
Abstract
Objective:
A case of primary first bite syndrome (FBS), diagnosed in a patient with nonspecific adenocarcinoma of the deep lobe of the parotid gland.
Data Sources:
A Medline literature search was conducted on PubMed, using the keywords “first bite syndrome.”
Review Methods:
Using primary FBS and existence of a definite etiology as inclusion criteria.
Results:
We report on an unusual case of primary FBS, which had no surgical history. After multiple examinations, the pain was localized to a mass in the deep lobe of the parotid gland. After tumorectomy, the FBS pain was significantly relieved. The postoperative pathological examination determined that the excised mass was a nonspecific adenocarcinoma. Reviewing the literature, we found that primary FBS was mostly caused by malignant tumors in the inferior temporal fossa, the deep lobe of the parotid gland, and (or) the parapharyngeal space. Surgery was reported to be an effective treatment.
Conclusion:
The case highlights the critical importance of identifying the etiology of primary FBS. When manifested with a primary FBS, malignant tumors must be high on the differential diagnosis list, especially those in the region of the inferior temporal fossa, the deep lobe of the parotid gland, and the parapharyngeal space.
Keywords
Introduction
First bite syndrome (FBS) presents as intense, electric shock–like pain in the parotid region after the first bite of each meal. This pain subsides with each subsequent bite. Although generally focused around the parotid gland, the pain might extend toward the ear. It is usually reported as a minor pain syndrome, yet FBS has a significant effect on both the quality of life and the physical health of the patients.1,2
First bite syndrome is usually considered an early postoperative complication in patients with head and neck cancer. The prevalence of this type of FBS is about 9.6%. 3 First bite syndrome without a history of surgery, termed primary FBS, is extremely rare. This type of FBS is often caused by tumors. If the tumor is malignant and is not detected and treated early enough, it might lead to local tissue infiltration and distant metastases, further affecting the health of the patients. Regardless of whether the tumor is benign or malignant, its surgical resection is often an effective treatment. For malignant tumors, postoperative radiation and/or chemotherapy is often required.
