
Abstract
Introduction:
First bite syndrome (FBS) is a rare but potentially debilitating complication observed after surgery involving the upper cervical region. Patients classically complain of severe facial pain in the ipsilateral parotid region with the first few bites of a meal.
Objective:
The aim of this study is to shed light on the incidence and potential risk factors of FBS, including a series of cases depicting FBS observed after parotidectomy.
Methods:
Retrospective review of 419 patients who underwent parotidectomy at a single tertiary care facility between December 2016 and June 2020.
Results:
With a mean follow-up time of 16.5 months, 8 (2%) patients were documented to have symptoms of FBS after parotid gland surgery. Six of these patients underwent partial parotidectomy by dissection of the deep lobe of the parotid (DLP).
Conclusion:
Patients undergoing dissection of the DLP are particularly at risk for the development of FBS. All patients should be appropriately counseled during informed consent discussions, especially in high-risk cases.
Keywords
Introduction
First bite syndrome (FBS) is a recognized complication after surgery involving the upper cervical region, including dissection of the deep lobe of the parotid (DLP), parapharyngeal space (PPS), or infratemporal fossa (ITF). 1 The diagnosis of FBS is purely clinical and based on patient history. It is classically characterized by sharp pain in the ipsilateral parotid region experienced with the first bite of each meal. These bursts of pain are said to be short-lived and to diminish with subsequent bites, though severe cases may interfere with an individual’s ability to tolerate oral intake. In this way, FBS can have a dramatic negative impact on the health and quality of life of affected patients.
Incidence and risk factors for FBS are relatively unknown; however, patients at particular risk are those undergoing procedures in which the sympathetic innervation of the parotid gland is interrupted. In order to achieve a better understanding of this rare pain syndrome, we provide a series of cases depicting FBS after parotidectomy. We aim to shed light on the incidence and risk factors for FBS based on our institutional experience.
Patients and Methods
Following approval by the institutional review board of Thomas Jefferson University Hospital, a retrospective review was conducted of all patients who underwent parotidectomy for histologically confirmed parotid gland pathology (n = 419). Patients who presented to our institution between December 2016 and June 2020 were reviewed. Only those who experienced symptoms of FBS postoperatively were included. Data regarding demographics, preoperative evaluation, extent of parotidectomy, reconstructive techniques, tumor size and pathology, postoperative complications, and date of last follow-up with otolaryngology were collected.
Results
Among 419 patients who underwent parotidectomy, 8 developed FBS (incidence 2%). All patients with FBS underwent partial parotidectomy, by dissection of either the deep or superficial lobe of the parotid. From 48 patients who underwent partial parotidectomy with DLP dissection, 6 developed FBS (incidence 12.5%). An equal distribution of men (4, 50%) and women (4, 50%) were included with a mean age of 49 years (range: 34-73 years). Average hospital length of stay was 1 day (range: 0-2 days). Average time from surgery to symptom onset was 28 days (range: 6-102 days). One patient received treatment for FBS (Table 1). Seven (87.5%) patients reached resolution of FBS throughout follow-up, with an average duration of 192 days (range: 28-534 days). One patient was still being observed for mild FBS 645 days after surgery. Average length of follow-up was 16.5 months (range: 3.3-39.5 months).
Patient Characteristics.
