
Abstract
Abdominal wall endometriosis refers to the presence of endometrial tissue within surgical scars, most commonly occurring following gynecological procedures such as cesarean sections. This case report presents a rare case of abdominal wall endometriosis in a cesarean scar. The patient, a 32-year-old woman with a history of two previous cesarean sections, presented with cyclic pain and swelling in the lower abdominal region. Physical examination revealed a tender, well-defined mass within the cesarean scar. Surgical excision of the mass was performed, and histopathological examination confirmed the presence of endometrial tissue. This case highlights the importance of considering abdominal wall endometriosis in the differential diagnosis of patients presenting with cyclic pain or swelling in previous surgical scars. Prompt diagnosis and appropriate management can help alleviate symptoms and prevent complications.
Keywords
Introduction
Abdominal wall endometriosis is a rare condition characterized by the presence of endometrial tissue within surgical scars. 1 It most commonly occurs following gynecological procedures, such as cesarean sections or hysterectomies.1,2 Abdominal wall endometriosis can present with cyclic pain and swelling, usually corresponding to the menstrual cycle. Early diagnosis and prompt management are crucial to alleviate symptoms and prevent potential complications. 3 This case report describes a rare case of abdominal wall endometriosis in a cesarean scar and emphasizes the significance of considering this condition in the differential diagnosis of patients presenting with similar symptoms.
Case presentation
A 32-year-old woman, para 2 living 2, presented to the gynecology clinic with complaints of cyclic pain and swelling in the lower abdominal region. She had a history of two previous cesarean sections, the most recent one being 2 years ago. The patient reported that the pain typically occurred a few days before her menstrual period and subsided afterward. The intensity of pain gradually increased over the past 6 months, prompting her to seek medical attention.
On physical examination, a tender, well-defined mass measuring approximately 2 cm in diameter was palpated within the lower segment cesarean scar. The mass was located superficially beneath the skin and demonstrated tenderness on deep palpation. No associated erythema or discharge was noted (Figure 1).

A picture of endometrial scar prior to excision.
Given the clinical suspicion of abdominal wall endometriosis, the patient was warranted for further evaluation. Ultrasonography of the scarred area revealed a heterogeneous mass with increased vascularity, suggestive of abdominal wall endometriosis. No evidence of associated herniation or other pathologies was noted.
Surgical excision of the mass was performed under general anesthesia. A 4 cm incision was made along the previous cesarean scar, and the mass was carefully dissected and removed, along with the involved scar tissue (Figure 2). Intraoperative frozen section examination revealed the presence of endometrial glands and stroma within the excised mass, confirming the diagnosis of abdominal wall endometriosis (Figure 3). The wound was closed in layers using absorbable sutures, and the excised mass was sent for histopathological examination.

A perioperative photograph showing endometriotic tissue was noted on the subcutaneous plane involving the outer layer of the rectus sheath.
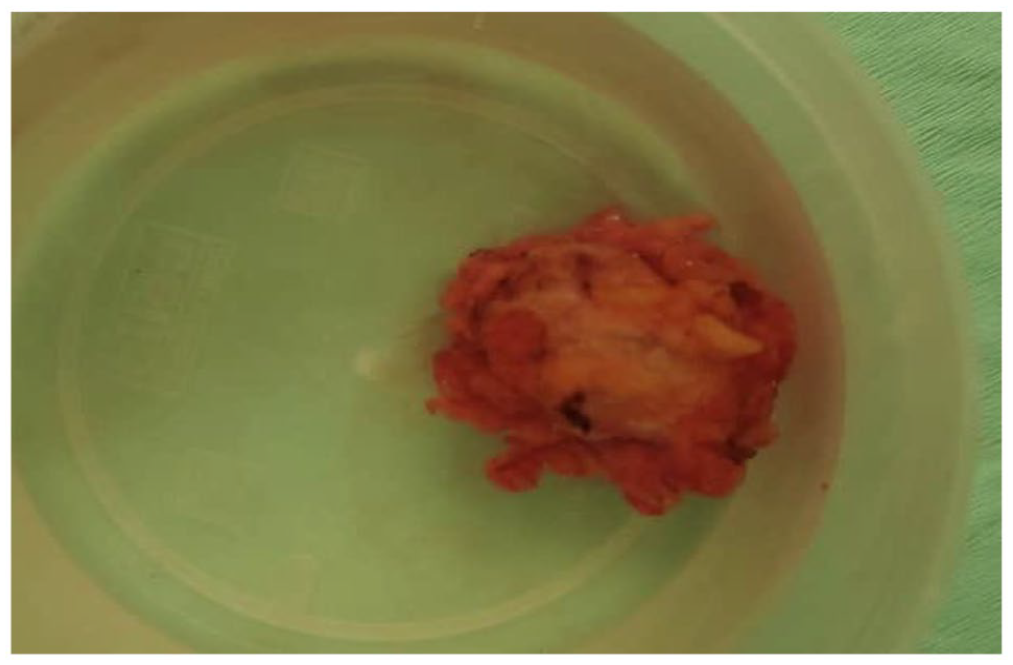
Photograph showing the resected specimen.
Histopathological examination confirmed the presence of endometrial glands and stroma within the excised mass, consistent with abdominal wall endometriosis (Figure 4). The patient’s postoperative course was uneventful, and her symptoms resolved after the surgery. Follow-up visits at regular intervals showed that the scar had completely healed.