Because of its scarcity, we report here of a case of primary FBS that was caused by nonspecific adenocarcinoma in the deep lobe of the parotid gland. Through this report, we extend the rather meager available information regarding the etiology and treatment of primary FBS.
Materials and Methods
Ethical Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (name of institute/committee) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. This article does not contain any studies with human participants performed by any of the authors.
Case Report and Literature Review
Here, we report of a 58-year-old man with primary FBS. A Medline literature search was conducted on PubMed, using the keywords “first bite syndrome.” A total of 338 articles were retrieved. Using primary FBS and existence of a definite etiology as inclusion criteria, 6 articles, reporting on 6 patients, were included (Figure 1).
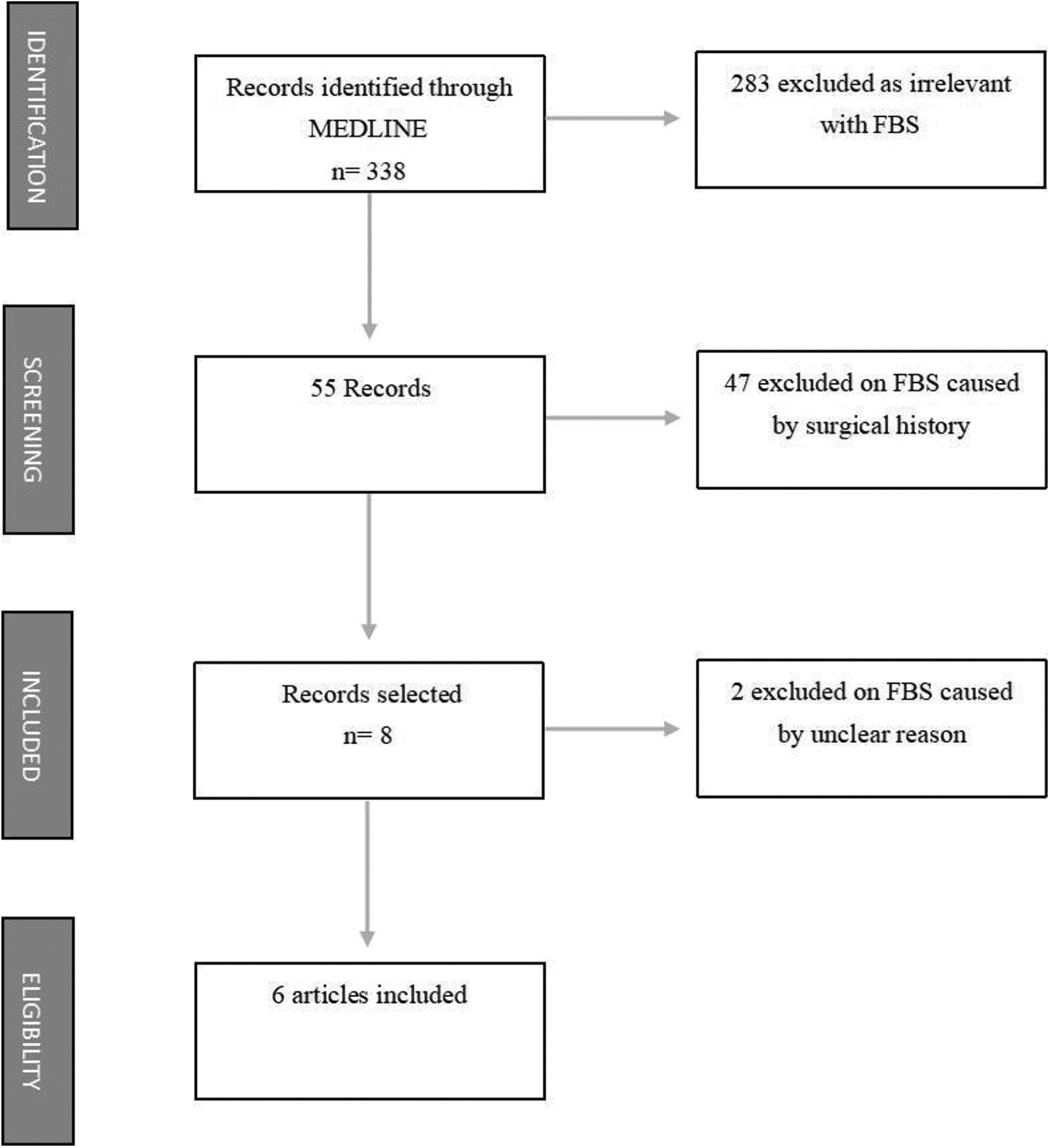
Flowchart.
Results
Case Report
A 58-year-old man was referred to our hospital in April 2019. He presented with a 5-month history of right facial pain upon the first bite of each meal. The patient complained of excruciating and electric shock–like pain on the right side of the face during the first bite of each meal. The pain episodes lasted, on average, a few seconds and he could then finish his meal without pain. On his first visit to the local doctor 5 months earlier, his symptoms were suspected to be secondary to temporomandibular joint dysfunction. There was no relief of the pain after a series of conservative treatments. His medical history was negative for chronic diseases, previous head and neck surgery, or the presence of tumors.
Physical examination revealed no abnormal region or swelling in the temporal bone area, no sign of facial nerve dysfunction, no Horner’s syndrome, no palpable masses, and no lymphadenopathic lesions within the head and neck. The patient’s facial pain symptoms were consistent with “first-bite syndrome.” To further investigate the source of the symptoms, we performed enhanced magnetic resonance imaging (MRI) scans of his head and neck. The enhanced MRI scans showed a mass in the deep lobe of the right parotid gland, accompanied by surrounding soft tissue infection (Figure 2).
