
Abstract
Colorectal cancer is the third most common cancer globally and nearly one fourth of distant metastases are found at the time of the primary diagnosis. Synchronous metastasis of colorectal cancer to the palatine tonsil is rare. To date, only 5 cases have been published in the English literature. In such cases, the prognosis is worse than in other common metastatic sites. Herein, we report a case of rectal adenocarcinoma who presented with a tonsillar mass initially.
Introduction
The most common malignancies of the palatine tonsil are squamous cell carcinomas which are strongly correlated with smoking, alcohol consumption, and Human Papillomavirus (HPV) infection. 1 Metastatic tumors of the tonsil are extremely rare, accounting for less than 1% of all tonsillar cancers, and most of them emerge from the skin, kidney, lung, stomach, and breast.2-7 To date, only 5 colorectal cancers (CRCs) with palatine tonsil synchronous metastasis have been documented in the English literature.8-12 Herein, we report the discovery of a very particular case of rectal adenocarcinoma recognized by diagnosis of a palatine tonsil mass.
Case Report
A 65-year-old male presented a lump sensation in the throat for more than 2 months. He had been a smoker for over fifty years. A 1 × 1 cm fungating mass over the upper pole of the right palatine tonsil was found (Figure 1). There were no palpable cervical lymph nodes. The rest of the physical examination was unremarkable. Punch biopsy disclosed adenocarcinoma, moderately differentiated, of the intestinal type (Figure 2). The patient experienced no gastrointestinal symptoms. A colonoscopy examination revealed a tumor at 4 cm from the anal verge and histopathology identified it as a moderately differentiated adenocarcinoma. Abdominal ultrasound and whole body bone scan were inconclusive to demonstrate metastatic disease. However, chest computed tomography scan disclosed nodular lesions at the right upper lung and mediastinum lymph nodes. The pretreatment carcinoembryonic antigen (CEA) level was within the normal limit. Wide excision of oropharyngeal tumor and open low anterior resection for rectal cancer were performed concomitantly. Eventually, a thoracoscopic resection was conducted and the lung and mediastinum lesions were proven to be metastatic mucinous adenocarcinoma originating from the colorectal tract. The final pathological diagnosis was rectal adenocarcinoma, pT3N2aM1b, stage IVB based on the American Joint Committee on Cancer TNM staging system, eighth edition. The patient received adjuvant chemotherapy with bevacizumab and fluorouracil and irinotecan after surgical interventions. Four months after diagnosis, the patient died due to chronic obstructive pulmonary disease with acute exacerbation.
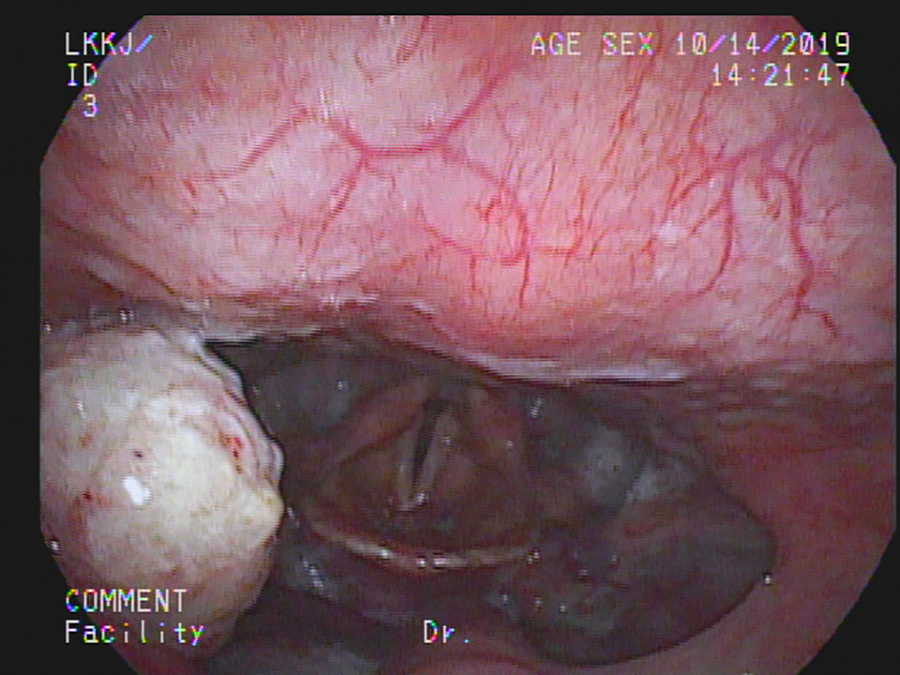
Image of the fungating mass on the right palatine tonsil.
