
Abstract
Actinomycosis is an infrequent infectious disease caused by Actinomyces species. Actinomycoses in the nasopharynx are extremely rare, especially in the Rosenmüller’s fossa. This report presents a case of actinomycosis in the Rosenmüller’s fossa. A 75-year-old woman presented with a 6-month history of bloody sputum. A grayish-white caseous tissue was found in the right Rosenmüller’s fossa after retracting the torus tubarius. Magnetic resonance imaging showed a well-defined lesion with low-signal intensity on T1- and T2-weighted images; small low-signal areas were interspersed inside. The lesion was removed under an endoscope. Histopathological examination revealed eosinophilic, club-shaped structures surrounding a hematoxylophilic center, leading to the diagnosis of actinomycosis. The symptoms improved after 3 months of amoxicillin administration but recurred quickly. After 6 months of amoxicillin administration, the bloody sputum disappeared, and local and imaging findings were normal.
Introduction
Actinomycosis is an infrequent infectious disease caused by Actinomyces species. Actinomyces are gram-positive anaerobic bacilli that are part of the normal flora in the oral cavity and oropharynx. Actinomycoses are opportunistic infections in most cases; foreign bodies or trauma can cause actinomycosis. Cervicofacial infection accounts for approximately 60% of all actinomycoses. 1 Actinomycosis developing in the soft tissues is a diagnostic challenge and can mimic malignant tumors. Studies on actinomycosis in the nasopharynx are extremely rare, and most reported cases occurred in the posterior wall.2-10 This report presents a case of actinomycosis in the Rosenmüller’s fossa.
Case Report
A 75-year-old woman was referred to Iwate Medical University with a 6-month history of bloody sputum. She consulted a clinic 5 months ago. On fiberscopic examination, necrotic tissue was found in the right Rosenmüller’s fossa. Histological examination was conducted; however, the results showed nonspecific reactive changes with erosions. The lesion persisted for months, and she was referred to our hospital.
The nasopharynx was thoroughly examined with a rigid endoscope. After retracting the torus tubarius, a grayish-white caseous tissue was found in the right Rosenmüller’s fossa. Magnetic resonance imaging (MRI) showed a well-defined lesion with low signal intensity (white arrowhead) on T1-weighted images. Small low-signal areas were interspersed within the lesion (Figure 1A). On T2-weighted images, the lesion showed low signal intensity surrounded by high-signal areas. All caseous tissues were removed under an endoscope. Histopathological examination revealed eosinophilic, club-shaped structures surrounding a hematoxylophilic center (Figure 2), leading to the diagnosis of actinomycosis.
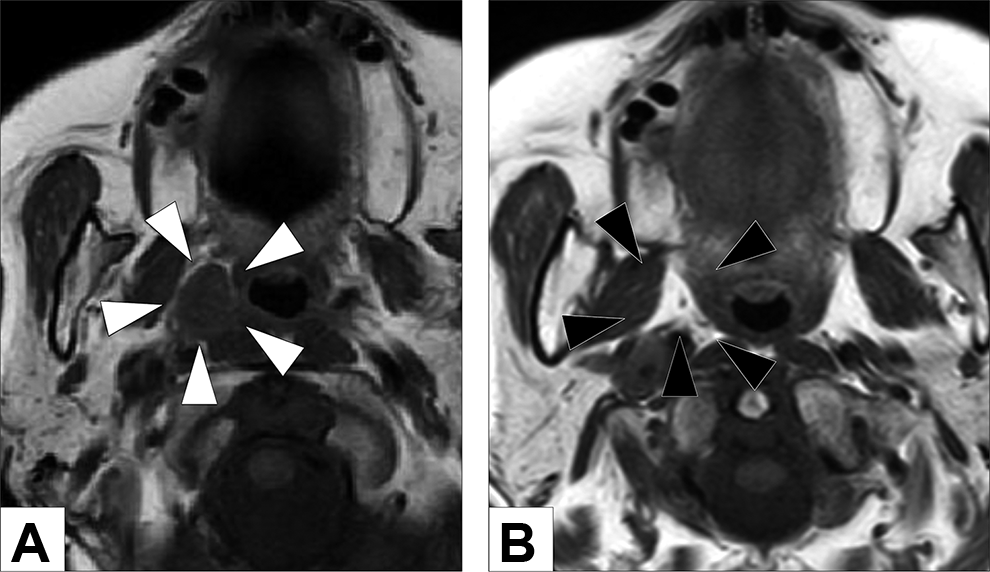
Axial T1-weighted images of the lesion before (A) and after (B) the treatment. The lesion was well-defined and showed low signal intensity on both T1-weighted images (white arrowhead). Small low-signal areas were interspersed within the lesion. On T2-weighted images, the lesion showed low signal intensity surrounded by high-signal areas. The lesion disappeared on T1-weighted images 6 months after the end of treatment (black arrowhead).