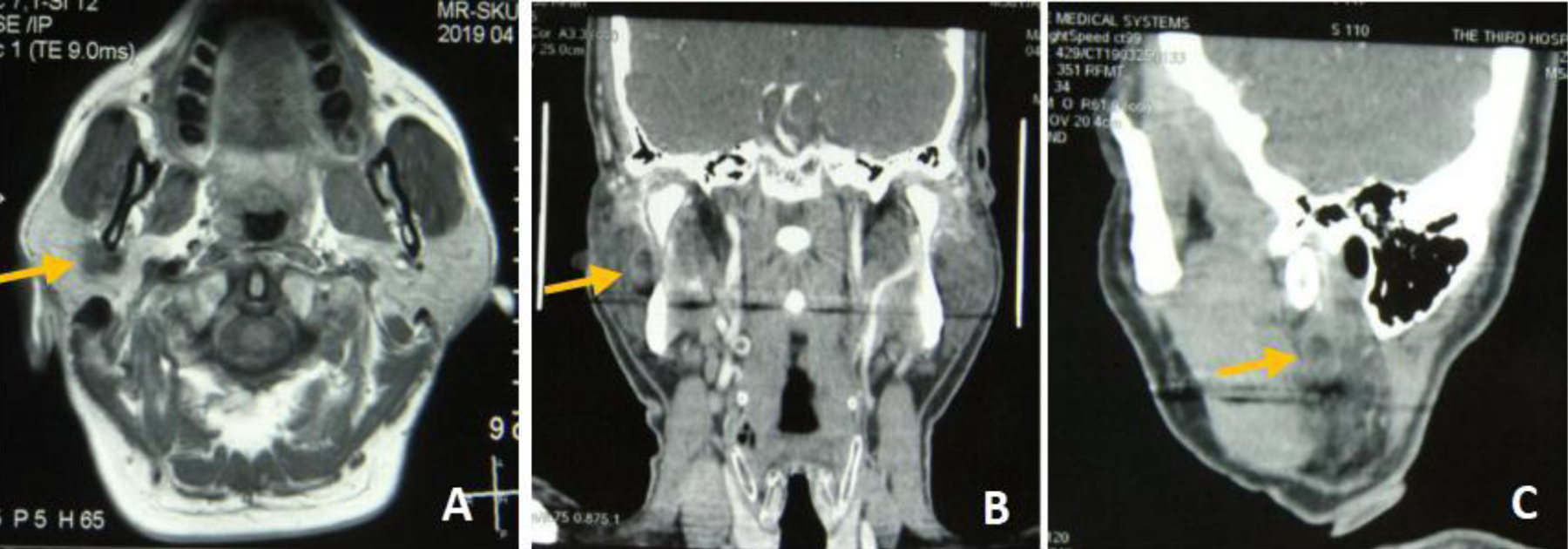
(A) Preoperative axial position (arrow). (B) Preoperative coronal position (arrow). (C) Preoperative sagittal position (arrow).
The patient underwent surgery under general anesthesia to resect the mass. Macroscopically, the tumor was firmly adherent to the undersurface of the main trunk of the facial nerve. Therefore, the mass was carefully dissected while preserving the nerve (Figure 3). During the surgery, the external carotid artery was sacrificed as it was completely engulfed by the tumor. Following the histopathological examination, the tumor was identified as a perineural nonspecific adenocarcinoma with gland and lymphovascular invasion (Figure 4).
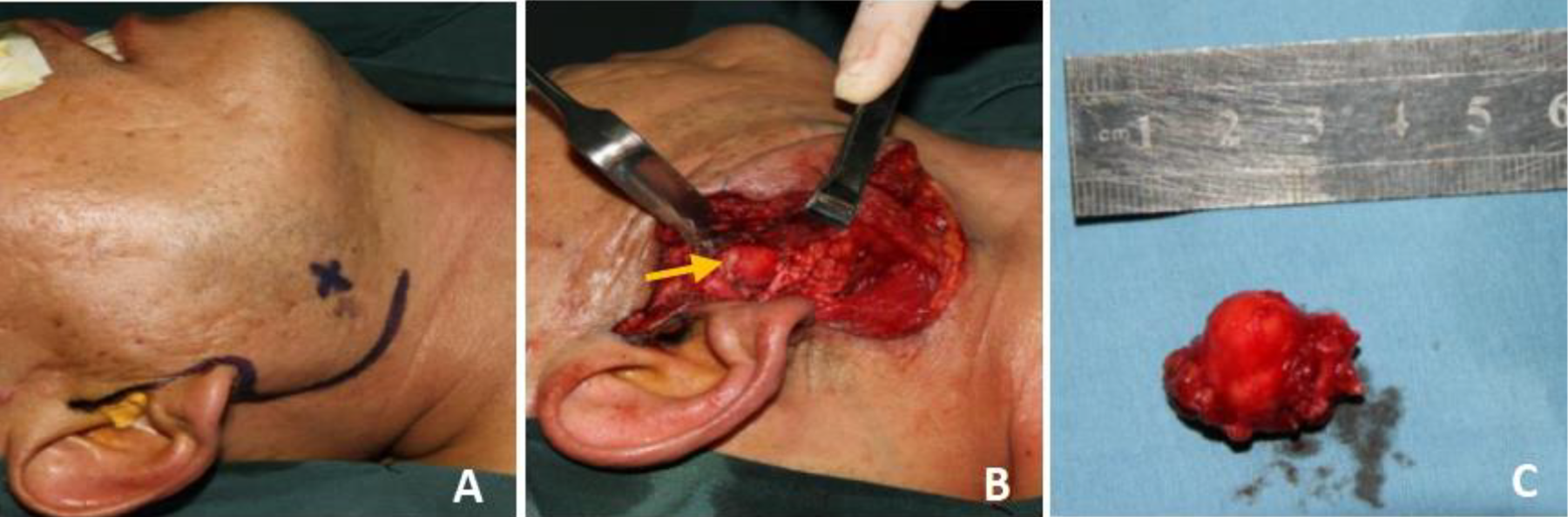
(A) Incision design. (B) The tumor was seen during the operation (arrow). (C) Complete resection of tumor.
