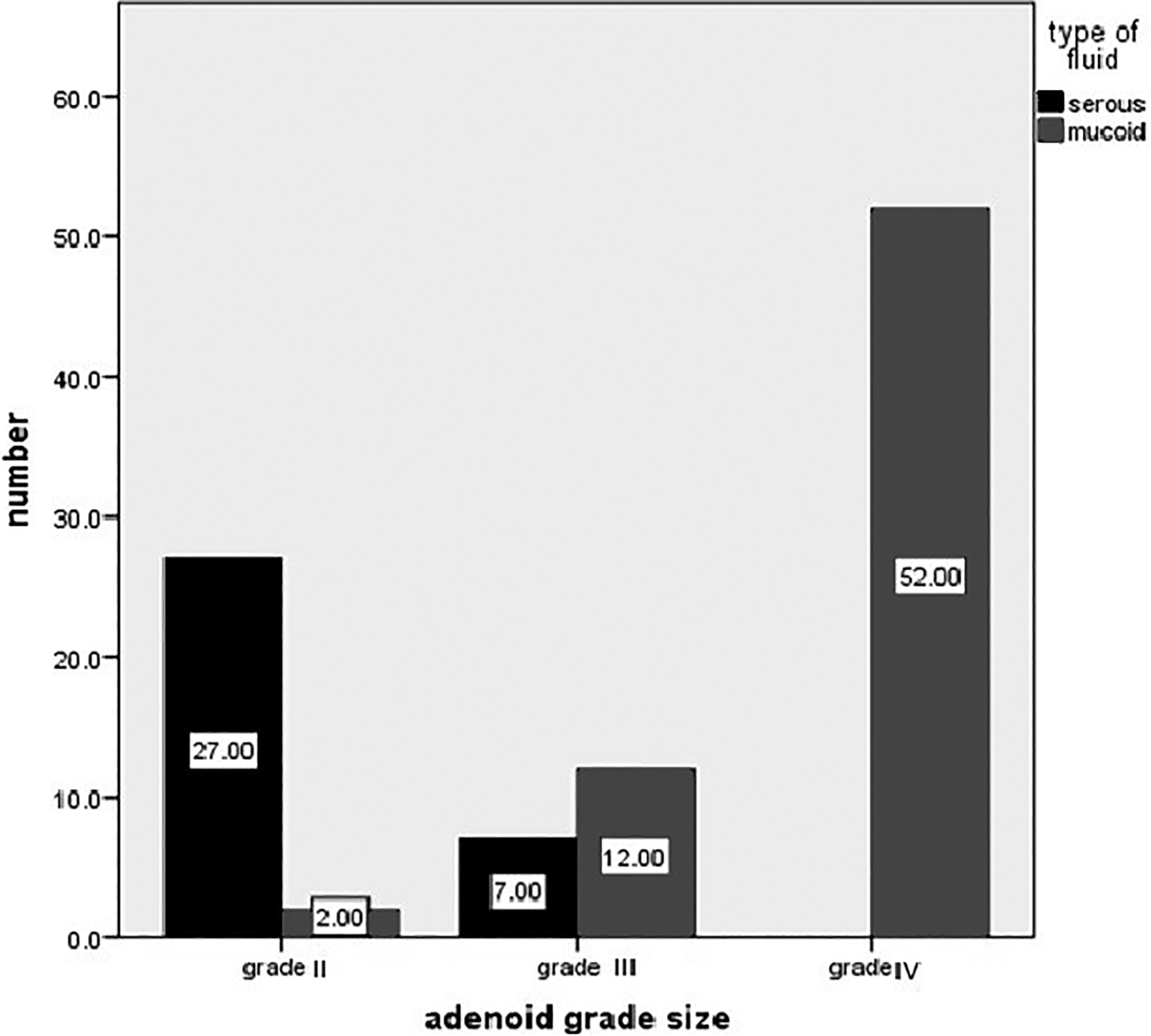
Correlation between adenoid size and type of middle ear fluid.
In the study, with more the size of the adenoid, the more frequent type B tympanometry and more encountered mucoid effusion of the middle ear, which suggests that with higher grades of adenoid size, we should suspect more viscosity of the fluid in the middle ear which will favor the surgical interference as the mainstay treatment method.
Discussion
Adenoid hypertrophy is a common problem in childhood. It plays an important role in pathogenesis of OME, a common cause of hearing impairment in young children. 11
Adenoids can cause OME by either mechanical obstruction of the Eustachian tube (ET) leading to negative pressure in the middle ear 12 or by acting as a reservoir for infection in upper respiratory tract infection with edema of pharyngeal opening of ET. 13
Duration of OME varies as it may be acute, which is less than 3 weeks, subacute which is between 3 weeks and 3 months, or chronic which is more than 3 months duration. 14
About 90% of children might have OME at sometime before school age which is more frequent between 6 months and 4 years of age. 14 The period of maximum lymphoid hyperplasia of the nasopharynx nearly coincides with the peak age of incidence of recurrent OME. 15
Tympanometry is one of the most useful quantitative measures for middle ear effusion. 16 Orchik et al considered type B tympanometry as the most sensitive and specific test in detecting middle ear effusion. 17 In this study, type B tympanometry was considered as evidence of fluid effusion in the middle ear. Type Cs also was considered as some fluid in the middle ear, while type A and C were considered normal.