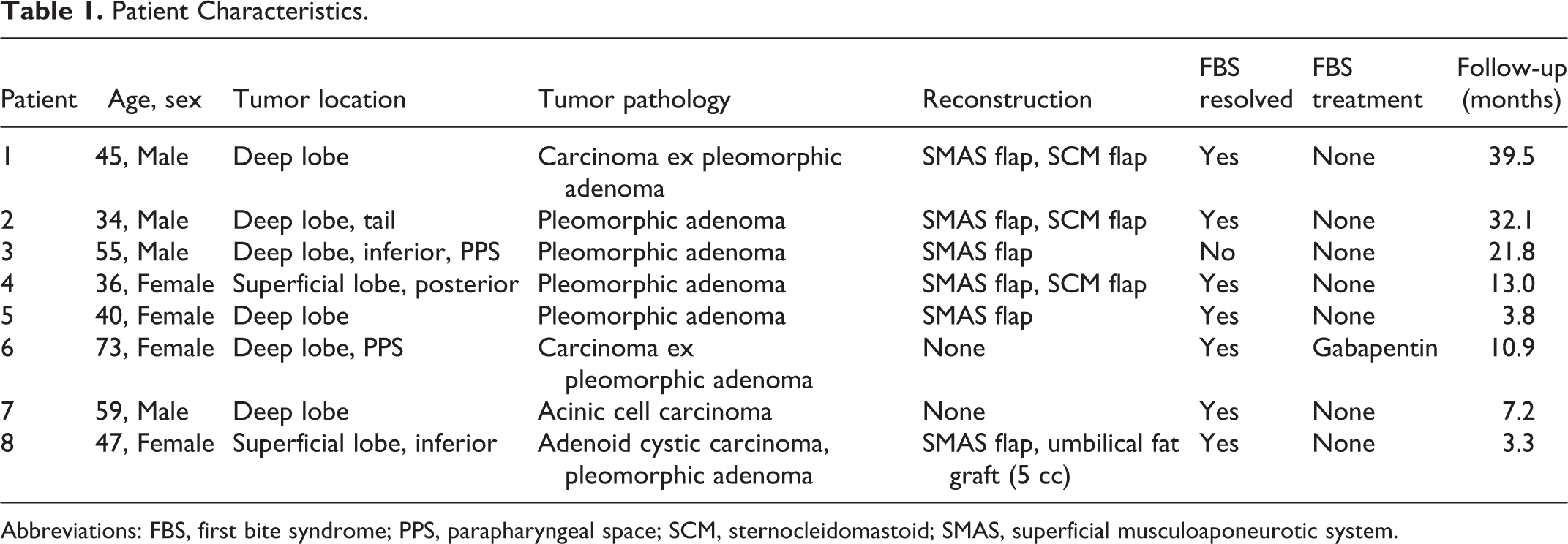
Abbreviations: FBS, first bite syndrome; PPS, parapharyngeal space; SCM, sternocleidomastoid; SMAS, superficial musculoaponeurotic system.
Case #1
A 45-year-old male presented with a right-sided parotid mass that he first noticed a few weeks prior. He denied pain, change in mass size, or other symptoms. Past medical history included basal cell carcinoma of the right temple that was excised 6 years ago and current smoking history. Fine needle aspiration (FNA) revealed pleomorphic adenoma. A 2.7 × 1.6 cm pleomorphic adenoma was excised from the DLP with superficial musculoaponeurotic system (SMAS) and sternocleidomastoid (SCM) flap reconstruction. The pathology report further revealed a 0.2 × 0.2 focus of carcinoma ex pleomorphic adenoma confined within the capsule of the larger tumor, staged T1Nx.
At 3.4 months postoperatively, he began to complain of a mild, sharp pain in the right parotid region with the first bite of a meal. This patient’s FBS was observed without treatment and gradually resolved by 20.9 months follow-up.
Case #2
A 34-year-old male presented for evaluation of a right parotid gland mass found incidentally on magnetic resonance imaging performed for new-onset left-sided headaches. He complained of pain with palpation and otherwise denied associated symptoms. Fine needle aspiration suggested pleomorphic adenoma. The patient underwent excision of a 3.3 × 2.6 × 2.0 cm pleomorphic adenoma of the DLP with SMAS and SCM flap reconstruction.
The patient returned on postoperative day 6 (POD#6) complaining of intermittent right-sided facial pain with eating and facial edema and was given a course of prednisone. On POD#13, he presented to the emergency department (ED) with a surgical site seroma, which was incised and drained. Throughout follow-up, the patient only complained of mild symptoms of FBS, which resolved without treatment by 3.6 months postoperative.
Case #3
A 55-year-old male with a history of transcervical and transoral robotic excision of a right PPS pleomorphic adenoma presented with a new neck mass concerning for recurrence. He denied pain or other associated symptoms. Fine needle aspiration suggested low-grade basaloid neoplasm. A 1.5 × 2.0 × 1.4 cm pleomorphic adenoma was excised from the right PPS and inferior DLP. Superficial musculoaponeurotic system flap reconstruction was performed.
On POD#19, the patient began to complain of intense pain in the right parotid region with the first few bites of a meal. At 3.4 months follow-up, treatment options including gabapentin and Botox were discussed; however, he elected for continued observation. At 21.8 months postop, he continued to defer treatment due to the mild nature of symptoms.