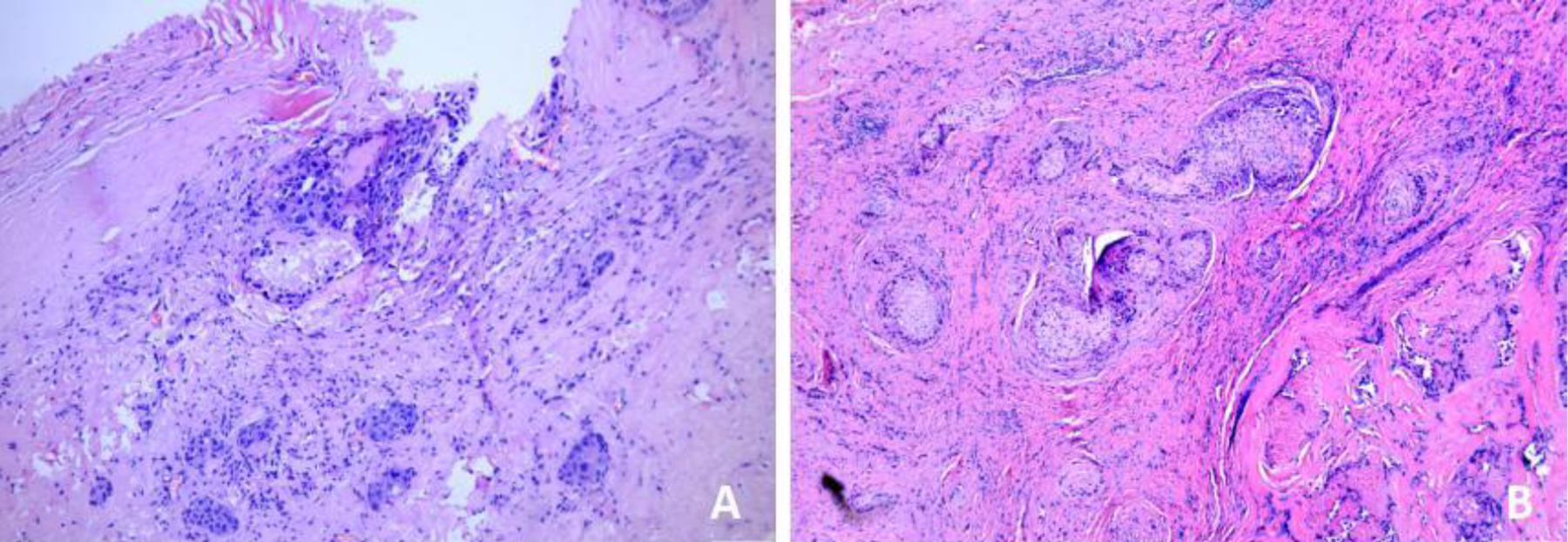
Photomicrographs showing (A) The nonspecific adenocarcinoma of right parotid. (B) The tumor invaded the normal glands and nerves.
After hospitalization for 5 days, the patient was discharged without any complications and complete and significant relief of the primary FBS pain. Since then, the patient has completed a course of postoperative radiation therapy. At the time of writing, almost one year after the surgery, the patient is still alive and with no symptoms or signs of relapse during clinical examination or imaging.