Evaluation of adenoid size in the literature had been performed using lateral skull radiographs and by endoscopic direct visualization using rigid or flexible scopes. A radiological plain film is 2-dimensional study only leading to misinterpretation of adenoid obstruction in cases of only bulky lateral adenoid growth. Also, exposing the patient to radiation as well as errors from skull rotation or changes in palatal position with inspiration, expiration, or phonation can be considered as limitations of this method in detecting adenoid size. 9
Nwosu et al 18 in 2016 studied the tympanometric findings in children with adenoid hypertrophy, where they used the postnasal X-ray done for children and calculated the adenoid nasopharyngeal ratio proposed by Fajioka et al. 19 They graded the adenoid size using Sade method (from 0 to Ⅲ). 20
In the literature, many authors used the endoscopic grading for adenoid size and correlated that with OME. Acharya et al 21 used Cassano et al grading system 22 depending on choanal obstruction and fullness of nasopharyngeal space.
The fact of no exposure to radiation and 3-dimensional dynamic viewing of the adenoid by nasal endoscopy makes this method more preferred for evaluation of adenoid size and correlation with different surrounding structures. 9
Many authors had used endoscopic examination for grading of adenoid size and correlating with incidence of OME such as Vijayan et al 6 and Timna and Chandrika study 23 in 2018 used the Clemens and McMurray grading system 7 that depends on the adenoid size in relation to the posterior choana.
In this study, we used Parikh et al 9 grading system for adenoid size for better detection of the relation between adenoid hypertrophy and Eustachian tube. The age of patients ranged from 3 to 12 years with a mean age of 7.19 ± 2.489 years. Peak age was from 5 to 7 years and from 5 to 10 years in Timna and Chandrika study 23 and Vijayan et al study, 6 respectively.
In our study, females were 40% of the study group with the rest 60% of the study group were males, making a more incidence in male group than the female group, while there was no definite report in the literature stating that COME is affected by gender of patients. 6
In this study, 14% of cases presented with unilateral COME, while 86% of cases showed a bilateral disease. This comes in contrast to Nwosu et al study, where unilateral cases reached up to 27% of the cases included in their study. 18
In Vijayan et al and in Timna and Chandrika studies, 6,23 COME was present in only 2 of 35 and 0 of 30 cases with grade Ι adenoid hypertrophy, respectively. In our study, grade Ι adenoid hypertrophy was not encountered in all the cases of COME. This can be explained by the fact that in grade Ι adenoid hypertrophy using either Clemens and McMurray classification or using Parikh et al classification, the small adenoid has no relation to the Eustachian tube.
In this study, grade Ⅳ adenoid hypertrophy showed a highly significant correlation with type B tympanometry either as unilateral or as bilateral finding. This comes in contrast to Timna and Chandrika study, where grade Ⅲ adenoid hypertrophy showed higher number of cases of COME. 23 Vijayan et al stated that with increasing the grade of adenoid size, the more chance of fluid level and COME, where they found that grade Ⅳ adenoid hypertrophy was associated with a more likely incidence of OME. 6 Using the X-ray findings for adenoid size, Nwosu et al found that the more the size of adenoid, the more cases of COME. They found that grade 3 adenoid hypertrophy is associated with higher incidence of OME. 18
With more the lesions abutting torus tubarius, the more likely the incidence of OME and more likely the need for adenoidectomy to relieve the hazardous effect of adenoid on the ear. 23 This comes as a support for this study, where with increasing the grade of adenoid size and consequently, the relation and proximity to torus tubarius, the more likely the affection with COME.
Lateral extension of adenoid was associated with more incidence of OME, where 60% of cases had been found to have laterally placed adenoids encroaching on the Eustachian tube and was also a support for our study. 24
According to Acharya et al study, grade 4 adenoid hypertrophy was the only significant one associated with high incidence of OME in children. 21 On the other hand, another study denied the future effect of adenoidectomy on recurrence of OME in children less than 4 years. 25
Maw et al stated that after 12 and 24 months follow-up period for cases of serous and mucoid effusion, there were no significant changes in the hearing threshold supporting the idea of no prognostic value of fluid thickness on the disease effects over time. 26 Acharya et al stated that there was no correlation between thickness of the fluid and the hypertrophied adenoid. 21
In this study, there was a highly significant correlation between the higher grades, especially grade ΙV adenoid hypertrophy with the viscosity of the fluid in the middle ear in cases of COME, where grade ΙV showed a highly significant correlation with mucoid type of effusion while grade II adenoid hypertrophy showed correlation with more incidence of Eustachian tube dysfunction documented by type C tympanometry.
Conclusion
This study confirms the high correlation between adenoid size and incidence of OME. There is a highly significant relation between grade Ⅳ adenoid hypertrophy and tympanometry type B. In this study, there is a highly significant relation between adenoid hypertrophy grade Ⅳ and mucoid type of middle ear effusion. With more increase in the adenoid size, more viscosity of middle ear effusion was detected.
Footnotes
Acknowledgments
The authors would like to thank Dr Enas M. Fawzy, Head of Statistical Department, National Nutrition Institute, Cairo, Egypt for her help with the statistical part of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.