
Abstract
Objective:
Hyoid bone metastasis from lung adenocarcinoma is exceedingly rare. This study aims to provide an experience to clinicians in the differential diagnosis of hyoid tumors and discusses its possible source.
Methods and Results:
We report a 68-year-old male patient having hyoid bone metastasis from lung adenocarcinoma. The initial symptom of the hyoid bone metastasis was neck pain exacerbated by swallowing. The hyoid bone mass was resected based on comprehensive analysis including whole-body bone imaging and pathologic analysis of the hyoid bone mass. The adenocarcinoma of hyoid was identified as a metastatic lesion of lung adenocarcinoma. The patient recovered well and the anterior cervical pain was significantly alleviated after surgery and the patient underwent corresponding chemotherapy.
Conclusion:
In patients with hyoid metastasis of lung adenocarcinoma, surgical resection may reduce the pain in anterior cervical after full consideration of physical condition.
Background
Secondary tumors in hyoid bone are rare in clinics. Only a few studies have reported the cases of hyoid bone metastasis from distal primary malignant tumors, such as breast cancer, renal cell carcinoma, hepatocellular carcinoma, and sigmoid adenocarcinoma. 1 -4 Although bone metastasis from lung adenocarcinoma has been reported in detail, 5 this study reports for the first time bone metastasis from lung adenocarcinoma. A 68-year-old male patient, having hyoid bone metastasis from lung adenocarcinoma with the only symptom of neck pain exacerbated by swallowing, underwent hyoid mass resection surgery after thorough examination and assessment of his physical status. This study analyzed the clinical differential diagnosis of hyoid bone mass and the possible pathways of hyoid bone metastasis from lung adenocarcinoma.
Case Presentation
A 68-year-old man with a long history of smoking and drinking was admitted to our hospital in July 2019, complaining of neck pain exacerbated by swallowing for 6 months. The patient’s vital signs were as follows: temperature 36.7°C; respiratory rate: 17 breaths per minute; pulse 80 bpm; blood pressure 135/77 mm Hg. Blood counts, kidney function, and liver function were in the normal ranges.
Physical examination revealed a palpable solid mass with an unclear boundary in the middle of the anterior neck, which was found to move while swallowing. The surface of the skin appeared tensed like and tenderness was obvious when swallowing. Contrast-enhanced computed tomography (CT) showed a semicircular soft tissue mass shadow of 4.5 × 2.5 cm2 in size in the anterior lower part of the epiglottic cartilage, and it was more obvious when contrast was enhanced (Figure 1A and B). Lung CT showed a soft tissue mass shadow in the lower lobe of the right lung. The edges were rough and burrs were visible, and a necrotic area could be seen inside the burrs (Figure 2A and B).
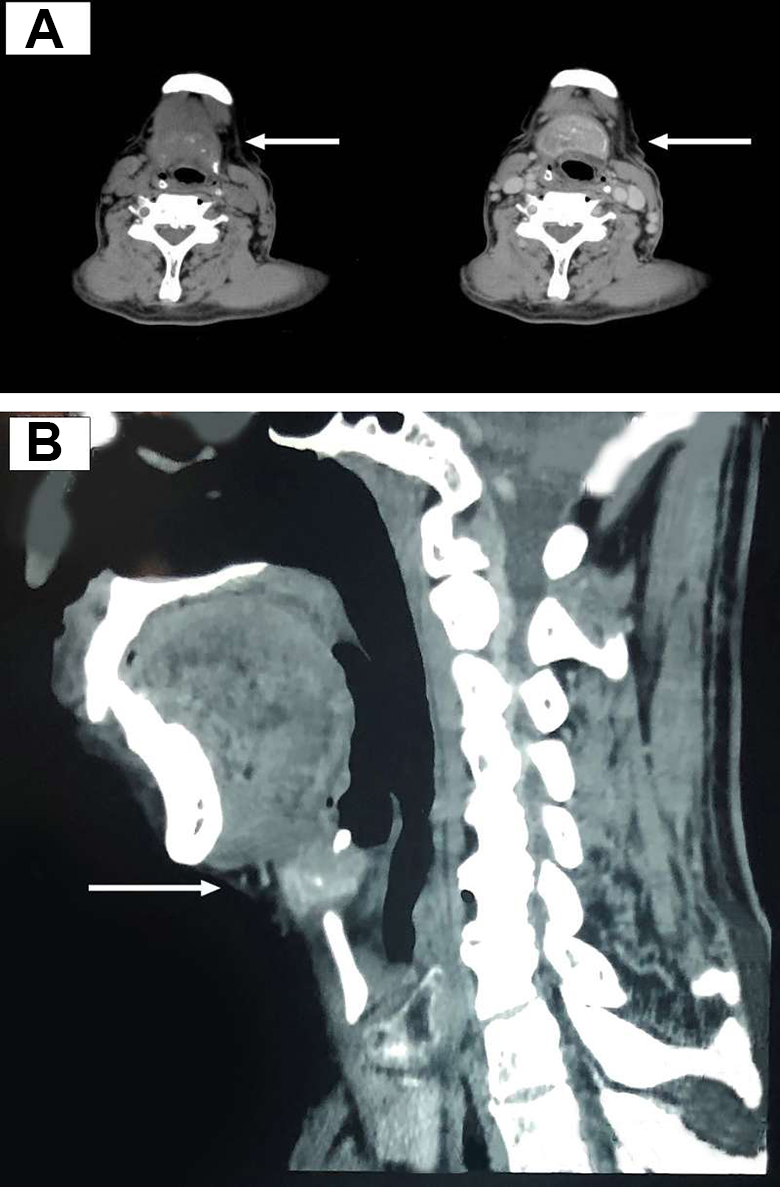
A and B, Neck contrast-enhanced computed tomography: showing the semicircular soft tissue mass shadow in the anterior and lower parts of the epiglottis cartilage and the osteolysis of the hyoid bone (arrows).