Literature Review of Primary FBS
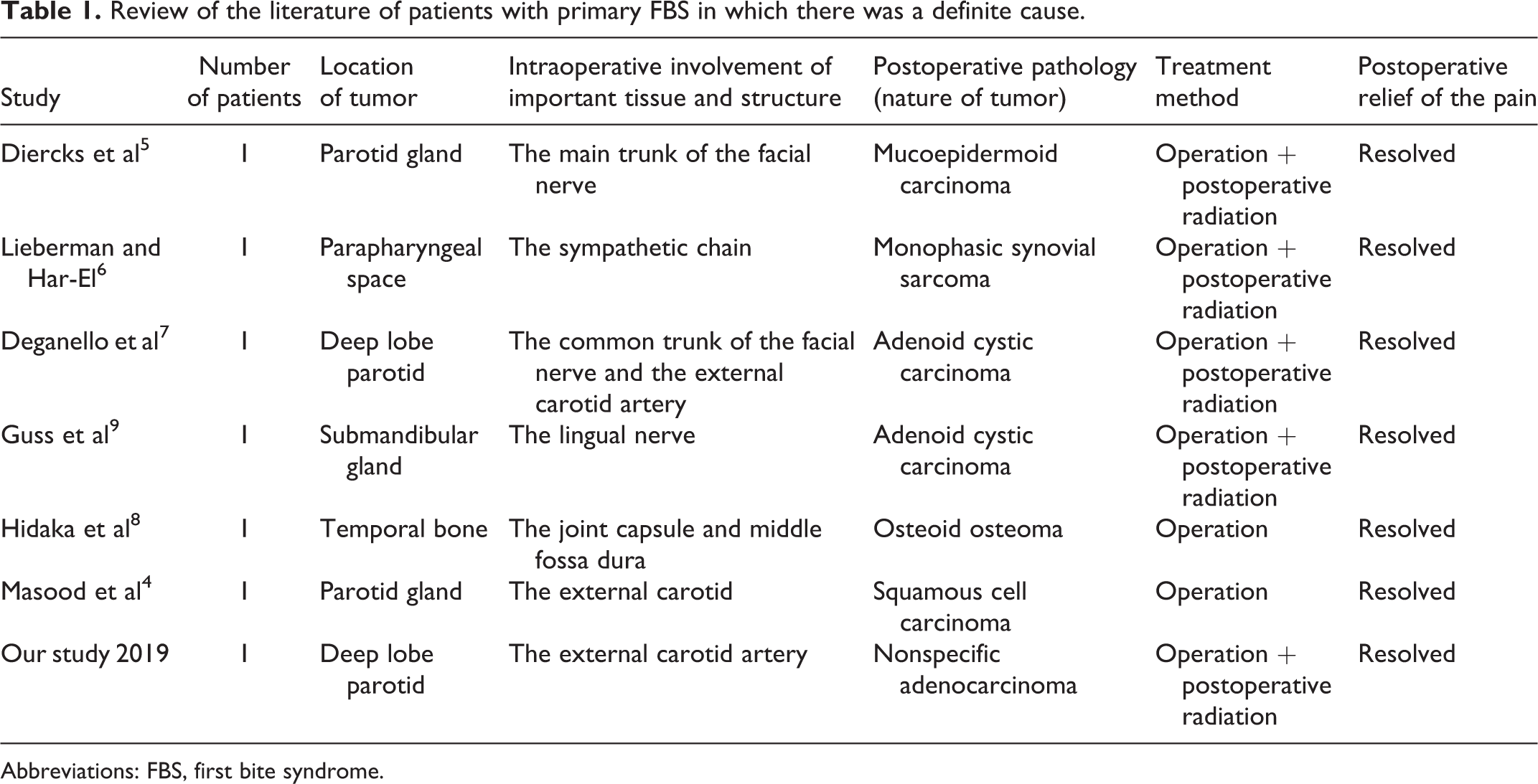
As shown in Table 1,4-9 6 cases of primary FBS were reported in the scientific literature. These were, respectively, 1 case each in the temporal region, the parapharyngeal space, and the submandibular gland, and 3 cases in the parotid gland, especially in the deep lobe of the gland. Of the 6 cases, one had a benign tumor, while all the rest had malignant tumors. During surgery, the tumors in 2 cases were found to be next to the main trunk of the facial nerve. In 2 cases, there was infiltration of the external carotid artery. In 1 case, the causing tumor was found to be directly associated with the sympathetic chain. In another case, the mass was adjacent to the lingual nerve. In the 6th case, the tumor was between the temporomandibular joint capsule and the middle fossa dura. After the surgery, 4 of the cases were resolved, in one case the FBS symptoms had diminished after the surgery but resolved completely 2 weeks later; and in the 6th case, the FBS symptoms continued after the surgery but resolved after radiotherapy. In our case, the external carotid artery passed through the malignant tumor. The FBS symptoms were resolved following surgical treatment.
