
Abstract
Actinomycosis is a rare bacterial infection caused by Actinomyces, a group of Gram-positive anaerobic bacilli. These bacteria are a normal component of human flora; however, they can become pathogenic in susceptible hosts by entering through mucosal defects and disseminating submucosally to involve the surrounding tissue. Cervicofacial actinomycosis is the most common presentation; however, Actinomyces can rarely involve other aspects of the head and neck. Actinomycosis in this region is often mistaken for other disease processes, given its tendency to mimic other pathologies. We present a unique case of a 72-year-old male presenting with acute respiratory compromise due to submucosal actinomycosis of both the hypopharynx and the larynx requiring an emergent surgical airway. Many aspects of this patient’s presentation were highly suspicious of malignancy, including medical history, presenting symptoms, flexible laryngoscopy findings, CT results, and intraoperative appearance of the lesions. Actinomycosis should remain on the differential in patients with a submucosal laryngeal mass with clinical and radiographic evidence of extra laryngeal extension, especially in patients with a history of mucosal trauma, poor dentition, or an immunocompromised state. Multiple biopsies should be obtained, with definitive surgical treatment planning pending final pathology.
Introduction
Actinomycosis is a rare bacterial infection most commonly seen in the cervicofacial context with draining sinus tracts along the mandible. 1 Even more rare is its presentation in other areas of the head and neck. It has been referred to as “the great masquerader” given its ability to emulate other pathology. 2 Many practitioners find it difficult to diagnose and often not considered on the differential of a patient presenting with an obstructive submucosal laryngeal mass. We present a case of a gentleman with many cancerous risk factors presenting with acute airway compromise due to an obstructive laryngeal mass who was found have actinomycosis.
Case Report
The patient is a 72-year-old male with a medical history of type 2 diabetes, hypertension, and former tobacco and alcohol use disorders who presented to the emergency department with complaints of dysphagia and shortness of breath. The patient reported gradual worsening of this dysphagia in the last year and a half, with recent difficulty tolerating his secretions. Additionally, he reported new unintentional weight loss of 30 to 40 pounds, intermittent hemoptysis, and a raspy voice. The physical examination was notable for biphasic stridor, drooling, muffled voice, poor dentition, and palpable fullness along the right neck. Flexible laryngoscopy revealed a large submucosal mass filling the postcricoid space and obscuring the glottis with significant laryngeal edema (Figure 1). A contrast-enhanced CT of the neck revealed a 3.9 × 4.5 × 2 cm heterogeneously-enhancing soft tissue mass centered in the hypopharynx with severe supraglottic and glottic narrowing, effacement of paralaryngeal fat spaces, and erosion of the cricoid cartilage. There were several borderline level II to IV nodes bilaterally; however, none were enlarged by size criteria. The patient was taken emergently to the operating room for an awake tracheostomy. The tracheotomy was performed higher than normal due to the patient’s kyphosis, but otherwise was a standard awake tracheostomy with placement of a size 6 cuffed Shiley tracheostomy tube. Subsequent bronchoscopy revealed normal tracheal anatomy. The patient was stabilized, and on postoperative day 5, he underwent a direct laryngoscopy and biopsy with tracheostomy tube change. Intraoperatively, a large submucosal tumor with epicenter in the right postcricoid area and pyriform sinus with circumferential involvement of the posterior pharyngeal wall was visualized. Several biopsies were obtained and sent for permanent analysis. At that time, no specimens were sent for frozen pathology.