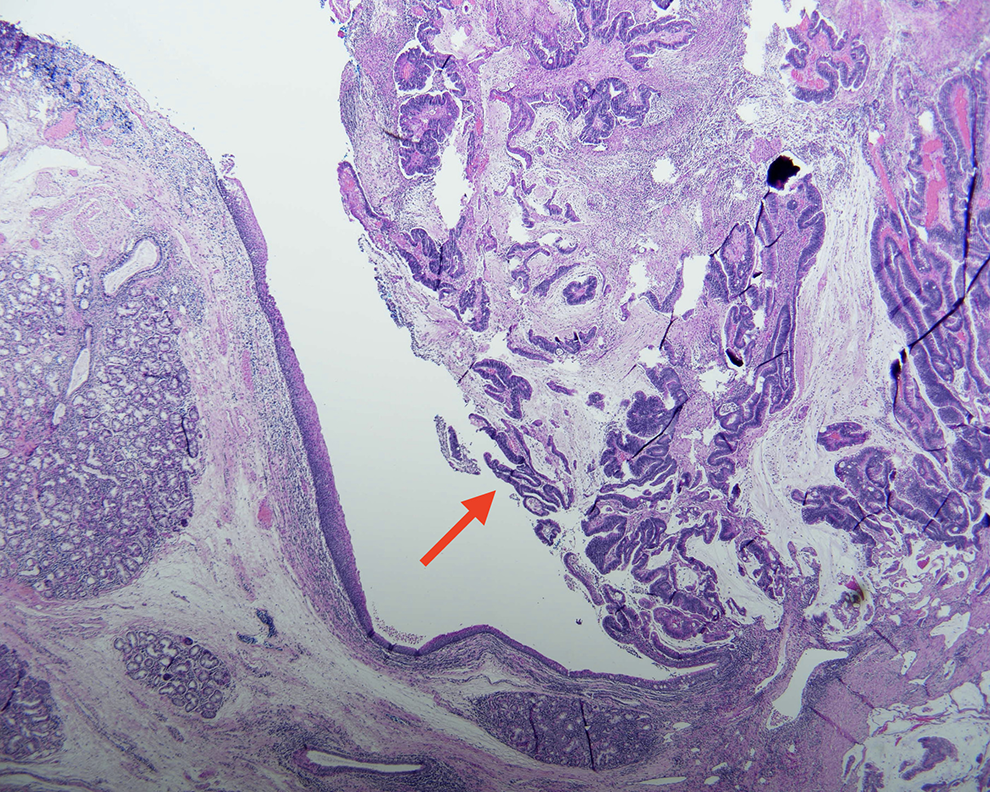
Histopathological examination of the resected tonsillar specimen. The arrow indicates a bulging mass of metastatic tumor with moderately differentiated glands composed of atypical columnar cells with extracellular mucin pooling, which is morphologically consistent with colorectal adenocarcinoma. Stromal invasion with desmoplastic change can also be seen.
Discussion
Colorectal cancer is the third most common cancer globally. Approximately 22% of patients with CRC will have distant metastases at the time of primary diagnosis.13,14 The most common distant metastatic site is the liver, followed by the peritoneum, lung, bone, and brain. Once distant metastasis occurs, the prognosis is dismal. The median survival varies from 4.4 to 24.1 months, depending on the site and numbers of metastases. 13
Colorectal cancer with palatine tonsil synchronous metastasis is an extremely rare event. This is the sixth reported case in the English literature (Table 1). The ages of these cases range from 44 to 81 years with a median age of 57.5 years, and the male to female ratio is 4:2. The most common primary site is the rectum. Furthermore, there is a high propensity of coexisting metastasis to other sites in these patients. The present case is atypical for the following 4 characteristics: first, the histopathology of the primary CRC; second, the side of tonsil affected; third, the sparing of neck lymph node involvement; and the final fourth, the pretreatment serum CEA level.
Characteristics of Patients With Tonsillar Synchronous Metastasis From CRC.