Review of the literature of patients with primary FBS in which there was a definite cause.
Abbreviations: FBS, first bite syndrome.
Discussion
First bite syndrome is characterized by severe cramping or spasm in the parotid region, in association with the first bite of each meal. The pain diminishes during the subsequent bites. The intensity of the pain often makes it difficult for the patient to eat, and the resulting lack of nutrients can slow the healing of surgical wounds and might exacerbate cancer-related weight loss. In addition, due to the severe pain, patients have fear and anxiety, resulting in impaired subjective quality of life. The first description of FBS was published in 1986 by Haubrich, who linked the pathogenesis of FBS to deliberate or inadvertent resection of the superior cervical sympathetic ganglion during surgery in the parapharyngeal space. 10 The currently used description of FBS was published in 1998 by Netterville et al, 11 who proposed that FBS is due to sympathetic denervation of the parotid gland, with subsequent hypersensitivity and supramaximal response to parasympathetic neurotransmitter release after oral intake, inducing spasm of myoepithelial cells and therefore pain.
In our study, the pathogenesis of the primary FBS was associated with an underlying neoplastic process, in the absence of surgery. Although benign tumors might compress nerves, malignant ones might even invade them, especially when located near the inferior temporal fossa, the deep lobe of the parotid gland, or the parapharyngeal space. Compression or invasion of the nerve in such cases is likely to lead to the loss of sympathetic innervation of the parotid gland. This is equivalent to surgical resection of the cervical sympathetic chain or ligation of the sympathetic nerves as they course along the vasculature toward the parotid gland. In our case, FBS may have been caused by the tumor’s invasion or compression of the sympathetic nerve chain, which had disrupted the balance between the sympathetic and parasympathetic nervous systems supplying the parotid gland. The tumor, in this case, was found in the deep lobe of the parotid gland, and histopathology suggested that it had invaded the nerve.
Over 95% of FBS cases are complications of surgery in the inferior temporal fossa, deep lobe of the parotid gland, or the parapharyngeal space. 12 For surgery-derived FBS, treatment methods include observation and follow-up, 13 dietary adjustment,14,15 drug therapy,16,17 surgery,18,19 radiotherapy, 20 and acupuncture. 21 However, for primary FBS, determination of the precise etiology is the key to the selection of treatment. Malignant tumors must be high on the suspicion list, especially around the inferior temporal fossa, the deep lobe of the parotid gland, or in the parapharyngeal space. For further workup, it is necessary to use techniques such as imaging to seek definite etiology and decide on the appropriate treatment. If a tumor could not be found, close follow-up and repeated imaging are warranted because tumors might become visible after several months. 22
The present case illustrates primary FBS caused by nonspecific adenocarcinoma in the deep lobe of the parotid gland. After surgical treatment, the symptoms of primary FBS were completely relieved. Hence, we hold the opinion that primary FBS are mainly caused by diseases in the region of the inferior temporal fossa, the deep lobe of the parotid gland, and the parapharyngeal space, where malignant tumors are common. The pain associated with primary FBS can be relieved through tumor resection.
Conclusion
First bite syndrome is a postoperative complication. Primary FBS is a rare presenting symptom in the absence of surgery. First bite syndrome has an enormous impact on the quality of patients’ life. It is vitally important to identify the cause of pain in patients with primary FBS. Once the etiology is identified, the pain can often be alleviated through the surgical treatment.
Footnotes
Authors’ Note
Xia Yang and Xinjie Yang wrote the article. Weiqi Wang gathered the information, Pu Zhang gathered the information and summarize the article. Rui Hou and Yaowu Yang organized the materials and summarize the article. Delin Lei proofread the article. Jianhua Wei provide the case and proofread the article. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript. The authors declare that they have neither personal conflicts of interest nor institutional or financial prosperity in any drugs, materials, or devices described in this manuscript. The authors have no financial disclosures to report. In addition, all patients gave their informed consent for any medical and scientific investigations. This paper has not been published previously, is not under consideration for publication elsewhere and we acknowledge that, if accepted, this paper will not be published elsewhere in the same form, in English or in any other language, without the written consent of the publisher.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from National Natural Science Foundation of China (No. 81973114) and grants from National Clinical Research Center for Oral Diseases (grant no. LCA202001 and LCB202008) Shaanxi Key Research and Development program (No. 2018SF-163).