
Abstract
Neoplasms in the infratemporal fossa (ITF) are rare and insidious lesions that cause various symptoms due to involvement of the temporomandibular joint (TMJ), paranasal sinuses, and orbit. Here, we report a case of metastatic non-small cell lung adenocarcinoma in the ITF. The patient presented with facial pain and limited mouth opening, which did not respond to treatment for TMJ disorder, and a neoplasm was discovered in the ITF through medical imaging. With an open biopsy, the diagnosis was finalized. This report suggested that the physician should consider lesions in the ITF when facial pain and limited mouth opening failed local treatment, and distant metastasis of malignant tumor should be alerted. We also reviewed the literature regarding metastatic cancer to the ITF.
Introduction
The infratemporal fossa (ITF) is a complex and deep anatomical space behind the zygomatic bone and maxillary tuberosity, resulting in insidious onset and late presentation of diseases in this area. Neoplasms in ITF are heterogeneous in pathologies, more often arise from neighboring structures such as the parotid gland, paranasal sinuses, and middle cranial fossa, less often onset primarily, and rarely spread from distant sites. 1
Lung cancer is the leading cause of cancer-related death worldwide. 2 The major subtype of lung cancer is non-small cell lung cancer (NSCLC), including lung adenocarcinoma (LUAD) and lung squamous cell carcinoma (LUSC). 3 Lung cancer in nonsmokers often presented as LUAD in histology, 4 and is more common in east Asia, which was considered associated with environmental, occupational, and genetic exposures. The most frequent metastatic sites of lung cancer were the nervous system, bone, liver, respiratory system, and adrenal gland, which vary between histopathological types, 1 metastasis to the head and neck region is rare.
We present a case of ITF mass in a 50-year-old man with a history of NSCLC. Positron emission tomography and computed tomography (PET-CT) was performed before surgery, suggesting the malignant nature of the mass, after which an open biopsy was performed. Histopathological examination and immunohistochemical staining confirmed the diagnosis of metastatic LUAD. Treatments for benign and malignant tumors are extremely different. To facilitate the most appropriate therapy, an accurate diagnosis is critical.
Case description
A 50-year-old man with a history of non-small cell LUAD presented with pain around the temples with restricted mouth opening for 4 months. He had been successively treated as periodontitis, temporomandibular joint (TMJ) disorder, and trigeminal neuralgia before a definitive diagnosis was made. A growing mass was found in the temple region, along with numbness over upper arch teeth, upper lip, nasal dorsum, and cheek in the left side.
The patient was diagnosed with non-small cell LUAD of the right lower lobe 4 years ago. He then received neoadjuvent targeting therapy with Gefitinib 250 mg for 6 months, reducing tumor size from 3 cm to 0.6 cm × 0.8 cm × 1.1 cm. Surgery was then performed to remove the residual tumor, and postoperative pathology revealed non-small cell adenocarcinoma of the right lower lobe. Gefitinib was resumed the 4th day after surgery, although several doses were missed due to severe pain during these months. He had a regular follow-up every year after surgery and his visit 5 years after surgery revealed a suspicious left supraclavicular lymph node.
On physical examination, a 3 cm tender mass was observed on the left side of the temporal region, which was hard and fixated, with a palpable left supraclavicular lymph node.
Computed tomography (CT) demonstrated abnormal soft tissue density in the left ITF area, and bone destruction in the lateral wall of the orbital cavity, the lateral wall of the maxillary sinus and the great wing of the sphenoid bone. On magnetic resonance imaging (MRI), the mass appeared isointense on T1- weighted imaging, hyperintense inside the lesion on T2-weighted imaging, and inhomogeneous enhancement on contrast-enhanced imaging. Meanwhile, the temporal lobe, lateral rectus and temporalis muscle were compressed and the temporalis, medial and lateral pterygoid muscle were swollen (Figure 1).