Case #4
A 36-year-old female who was seen in Urgent Care for a left-sided parotid mass presented for surgical evaluation. She denied any symptoms associated with the mass. Fine needle aspiration was consistent with pleomorphic adenoma. A1.4 × 1.1 × 1.0 pleomorphic adenoma was excised from the posterior superficial lobe of the left parotid gland with SMAS and SCM flap reconstruction.
On POD#8, she returned with mild symptoms of FBS and was encouraged to massage the area. At 1.2 months follow-up, in-office surgical correction of buckling skin in the left preauricular area was performed, but she no longer complained of FBS symptoms.
Case #5
A 40-year-old female presented for evaluation of a left-sided parotid mass that had been present for 4 years with a mild increase in size over the past 10 months. She complained of mild soreness near the mass and mild left-sided otalgia. Fine needle aspiration demonstrated pleomorphic adenoma. A 3.0 × 2.1 × 1.5 cm pleomorphic adenoma was excised from the left DLP with SMAS flap reconstruction.
At 1.9 months follow-up, she reported moderate left-sided facial pain that was worse when taking the first bite of food. A course of gabapentin was offered, but the patient declined. By 3.8 months follow-up, her symptoms had resolved.
Case #6
A 73-year-old female with a former 45-pack-year smoking history and known right PPS mass presented for evaluation. The mass had been stable for 6 years without associated symptoms, but the patient reported recent onset of hoarseness, globus sensation, dysphagia, cough, and throat discomfort. She underwent excision of a 3.5 × 3.0 × 2.7 cm mass from the right PPS with DLP dissection. Frozen section revealed carcinoma ex pleomorphic adenoma, and a right-sided neck dissection of levels 1B, 2A, 2B, and 3 was performed. The tumor was staged T3N0, and adjuvant radiation therapy was recommended.
On POD#11, she reported right-sided shooting jaw pain with chewing, ranging from 7/10 to 10/10 in severity. She was observed and maintained on a soft diet. At 7 months postop, gabapentin 100 mg three times daily was prescribed for persistent FBS. Due to concern for recurrence or residual disease on postoperative imaging scans, she was taken to the operating room for exploration of the right neck with PPS biopsies. Pathology returned negative, but she continued to complain of dysphagia, neck pain and tightness, right-sided facial pain, and intermittent right otalgia. It was unclear whether these symptoms represented sequelae of radiation therapy or cancer-related pain. At 9.6 months postop, the patient presented to the ED with acute-onset right-sided cranial nerve 6 palsy. Imaging was negative for acute stroke but significant for extensive atherosclerosis and skull base tumor recurrence. The tumor was restaged as T4bN0M1. At 10.8 months postop, she had received 2 doses of systemic ado-trastuzumab emtansine and her pain, including FBS, had improved.
Case #7
A 59-year-old male presented for follow-up of a right-sided parotid mass that was incidentally seen on imaging following a motorcycle accident. He denied associated symptoms, and FNA was inconclusive. A 1.5 × 1.2 × 1.2 cm mass was excised from the right DLP. Frozen section revealed acinic cell carcinoma, staged T1Nx.
On POD#7, the patient presented to his local ENT for drainage of surgical site seroma. On POD#8, he reported mild right-sided facial discomfort with chewing. His symptoms, including twinges of pain in the right periparotid region, gradually resolved without intervention by 7.2 months postop.
Case #8
A 47-year-old female presented for evaluation of a left-sided parotid mass noticed 3 months prior, persistent despite a course of Augmentin. She complained of intermittent left otalgia and pain with palpation of the mass. Fine needle aspiration was suspicious for adenoid cystic carcinoma. A left-sided superficial parotidectomy was performed, including excision of a 1.2 × 1.2 × 1.0 cm T1N0 adenoid cystic carcinoma and a separate 0.6 × 0.6 × 0.3 cm pleomorphic adenoma. Reconstruction was performed by SMAS flap and umbilical fat graft (5 cc).
On POD#8, the patient complained of sharp left-sided periparotid pain that she experienced with the first 1 to 2 bites of a meal and occasionally at nighttime. No treatment was offered, and her FBS resolved by 3.3 months postop.