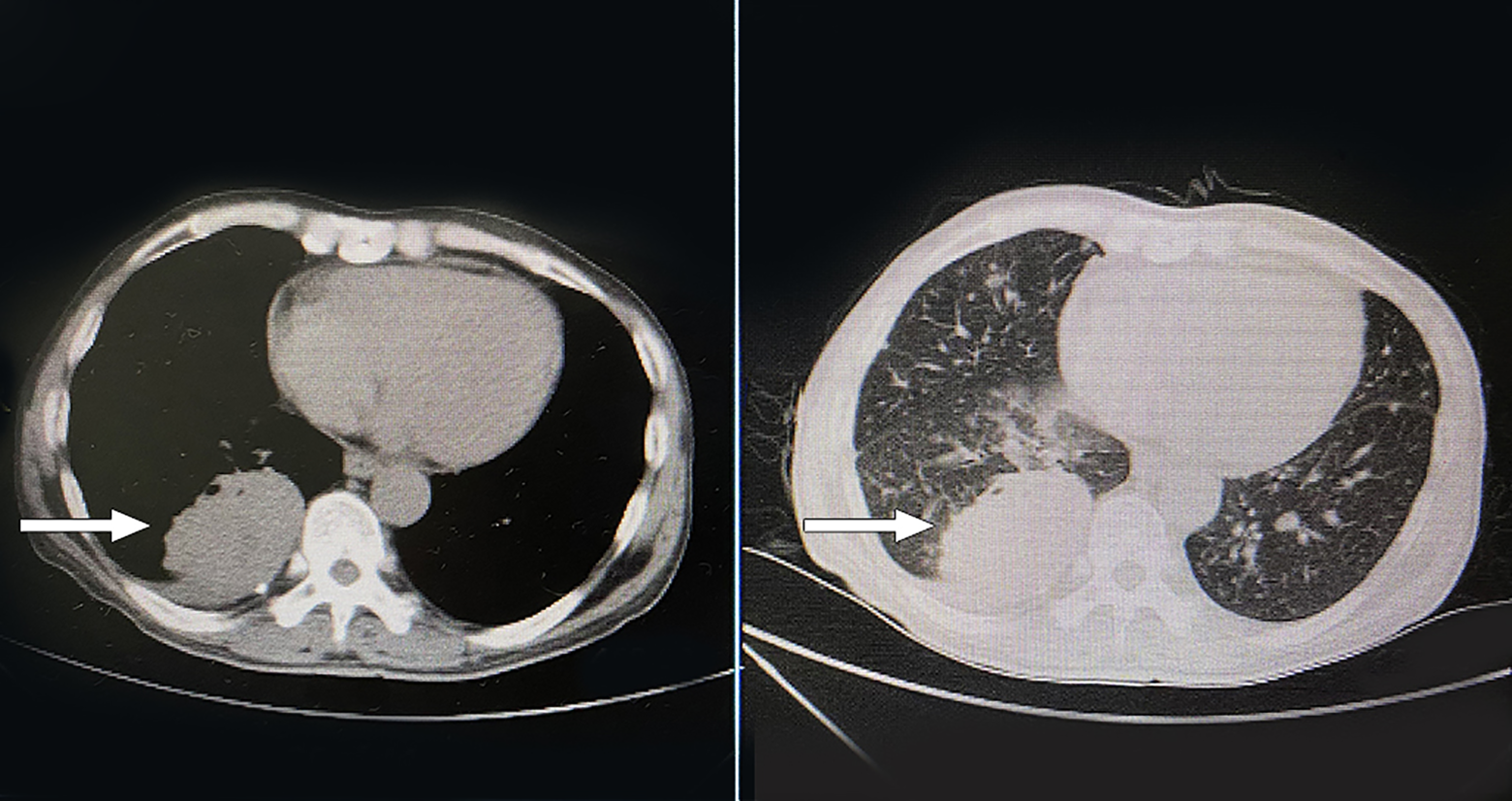
Lung computed tomography: showing a soft tissue mass shadow in the lower lobe of the right lung with a rough edge and burr formation, and a necrotic region was visible in both the mediastinal and lung windows (arrows).