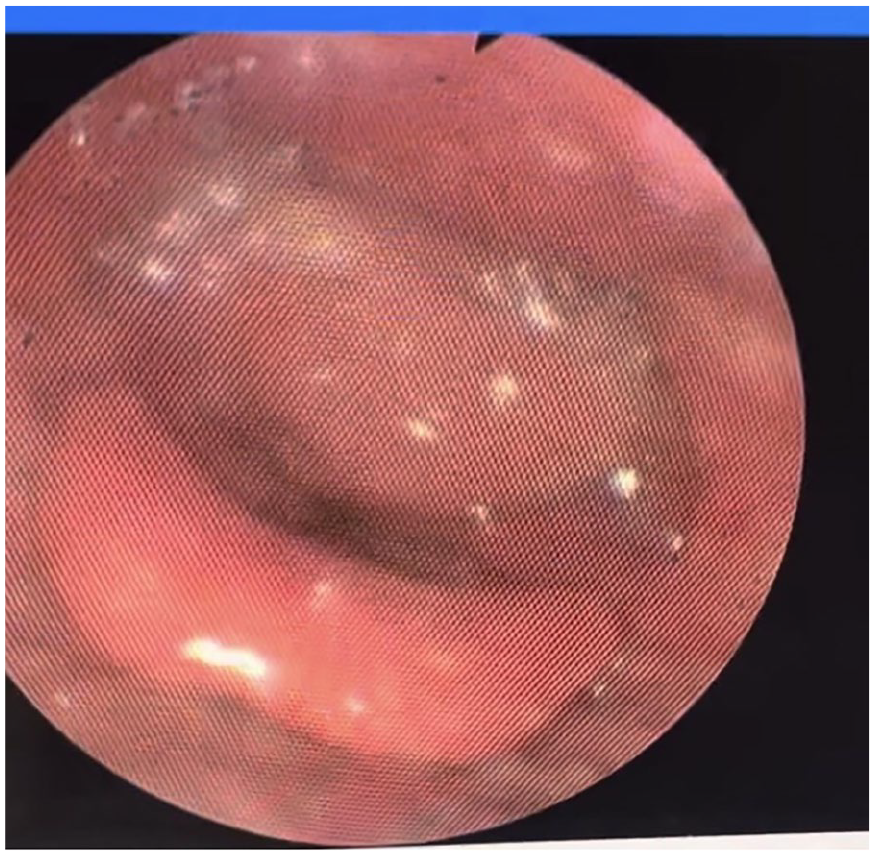
Flexible laryngoscopy on admission.
There was a high index of suspicion for malignancy, so he was counseled accordingly. He was taken back to the operating room with plans for total laryngectomy. Direct laryngoscopy with biopsy was repeated. Frozen results revealed acute and chronic inflammation, with no signs of malignancy. Bilateral selective neck dissection levels I to IV were then performed. Due to the presumptive nondiagnostic biopsy, a lateral pharyngotomy was performed to gain broad access. Multiple distinct lesions were identified, each with a large central ulceration, heaped mucosal edges, and submucosal extension. Many more specimens were obtained. Frozen section analysis revealed extensive inflammation and necrosis without atypical cells. At this point, the pharynx was repaired primarily and the case was aborted. Comprehensive infectious and immunologic workup was performed, all of which were negative, including QuantiFERON-TB Gold Plus testing. His history of a chronic productive cough and many years living outside of the United States promoted the inclusion of tuberculosis infection on our differential. The final pathology revealed necrotic connective tissue with acute and chronic inflammation, granulation tissue, and Actinomyces without signs of neoplasm (Figure 2). Infectious disease was consulted, and a prolonged course of penicillin therapy was recommended. Initially, he was treated broadly with ampicillin-sulbactam. After 6 weeks, he was discharged on 500 mg of amoxicillin-clavulanate three times daily for 6 to 12 months according to recommendations from the infectious disease team. There was near resolution of the lesions after approximately 1 month of treatment. The patient was decannulated 2 months after discharge.
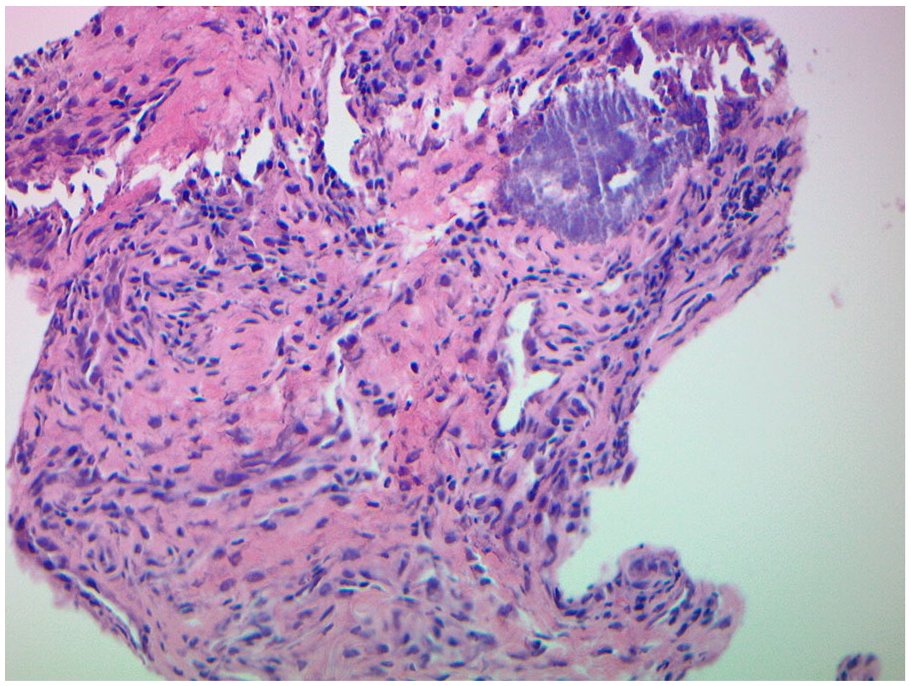
Photomicrograph of pathology revealing Actinomyces.