Discussion
While the incidence of FBS remains low, it should be recognized as a complication of parotid gland surgery, especially in procedures involving the deep lobe. We observed an incidence of 2% among all parotidectomies and 12.5% after partial parotidectomy with DLP dissection. This coincides with a review by Linkov et al, in which a 9.8% incidence of FBS was observed among 499 patients undergoing surgery involving the DLP, PPS, and/or ITF. 2 Furthermore, they found an incidence of 39.4% within patients who underwent isolated DLP resection. 2 Isolated dissection of the DLP should be considered a significant risk factor for development. Type of incision and reconstructive technique performed did not appear to play a role in the development of FBS at our institution.
Patients with FBS may present as early as a few days or as late as several months postoperatively. We observed an average time to presentation of 4 weeks, with a maximum time of 14.6 weeks. This variable time to presentation mirrors that observed in other studies3,4 and emphasizes that patients should be monitored for symptom development throughout the postoperative period. Duration of symptoms may be highly variable as well, but a large proportion of patients reach gradual resolution of symptoms within several months to 1 year. 5 Spontaneous resolution was observed in 7 (87.5%) of 8 patients included in this case series.
The exact pathophysiology of FBS remains unclear; however, it is hypothesized to be due to an interruption of the sympathetic innervation to the parotid gland. These fibers, along with parasympathetic fibers, control contraction of myoepithelial cells within the salivary glands to regulate saliva secretion.6,7 An interruption in the sympathetic system leads to denervation supersensitivity and upregulation of myoepithelial cell receptors within the parotid gland.1,3 Subsequent gustatory stimulation elicits a supranormal response from the intact parasympathetic fibers and causes excessive myoepithelial contraction. Furthermore, the first saliva to be secreted is the most viscous, as it has a high amylase and protein content. The combination of these 2 mechanisms leads to a sudden increase in intraluminal pressure of the parotid gland ducts that results in severe facial pain. 1
A review of the literature reveals multiple descriptions of FBS occurring as a complication of surgical procedures, including dissection of the DLP,2,8 dissection of the PPS,9,10 carotid endarterectomy,5,11 and other surgery of the upper cervical region.3,12-16 Although postoperative FBS represents more than 95% of the cases published, 4 FBS due to tumor17,18 and FBS of unknown etiology1,19 have also been described. Previously cited risk factors include injury to the superior cervical ganglion and ligation or resection of part of the ECA causing damage to the surrounding sympathetic plexus. 10
A consistently effective treatment regimen for FBS has not been well established, but the most promising treatment described thus far is Botulinum toxin injections into the parotid gland.4,9,20-22 Additional medical therapy includes anticonvulsants (carbamazepine, gabapentin, pregabalin), which may minimize pain severity and duration. Those wishing to avoid medical therapy may try eating bitter or sweet foods before salty or sour. 1 This method aims to suppress salivary secretion and prevent the sudden increase in parotid ductal pressure. 16 Another documented dietary strategy includes gargling Rikkosan prior to meals. As a type of traditional Chinese medicine classically used in the treatment of orofacial pain, Rikkosan has both local anesthetic properties and a bitter taste, which suppresses taste stimulation. 1 At our institution, patients are counseled on the high likelihood that FBS symptoms may diminish over time without intervention, and many improve with observation alone. For those with severe or persistent symptoms, medical treatment in the form of Botox injections or anticonvulsants such as gabapentin or carbamazepine is offered. Choice of treatment is made based on individual preferences, medical history, and contraindications. Ultimately, the goals of treatment for patients with FBS should include pain management, maintenance of oral intake, and preservation of quality of life.
We acknowledge the limitations of this study, including those that are inherent to a retrospective design. Additionally, these cases were performed at a single institution and outcomes may not be representative of the entire population.
Conclusion
First bite syndrome is a rare but potentially debilitating complication that occurs due to interruption of the sympathetic innervation to the parotid gland. Although some patients experience self-limited disease, others have severe chronic pain. Treatment options include Botox injection, anticonvulsants, and dietary strategies; however, a treatment regimen that consistently provides relief has yet to be established. We propose partial parotidectomy with dissection of the DLP as a significant risk factor for the development of postoperative FBS. All patients, especially those at particularly high risk, should be counseled appropriately during informed consent discussions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.