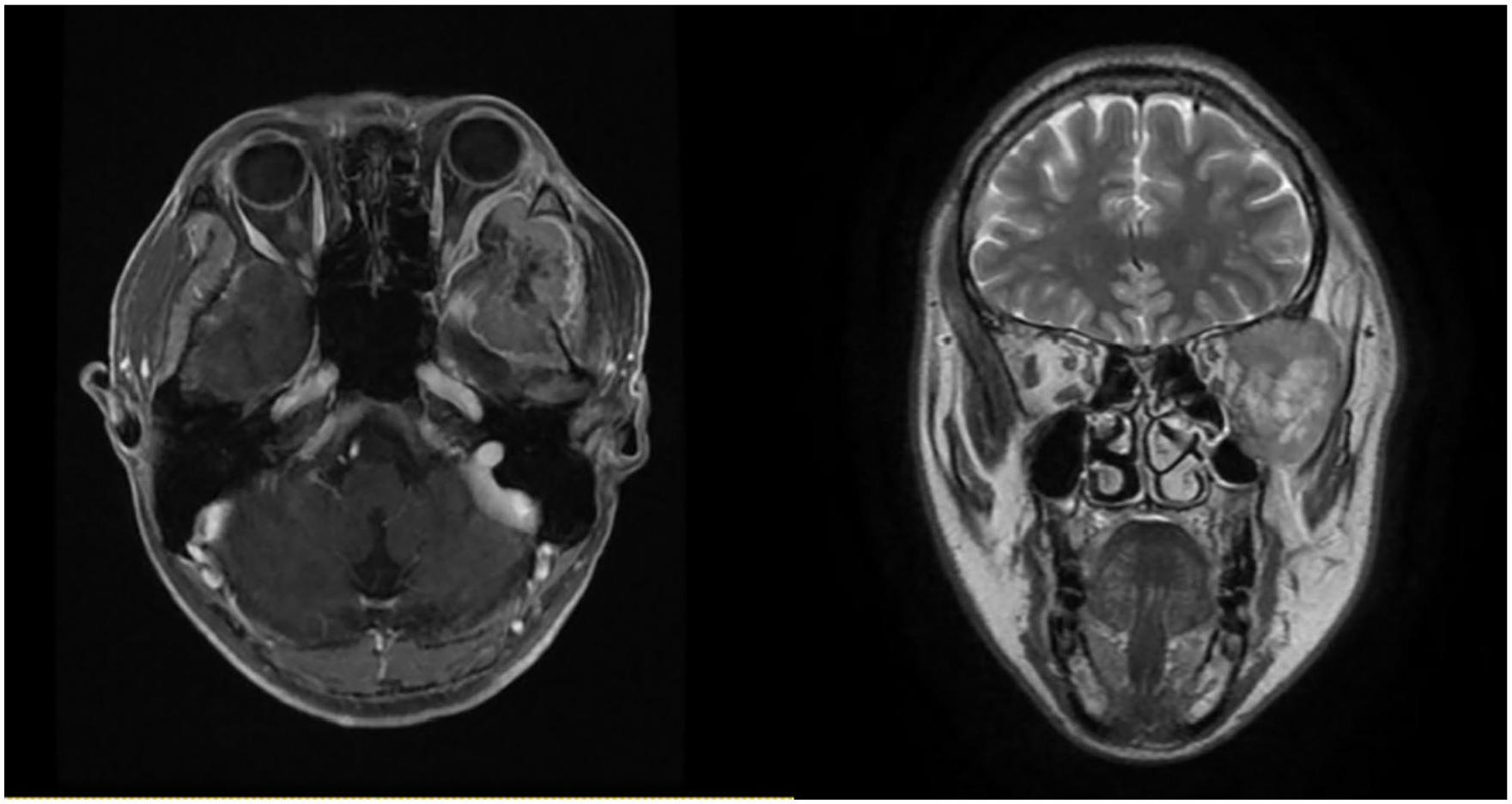
Post-contrast axial and coronal T1-weighted magnetic resonance image.