Discussion
Actinomycosis is a rare bacterial infection caused by Actinomyces, a Gram-positive anaerobic bacillus known to be a normal component of the human flora. Despite their filamentous structure resembling fungi, Actinomyces are true bacteria. 1 When pathogenic, Actinomyces is most commonly implicated in cervicofacial actinomycosis (50%-55%), followed by abdominopelvic (20%-25%) and thoracic (15%-20%) manifestations.3,4 Actinomycosis has been referred to as a “great masquerader,” particularly in the head and neck regions, given its tendency to emulate a multitude of pathologies.2,5 Destructive lesions and masses have also been reported involving the larynx, pharynx, temporal bone, thyroid, tonsils, paranasal sinuses, and the orbit.1,3 Bacteria enter through mucosal defects (often traumatic) and may disseminate submucosally to involve surrounding tissue. Risk factors include diabetes, poor dental hygiene, trauma, and immunosuppression.2,5,6
Actinomyces infections in the head and neck outside of the context of cervicofacial actinomycosis are most often isolated to the larynx (69%) or the pharynx (16%), with only 14% of cases involving both the larynx and the pharynx, as was the case for our patient. 7 Laryngeal actinomycosis can present with a variety of nonspecific symptoms including hoarseness, respiratory distress, stridor, and dysphagia, typically over the course of weeks to months. 6 Its presentation has even mimicked an airway foreign body.4,8,9 Rarely, it can present with acute respiratory compromise and may necessitate an emergent surgical airway although most patients can be decannulated within weeks after starting treatment.7,10
Flexible laryngoscopy often reveals a whitish or yellow exophytic or pedunculated mass exhibiting necrotic or ulcerative features within the hypopharynx or larynx, almost always with laryngeal edema.6,7 Notably, our patient’s laryngoscopy findings were incongruent with these traditional features; rather, a large submucosal mass was visualized. CT scans are similarly nonspecific and often demonstrate a soft tissue mass with adjacent infiltrative inflammatory changes, destruction of adjacent laryngeal cartilages, and effacement of adjacent fat planes, as observed in our patient’s CT scan.3,6
In the context of our patient, a 72-year-old male with a significant alcohol and smoking history with an exophytic submucosal laryngeal mass with hypopharyngeal extension presenting with respiratory distress requiring awake tracheostomy, along with CT findings demonstrative of a destructive heterogeneous mass, our team had a high index of suspicion of malignancy. This case emphasizes the importance of obtaining thorough biopsies early in the workup of submucosal glottic masses.
It is crucial to note that actinomycosis of the head and neck can also present in conjunction with malignancy. Studies have reported that up to 10% of patients with laryngeal actinomycosis may have concomitant malignancy (most often squamous cell carcinoma).5,7 Thus, while prompt penicillin-based therapy should be initiated, close follow-up with otolaryngology is recommended to ensure resolution of symptoms.
The standard of treatment for actinomycosis remains as initial intravenous and then prolonged oral penicillin-based therapy, the duration dependent on the clinical response.5,7 Actinomyces species are susceptible to β-lactam antibiotics, with doxycycline, clindamycin, and carbapenems serving as alternatives in cases of penicillin allergy or intolerance. 11 Following excisional biopsy, surgical intervention for head and neck actinomycosis has been indicated primarily in the context of complications of the disease, including airway compromise or abscess formation. Debridement may be necessary in the cases of osteomyelitis, recalcitrant fibrotic lesions, or concurrent malignancy.1,5
Conclusion
We present a unique case of Actinomycosis in the head and neck, presenting as a submucosal mass in the hypopharynx and larynx, with features mimicking primary laryngeal malignancy. Actinomyces should be considered in patients with submucosal laryngeal masses showing clinical and radiographic signs of extralaryngeal extension, particularly those with a history of mucosal trauma, poor dentition, or immunocompromised status. Multiple biopsies should be performed, with definitive surgical treatment pending final pathology.
Footnotes
Acknowledgements
We thank the patient mentioned in this study. We also thank Rush University Medical Center for their valuable help.
Author Contributions
J.M.: Writing—original draft, review, and editing; conceptualization; and visualization. R.R.: Writing—review and editing. A.S.: Writing—review and editing. K.S.: Conceptualization, writing—review and editing, and project administration.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient.
Consent for Publication
Informed consent for publication was provided by the participant.