In view of the uncertain nature of the lung mass, we performed a lung biopsy and the result was adenocarcinoma. The combined detection of multiple gene mutations in human lung cancer showed the epidermal growth factor receptor exon 20 insertion mutation. Bone scintigraphy suggested multiple shadows of bone metabolism in the whole body, which were likely to be malignant bone metastasis (Figure 3).
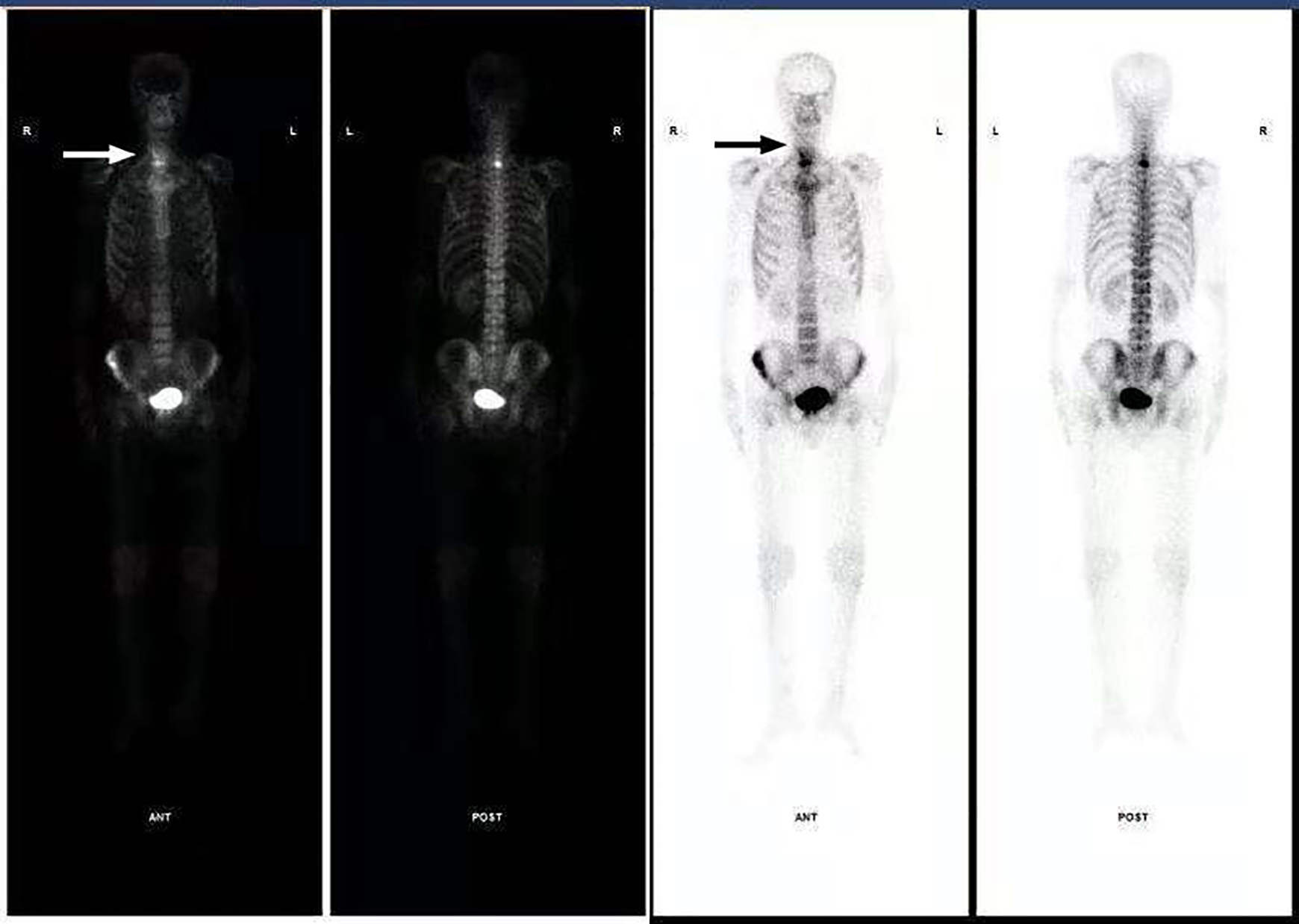
Bone scintigraphy imaging: shows tc-99 m accumulating in the front of the neck (arrows).