Given his past history of malignant tumor, cervical lymph node enlargement on physical examination, and bone destruction of CT imaging, PET-CT scan was performed to rule out malignancies or distant metastasis, though demonstrated excessive accumulation of radioactive isotopes at the left temporal region (SUVmax 7.6), on the right of the atlas (SUVmax 5.0) and of a ground glass nodule in the left upper lobe of the lung (SUVmax 0.7). A comprehensive preoperative examination was performed to exclude surgical contraindications. Then an incisional biopsy was performed and the neoplasm was observed at the attachment site of the temporal muscle swelling, where fast frozen pathology revealed adenocarcinoma tissue. Immunohistochemical staining showed that the sample was positive for AE1/AE3, Napsin A and TTF-1, and negative for CDX-2, Thy, AE1/AE3, PAX-8 and PSA. The Ki-67 index was 60%. These findings were suggestive of metastatic LUAD (Figure 2).
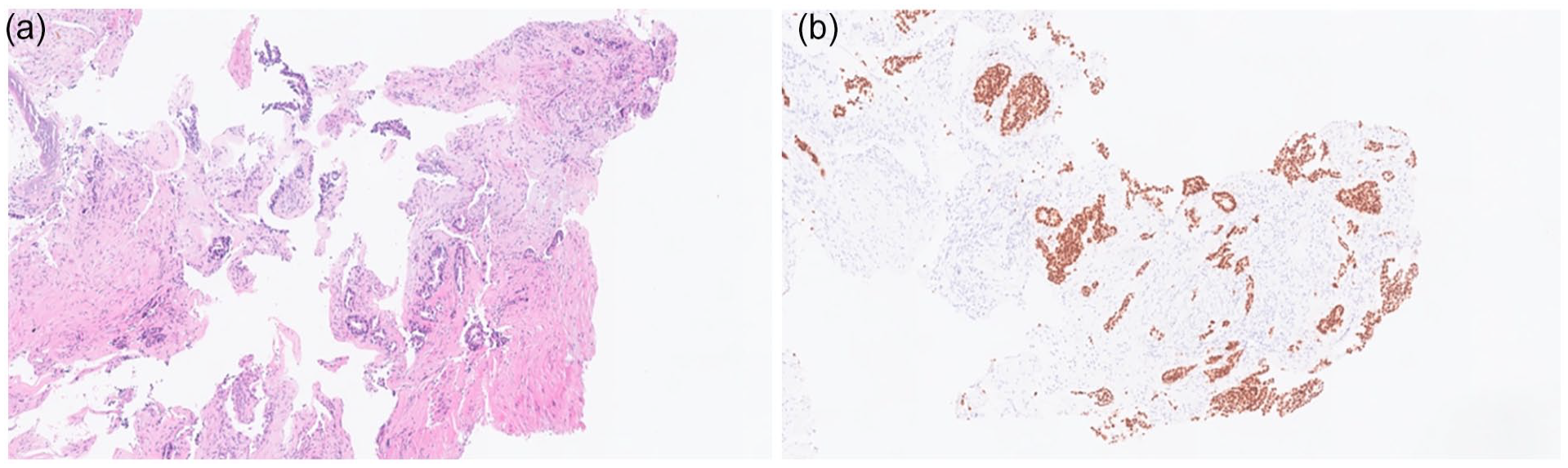
(a) Histopathologic image of excised tissue (hematoxylin-eosin). (b) Histopathological image of excised tissue Thyroid transcription factor-1 (TTF-1).
The patient was then given targeted therapy with third generation epidermal growth factor receptor (EGFR) - tyrosine kinase inhibitor (TKI) in the local hospital and remains asymptomatic 1 year after his first development of facial pain.
Discussion
We identified 13 case reports of metastatic lesions in ITF and its surrounding structures that included detailed patient information in English language articles published from 2000 to date. The clinical characteristics of the reported cases of metastatic ITF tumors are shown in Table 1. Cases of metastatic lesions that extend to ITF are included in this review.
Cases of Metastatic Lesions Extend to ITF.