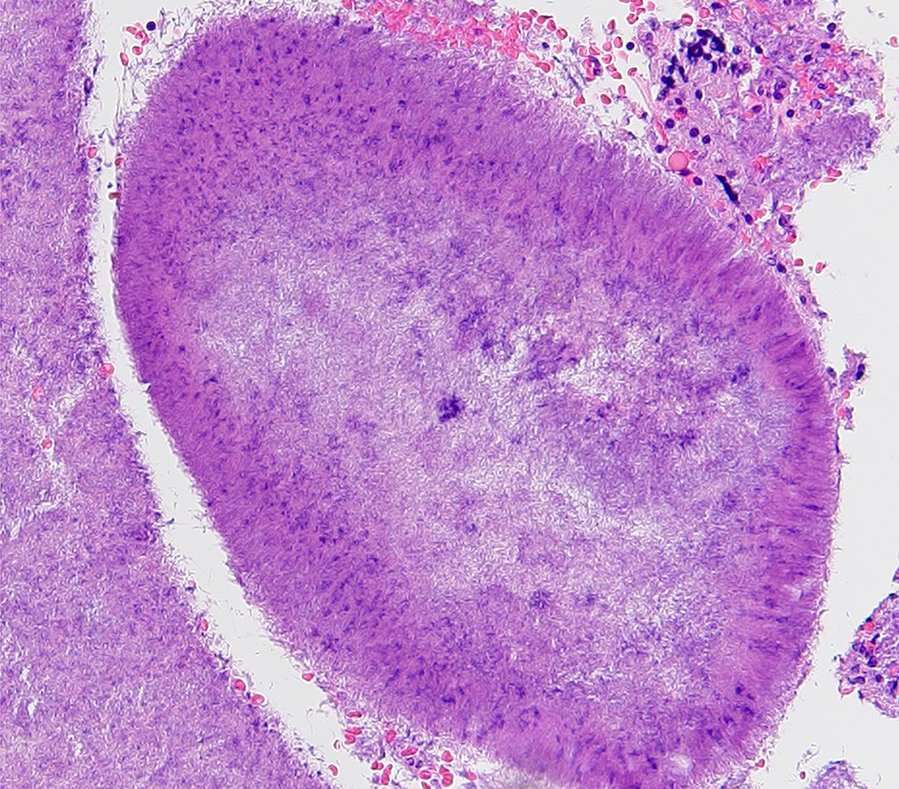
Histopathological examination showed oval hematoxylophilic masses with radiating fringes of eosinophilic club-shaped structures (original magnification, ×200; hematoxylin-eosin stain).
Systemic amoxicillin 750 mg/d was administered for 3 months. All symptoms disappeared, and the mucosa of the Rosenmüller’s fossa became normal. However, the bloody sputum and caseous tissue recurred in Rosenmüller’s fossa one month after the cessation of antibiotic therapy. After 6 months of amoxicillin administration, the bloody sputum and caseous tissue disappeared. Magnetic resonance imaging confirmed that the lesion resolved (Figure 1B). The patient was free from the disease for 6 months.
Discussion
Actinomycosis is a chronic infection caused by Actinomyces species. Actinomyces israelii, which contributes to the normal flora of the oral cavity and is not usually pathogenic, is the most frequent causative agent. 1 Actinomycosis is triggered by trauma or systemic immunodeficiency but can develop without these backgrounds.
The symptoms vary according to the site of infection. Actinomycosis lacks characteristic clinical findings, and the diagnosis is challenging, especially when it develops in noncutaneous soft tissue. Actinomycosis in the nasopharynx shows symptoms similar to nasopharyngeal cancer, including nasal obstruction, otitis media with effusion, otorrhea, headache, and epistaxis.5-7 Intracranial complications, such as brain abscess 2 and internal carotid artery obstruction, 4 can develop. The endoscopic findings also mimic those of nasopharyngeal cancer.3,5-9 In most cases, nasopharyngeal cancer was suspected before the diagnosis. The patient presented with bloody sputum with a caseous substance in Rosenmüller’s fossa. Endoscopic findings alone were insufficient to exclude fungal infection and neoplastic disease.
The diagnosis of actinomycosis can be made according to bacterial culture testing and histopathological examination. However, the detection rate in bacterial cultures is low. 1 This is partially because Actinomyces spp. are anaerobic or microaerophilic. Systemic antibiotics are often prescribed before diagnosis, which may reduce the identification rate. In Japan, up to 96% of cervicofacial actinomycoses were diagnosed by histopathological examination. 11 The diagnosis in the present case was also made based on histopathological examination results; moreover, the bacterial culture test failed to show Actinomyces. Histologically, actinomycosis shows chronic inflammation of granulomatous fibrous tissue, within which eosinophilic club-shaped structures are found surrounding a hematoxylinophilic center. Although it is difficult to diagnose actinomycosis on imaging alone, there are some characteristic findings. Popcorn-like dystrophic calcification within the lesion, which is caused by tissue necrosis and eventual dystrophic calcification, is reported in actinomycosis. 12 This finding is rare but may suggest actinomycosis.12,13 In the present case, MRI showed scattered low-signal areas within the mass, which corresponded to popcorn-like dystrophic calcification.
There is no established treatment policy for actinomycosis. Debridement is considered important, but surgical treatments alone have a high probability of recurrence and systemic antibiotics are needed. In most cases, the drug susceptibility test is impossible, and large doses of penicillin-based antimicrobial agents are used. The chronic form of actinomycosis shows strong fibrosis and poor blood flow within the lesion, resulting in poor tissue responses to antimicrobial agents. It has been argued that long-term administration is necessary. Traditionally, prolonged high doses of penicillin G or amoxicillin (6-12 months) are recommended, but short-term antibiotic therapy (3 months) can be justified, particularly for patients who underwent optimal debridement of infected tissues.1,14 In some cases, the symptoms disappear quickly after treatment, but relapse is common. In the present case, the disease recurred after 3 months of amoxicillin administration. The duration of administration should be determined by careful follow-up in combination with local and imaging findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.