
Abstract

The Gram-positive anaerobe Actinomyces spp. is a common bacteria found naturally in oral flora. Actinomycosis, the rare chronic disease caused by Actinomyces spp., commonly involves the perimandibular soft tissue and presents as a slowly progressive abscess. Laryngeal Actinomycosis has rarely been reported in the literature. While rare, we present a unique case of post-cricoid Actinomycosis in a pediatric patient. This case highlights a distinct occurrence, especially when history, symptoms, and imaging features are not specific.
Body
A 3-year-old female with speech delay, congenital torticollis, and recently diagnosed severe aplastic anemia on cyclosporine presented to the emergency department with fatigue, bloody stools, new petechia, and fevers. She was started on cefepime, voriconazole, and acyclovir, but with a negative infectious workup, those were discontinued. She was found to have persistent cytopenias and after complete infectious workup including negative blood, urine, stool, respiratory, and CSF studies, she did not have a clear infectious etiology. She was noted to have increased gamma-glutamyl transferase and bilirubin levels, which were determined to be possibly due to drug-induced (cyclosporine) toxicity. The otolaryngology service was initially involved due to oral ulcers resulting in decreased oral intake and pain. At that time, this was suggested to be possibly due to cyclosporine, but she did not have improvement upon discontinuation. An MRI of the neck was completed which showed mild mucosal enhancement, but no notable growth.