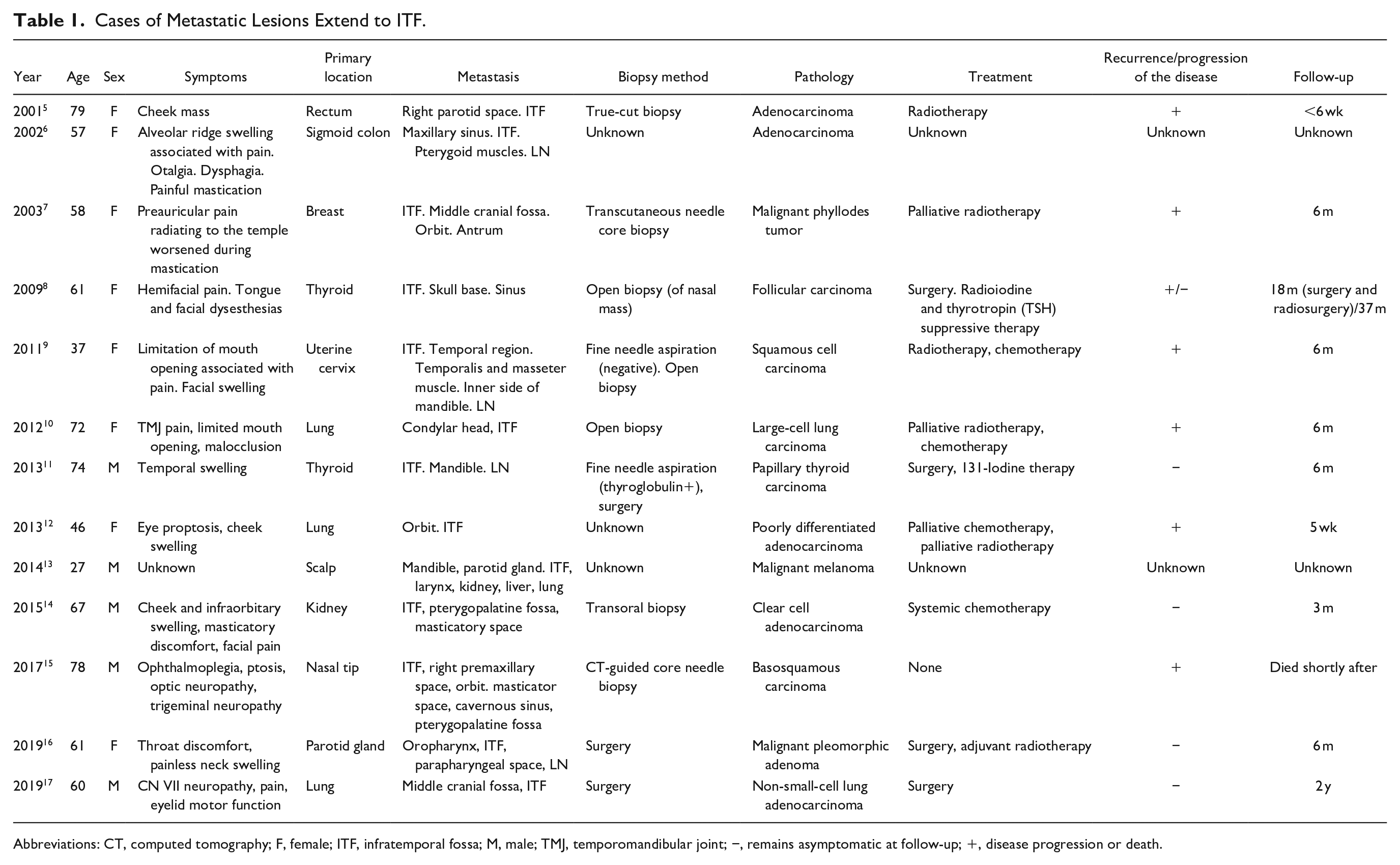
Abbreviations: CT, computed tomography; F, female; ITF, infratemporal fossa; M, male; TMJ, temporomandibular joint; −, remains asymptomatic at follow-up; +, disease progression or death.