Photograph showing a histopathologic slide of the resected specimen showing endometrial glands lined by benign endometrial cells.
Discussion
Abdominal wall endometriosis is a rare condition characterized by the presence of endometrial tissue within surgical scars. 1 The prevalence of abdominal wall endometriosis in cesarean scars is relatively low compared to other forms of endometriosis. 2 Exact prevalence rates are challenging to determine due to the rarity of the condition and potential underdiagnosis or misdiagnosis. 3 Abdominal wall endometriosis is estimated to occur in approximately 0.03%–1% of women who have undergone cesarean sections.1,2
While the exact pathophysiology of abdominal wall endometriosis remains unclear, several theories have been proposed to explain its development. The two most commonly suggested mechanisms are surgical implantation and retrograde menstruation. 4
Surgical implantation theory suggests that endometrial tissue may inadvertently implant within the surgical incision during gynecological procedures. This theory is supported by the observation that abdominal wall endometriosis often occurs at the site of previous surgical interventions. During surgery, endometrial cells may be unintentionally transported to the surgical site and subsequently develop into endometriotic lesions. The exact mechanism by which endometrial cells are implanted in the scar tissue is not fully understood and requires further research. 5
Retrograde menstruation theory proposes that endometrial cells flow backward through the fallopian tubes and reach the abdominal cavity during menstruation. These cells can then access the surgical scar through the patent tract created during the previous surgery. 6 Retrograde menstruation is a physiological process observed in many women, and it is considered a contributing factor to the development of endometriosis in various locations. In the context of abdominal wall endometriosis, retrograde menstruation provides a potential mechanism for the migration of endometrial cells to the surgical scar. 7
The diagnosis of abdominal wall endometriosis can be challenging, as its symptoms often overlap with other conditions such as incisional hernias or keloids.8,9 Cyclic pain and swelling in the scar area, typically associated with the menstrual cycle, are common presentations. Clinical suspicion, combined with imaging studies such as ultrasonography or magnetic resonance imaging, can aid in identifying the presence of a well-defined mass within the surgical scar, suggestive of abdominal wall endometriosis. 10 However, a definitive diagnosis requires a histopathological examination of the excised tissue.
Surgical excision is the primary treatment modality for abdominal wall endometriosis. Complete excision of the lesion, including the involved scar tissue, is crucial to minimize the risk of recurrence. It is essential to remove all endometriotic tissue, as residual cells can contribute to persistent symptoms and the potential for recurrence.11,12 The excised tissue should be sent for histopathological examination to confirm the diagnosis by demonstrating the presence of endometrial glands and stroma.
The commonly accepted treatment of choice for abdominal wall endometriosis is the total surgical excision of nodules. The pooled recurrence rate from previous reports is 4.5%. 13 Long-term follow-up is essential to monitor for recurrence or complications, although abdominal wall endometriosis has a low recurrence rate after complete excision. Recurrence typically presents with cyclic symptoms and can occur months to years after the initial surgery. 4
Conclusion
This case report highlights the occurrence of abdominal wall endometriosis in a cesarean scar, emphasizing the importance of considering this rare condition in the differential diagnosis of patients presenting with cyclic pain or swelling in previous surgical scars. Early diagnosis, surgical excision, and histopathological examination play crucial roles in the management of abdominal wall endometriosis. Awareness among clinicians and approprite interdisciplinary management can lead to successful outcomes, alleviating symptoms and preventing recurrence.
Footnotes
Acknowledgements
We would like to thank all the physicians, pathologists, and staff who have worked very hard to take care of this patient. Also, we would like to thank our patient for her allowing us to learn from her clinical presentation.
Author contributions
All authors contributed to the conceptualization, writing, and critical review of this case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.