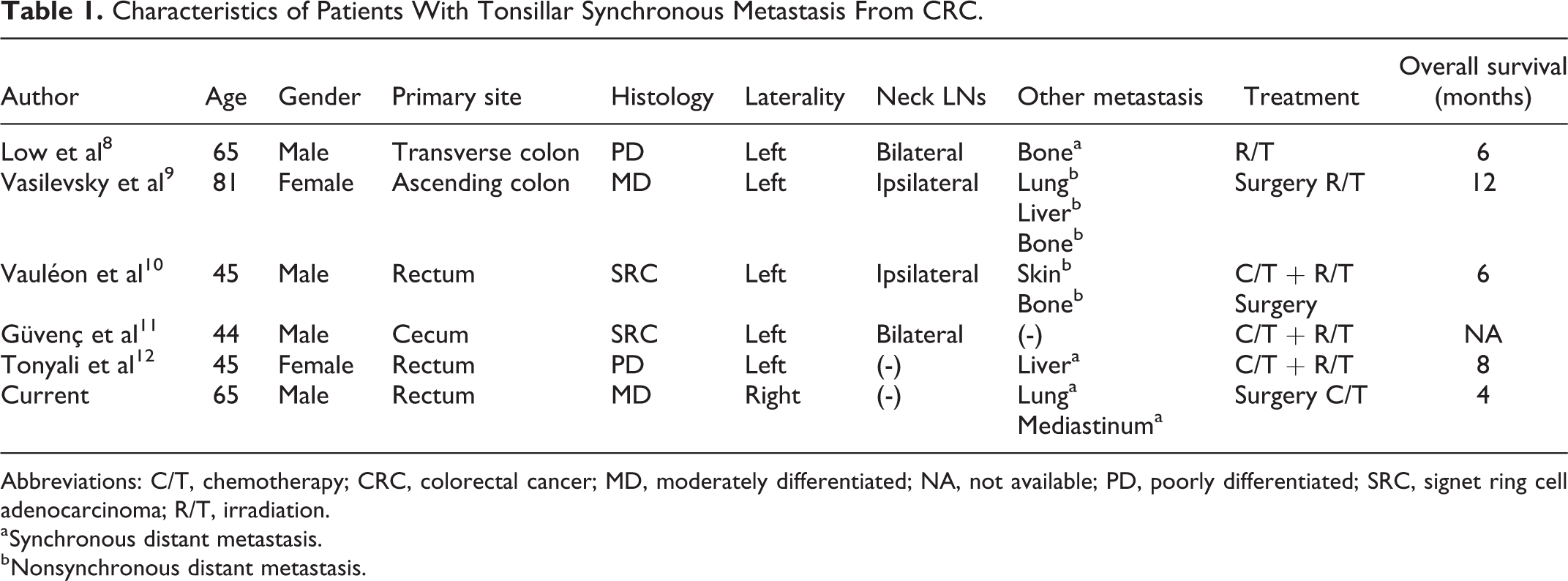
Abbreviations: C/T, chemotherapy; CRC, colorectal cancer; MD, moderately differentiated; NA, not available; PD, poorly differentiated; SRC, signet ring cell adenocarcinoma; R/T, irradiation.
a Synchronous distant metastasis.
b Nonsynchronous distant metastasis.
Poorly differentiated or signet ring cell adenocarcinomas are the major histology findings when tonsil metastasis develops from primary carcinoma of the gastrointestinal tract. 10 Metastatic palatine tonsil cancer is often unilateral with a preference for the left side. 4 None of the theories of metastatic spread can explain this finding. Once the tonsillar cancers are diagnosed, around 70% of patients present with metastasis to the cervical lymph nodes. 1 It seems that the same phenomena occur when the tonsil is invaded by CRC simultaneously.
The mechanisms of metastasis to the tonsil are controversial. Direct hematogenous spread is the most likely explanation. The route of spread is possibly via the portal vein and systemic arterial circulation to the tonsil. 4 Metastasis occurring in a cascading fashion cancer from already present in the liver and lungs has been postulated by Passmore et al. 5 It is reasonable to speculate that the 2 modes of spread may have been responsible for the metastasis found in our case. In addition, retrograde lymphatic tumor permeation or embolization is less common since the tonsil contains only efferent lymphatics. The possibility of tumor implantation from instrumentation or regurgitation (5) is not relevant in the present case.
High pretreatment serum CEA levels are associated with advanced tumor stage, elevated incidence of recurrence, and decreased survival. 14 The serum CEA level of our patient was not remarkable, but nevertheless, the survival time was dismal. Metastatic tonsillar cancers seem to carry a poor prognosis regardless of the primary tumor and the type of treatment. 7 The overall survival time of the 6 patients reported in the literature was between 4 and 12 months, which is compatible with tonsillar metastases from other malignancies.3-7 A rational explanation may be the presence of synchronous or rapid onset of further metastatic disease in other foci.
In conclusion, synchronous metastatic palatine tonsil tumor from CRC rarely occurs and has a dismal prognosis. Additionally, the cervical lymphadenopathy and the high CEA level may not be significant in these cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.