ITF tumors are rare, making their general epidemiology little known. Lisan et al. 18 observed 62 patients consecutively in a 16-year period in a university hospital and found that the majority of ITF tumors were benign. The most common pathological types include juvenile nasopharyngeal angiofibroma, adenoid cystic carcinoma, and schwannoma. 18 Another recent published systemic review by Bin-Alamer et al. 19 centered on tumors involving ITF, suggesting schwannoma and meningioma being the most frequent pathological types, followed by synovial chondromatosis, squamous cell carcinoma and adenoid cystic carcinoma, with patients often presented with facial hypoesthesia, auricular/preauricular pain, headaches, and jaw deviation.
In the 13 case reports included in our literature review, the primary focus of these metastatic lesions was miscellaneous, including lung (3 cases), thyroid (2 cases), gastrointestinal tract (2 cases), skin (2 cases), kidney, breast, uterine cervix and parotid gland. The pathologic findings of 4 cases were adenocarcinoma (30.7%). The clinical symptoms were associated mainly with focal mass effects and adjacent structure involvement including TMJ,9,10 pterygopalatine fossa,14,15 orbit,7,12,15 paranasal sinus6,8 and cavernous sinus. 15 Patients were presented with facial pain and headache (n = 7), limited mouth opening (including painful mastication, n = 4), facial swelling (cheek, temporal and preauricular region, n = 3), neuropathy (including optic nerve, trigeminal nerve, and lower cranial nerves, n = 4), facial mass, eye proptosis and ophthalmoplegia. Limitation of mouth opening associated with pain often lead to diagnosis and treatment as TMJ dysfunction before further CT or MRI examination was introduced to make a definite diagnosis. 10 Therefore, one should be alert for ITF mass in case where TMJ disorder failed to conservative treatment.
The metastatic lesion in ITF often indicates distant metastasis and poor prognosis, therefore the treatment strategy was often non-surgical, accordingly to the histologic type with radiotherapy and/or chemotherapy. In our literature review, 5 cases were treated with surgery, four of which underwent postoperative treatments with radioiodine, radiotherapy or immunotherapy, and one had preoperative chemotherapy. Six cases had systemic treatment with radiotherapy and/or chemotherapy. The follow-up was described in 9 cases, and period ranges from 5 weeks to 6 years: 4 of which died, among them, 2 had radiotherapy, and 2 had radiotherapy combined with chemotherapy.
In this case, we reported a malignant ITF mass which was finally confirmed by biopsy as a metastatic LUAD. The patient presented with severe pain over the temporal area, limited mouth opening and hypoesthesia in a trigeminal nerve territory, and was first diagnosed as periodontitis. Radiologically, the appearance of the lesion was not specific apart from evident bony destruction of surrounding areas, which often indicates malignancy, corresponding with hypermetabolism in the PET-CT scan. Considering a suspicious secondary lung cancer and bone metastasis, an open biopsy was performed to reveal adenocarcinoma positive for TTF-1, indicating a metastatic lung cancer according to history.
Conclusion
In summary, an ITF mass can be suspected when patients present with severe facial pain worsened with occlusion, limited mouth opening, and have no response with local treatment to TMJ dysfunction. Metastasis in this area can be insidious and often have a late presentation. A fine-needle biopsy can fail to make a diagnosis and an open biopsy should be required. A thorough evaluation was required before treatment since multiple metastasis can be presented. Treatment plans were often made according to histologic types. Combined therapy with radiotherapy, chemotherapy and surgery was commonly undertaken. With the development of targeted therapy and immunotherapy, survival time was expected to be prolonged.
Footnotes
Data Availability Statement
No new data were generated or analyzed in support of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was funded by National High Level Hospital Clinical Research Funding (grant number 2022-PUMCH-B-096), National Natural Science Foundation of China (grant number 82071027).
Ethical Statements
The ethical approval of retrospective individual case reports was waived by the Ethics Committee of Peking Union Medical College Hospital, and the informed consent has been acquired from the patient. All the authors have followed the applicable ethical standards to maintain the research integrity without any duplication, fraud, or plagiarism issues.