Despite a largely negative MRI, over the next three days, she had persistent odynophagia, lack of oral intake, and progressively worsening obstructive events during sleep which required treatment with continuous positive airway pressure; therefore, she was taken for a direct laryngoscopy with biopsy. This revealed a large fungating lesion filling the post-cricoid region with a furrow where the feeding tube was passing. Her epiglottis was normal; however, her arytenoids were bulbous, yellow in appearance, and ball valving into the airway (Figure 1). Otherwise, there was a normal laryngeal complex. The fungating lesion in the post-cricoid region was biopsied which showed granulomatous tissue with abundant plasma cells and areas of necrosis with evidence of filamentous organisms consistent with Actinomyces. She was taken back to the operating room for debulking of the lesion and esophagoscopy which was normal. She was started on penicillin G which was later deescalated to amoxicillin. For her aplastic anemia, she has been recommended to proceed with a bone marrow transplant; therefore, infectious disease recommended up to 6-12 months of treatment with amoxicillin. Direct laryngoscopy reveals a fungating mass in the post-cricoid region and large ball valving arytenoids.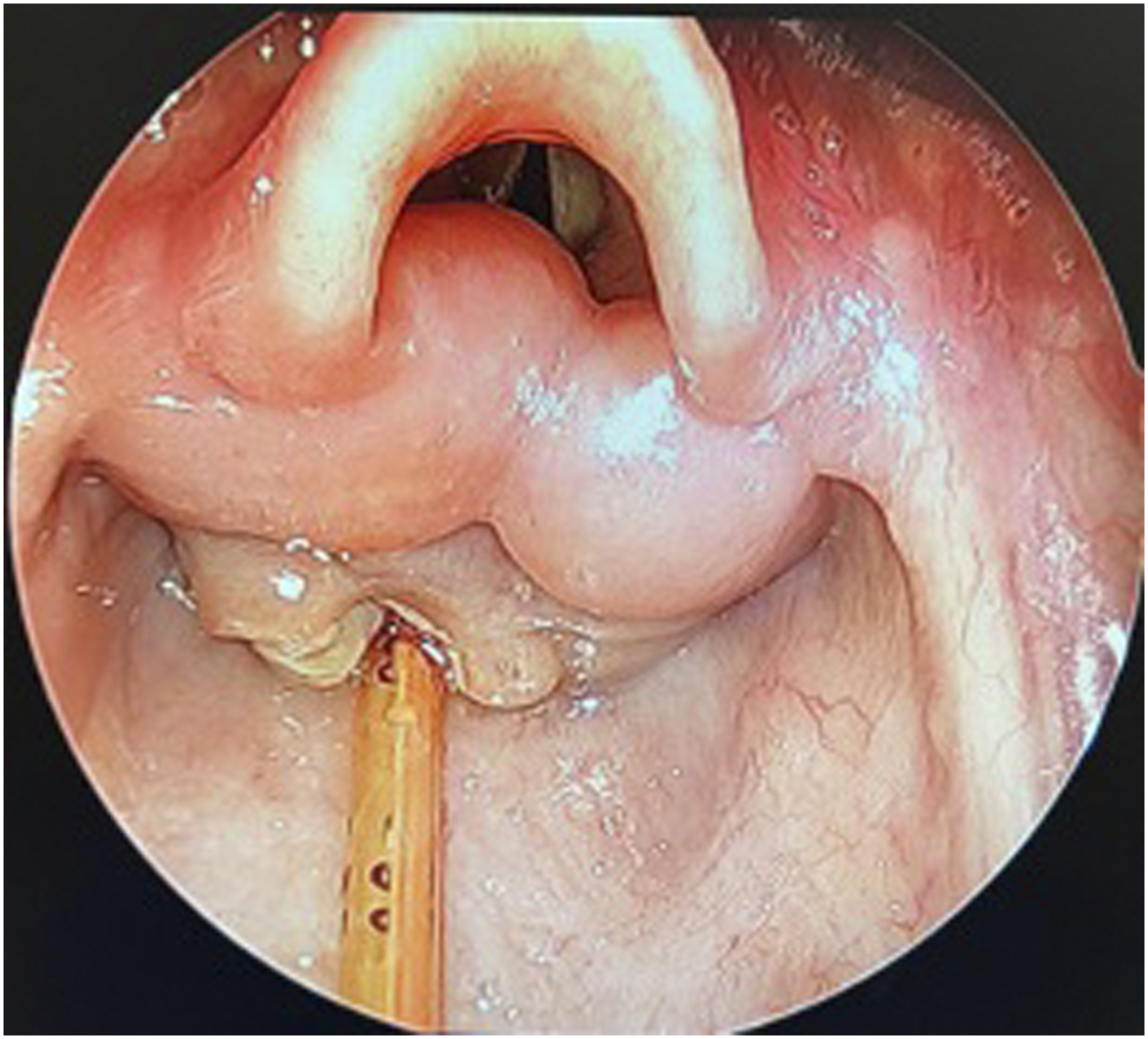
Six weeks after debulking and treatment, a direct laryngoscopy was completed which showed improvement with no granulation tissue in the post-cricoid region and significant improvement of the arytenoid edema (Figure 2). Symptomatically, she has improved from a pain standpoint and has been completely weaned off CPAP. After treatment, direct laryngoscopy revealing improvement in post-cricoid granulation and arytenoid edema.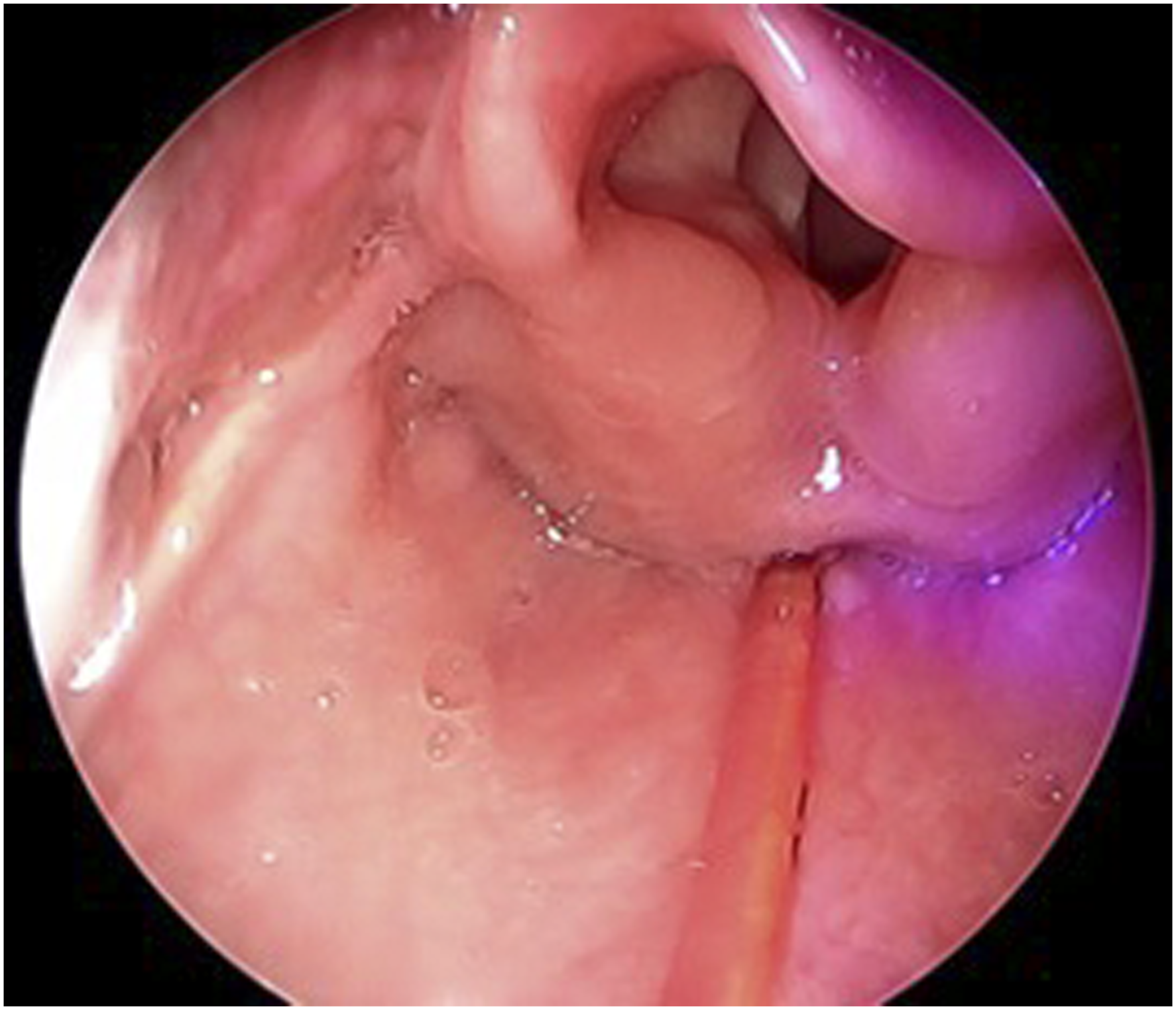
Actinomyces is an anaerobic, Gram-positive, filamentous, normal commensal bacteria of the oral flora. They are opportunistic pathogens that take advantage of trauma or injury to the mucosal barrier and can cause infection in both immunocompetent and immunocompromised hosts. Cervicofacial infections with Actinomyces have been documented, most commonly as an abscess over the mandible 1 . However, few reports exist in the literature of hypopharyngeal Actinomyces, specifically in the pediatric patient2-6. To our knowledge, this is the first reported case of pediatric laryngeal Actinomyces infection. Actinomyces can be difficult to diagnose and biopsy is the gold standard for diagnosis. Additionally, immunocompromised patients can present in a variety of ways further complicating the diagnosis. Previous case reports have had patients present with dysphagia, but it is not always present.2-7
Although rare, Actinomyces should be included on the differential for odynophagia unresolving with antibiotic and antifungal treatment, especially in the immunocompromised patient. Standard treatment includes long-term penicillin-based monotherapy; however, there has not been a standard treatment guideline developed 5 . Debulking appeared beneficial for our patient and a tracheostomy was avoided, although it has been documented in other case reports. Patients generally have full recovery with appropriate treatment and diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.