Since hyoid metastasis from lung adenocarcinoma is rare, and osteosarcoma and myeloma, which can cause osteolytic lesions, require pathological diagnosis, the patient underwent a neck mass resection surgery under general anesthesia after pathological diagnosis. The resection was also needed to assess the cause of pain while swallowing. A mass of about 4.5 × 2.5 cm2 in size was completely resected and the middle segment of hyoid bone disappeared after surgery. The results of intraoperative pathological detection were adenocarcinoma originating from the lung. The patient recovered well and the anterior cervical pain was significantly alleviated post-surgery and the patient underwent corresponding chemotherapy.
Discussion
Lung cancer is one of the most common malignant tumors in the world. Although this disease usually spreads to the liver and brain through the blood or lymph circulation, 6 bone metastases are also very common. 5 A previous study reported 74 lung adenocarcinoma patients with bone metastasis among 168 lung cancer patients with metastasis, the metastatic sites were spine, ribs, and pelvis. 7 Lung adenocarcinoma is a type of lung cancer that is prone to bone metastasis; for instance, bone metastases have been reported in 45% of the lung adenocarcinoma patients in a previously published article. 8 Considering that the patient’s lung CT showed definite lumps, we performed lung biopsy and combined the detection of multiple gene mutations involved in human lung cancer, as well as whole-body bone imaging, and finally confirmed the diagnosis of lung adenocarcinoma.
Regarding the mass of hyoid bone at the anterior portion of the neck, common thyroglossal duct cyst in children often occurs in clinics, whereas the mass of hyoid bone in adults is rare. However, some thyroglossal duct cysts with atypical symptoms can still be found in adults. 9 In addition, some rare hyoid masses transferred from distant primary tumors have been reported, such as hyoid bone metastases from breast cancer, renal cell carcinoma, hepatocellular carcinoma, and colon cancer. 1 -4 However, considering that hyoid metastases from lung adenocarcinoma are rare and have not been reported, it is reasonable to suspect that there is no clear relationship between hyoid masses and lung adenocarcinoma.
Considering that osteosarcoma and myeloma, which can cause osteolytic lesions, also require pathological diagnosis and surgical intervention, 10,11 and in many circumstances, the life quality of patients will be significantly affected if the patients do not receive surgical intervention for bone metastases of lung cancer, 12 we performed the mass resection surgery based on comprehensive assessment according to Expert Consensus on Diagnosis and Treatment of Bone Metastasis from Lung Cancer (version 2019): the patient could live for more than 3 months in good condition; the patient was able to tolerate surgical trauma and anesthesia; the patient was expected to have a better life quality after surgery than before. During the operation, we removed the tumor completely and identified the hyoid mass as a metastatic lesion of lung adenocarcinoma.
Among all lung cancers with bone metastases, the incidence of adenocarcinoma is much higher than that of squamous carcinoma. The reason may be that lung adenocarcinoma often occurs in mucous glands and goblet cells surrounding the lung tissue and is prone to vascular invasion and distant metastasis. Lung adenocarcinoma is most likely to metastasize to the hyoid through the circulatory system, and the most likely route is the branch of the superior laryngeal artery. 13 While the lingual artery supplies blood to the hyoid bone, metastasis may occur through these vessels.
Many other studies have also reported cases of hyoid mass metastases from distant malignant tumors. Lung adenocarcinoma, as a pathological type that is prone to bone metastasis, should be paid more attention to. Whole-body bone scintigraphy is of great significance in the surgical intervention of hyoid bone metastasis from lung adenocarcinoma. In our case, the anterior cervical pain was significantly alleviated after resection of the hyoid mass.
Conclusion
Hyoid bone metastases can also occur in lung adenocarcinoma. Resection of hyoid mass is recommended after the overall consideration of the patient’s physical status and the improvement of life quality after surgery. Superior laryngeal artery and the branch of the lingual artery may be the pathways mediating the hyoid bone metastasis from lung adenocarcinoma.
Footnotes
Authors’ Note
This is the first submission on this topic and this research has not been presented at a scientific meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Department of Science and Technology of Liaoning Province (No. 201602881).