
Abstract
Skull base metastatic tumors are rare. Breast cancer in particular can cause bone metastases after a long period of time. A 70-year-old woman presented with multiple cranial nerve palsy. Magnetic resonance imaging revealed a lesion that extended from the orbit to the base of the skull, and the patient was referred to our department. Ophthalmological evaluation showed left visual acuity impairment, left oculomotor nerve palsy, and left trochlear nerve palsy. Endoscopic biopsy performed 5 years after the completion of breast cancer treatment revealed skull base metastases. In unilateral multiple cranial nerve palsy, the possibility of skull base metastases should be considered.
Introduction
Breast cancer often causes bone metastasis. We present the case of a patient who presented with ptosis and diplopia and was found to have skull base metastasis of breast cancer.
Case Report
A 70-year-old woman with diabetes mellitus, cerebral infarction, and a history of breast cancer presented to our Department of Neurology with diplopia and left eyelid ptosis for 2 months. Magnetic resonance imaging (MRI) revealed a lesion from the orbit to the base of the skull, and the patient was referred to our department. Ophthalmological evaluation showed left visual acuity impairment, left oculomotor nerve palsy, and left trochlear nerve palsy.
Endoscopy showed no abnormal findings in the nose, and contrast-enhanced computed tomography (CT) showed an irregular mass around the upper left orbital margin, frontal sinus, ethmoidal sinus, upper intraorbital margin, orbital apex, and skull base (Figure 1A). Multiple lymph nodes with a 1-cm diameter were found in the mediastinum. Magnetic resonance imaging showed a mass extending from the base of the anterior skull to the left ethmoid sinus, frontal sinus, and intraorbital to orbital apex, with reticulation on contrast (Figure 1B and C). Positron emission tomography–CT demonstrated fluorodeoxyglucose accumulation in the mass from the left anterior skull base to the left frontal sinus and orbit, as well as in the sternocleidomastoid, right scapula, cervical spine, thoracic spine, lumbar spine, and femur (Figure 1D).
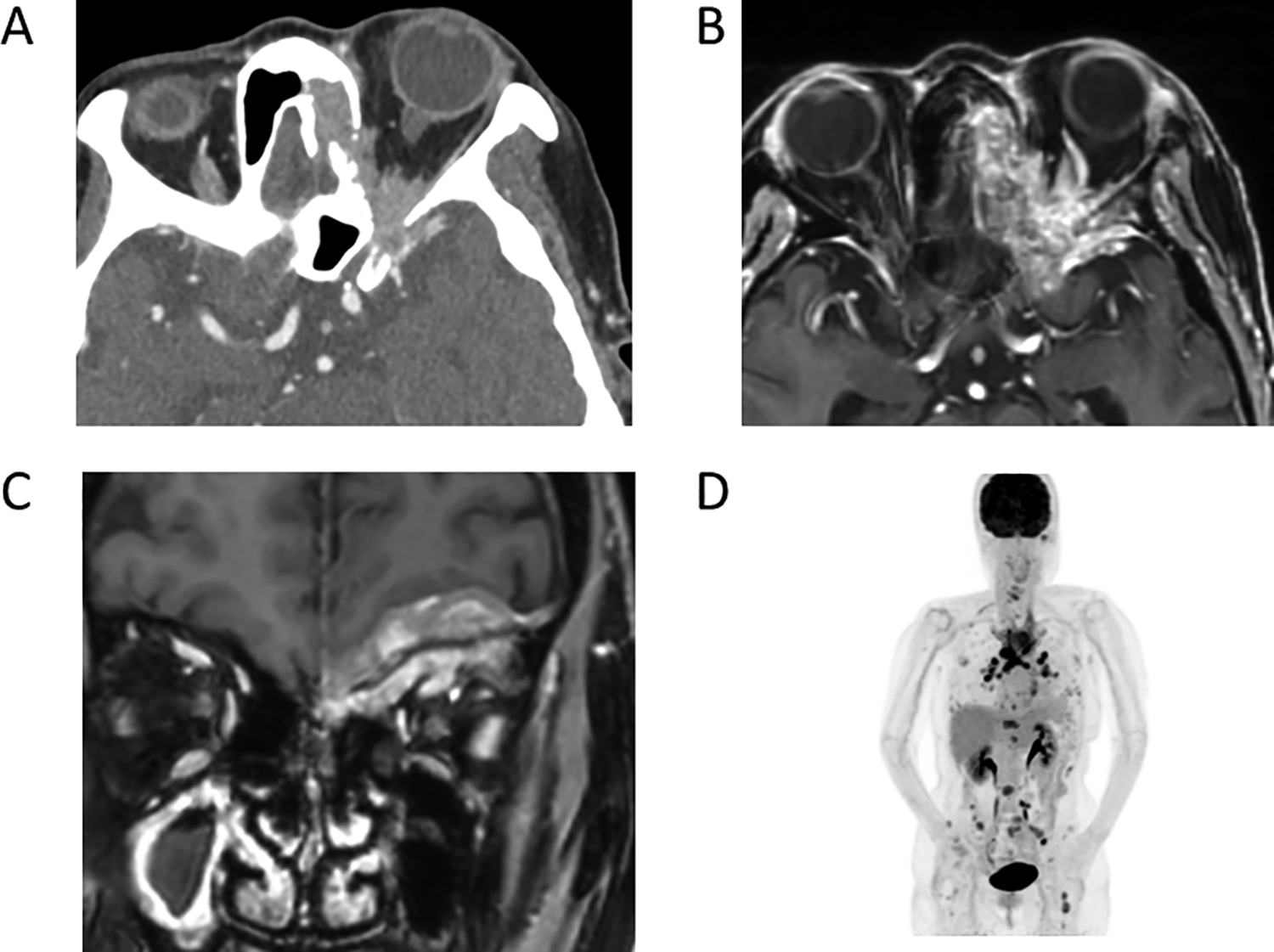
A, Axial contrast-enhanced computed tomography (CT) from the orbital apex to the ethmoid sinus and skull base, showing bony destruction in the skull base and the medial part of the orbit. B, Axial, T1-weighted, contrast-enhanced magnetic resonance imaging (MRI) shows findings similar to those of CT, and a fuzzy contrast effect from the orbital tip to the ethmoid sinus and skull base. C, Coronal, T1-weighted, contrast-enhanced MRI shows an uneven contrast effect centered on the left anterior skull base and intracranial and intraorbital areas. The right maxillary sinus demonstrates contrast enhancement along the edge and a low-intensity central area suggesting sinusitis. D, Positron emission tomography–CT showing swollen systemic lymph nodes and uptake in the vertebrae and femur.
Based on these results, we considered metastatic malignancy. The patient had a history of 5 years of additional treatment after surgery for breast cancer 10 years ago, and it had been 5 years since her last treatment, the presumptive diagnosis was systemic metastatic recurrence of breast cancer. Biopsy of the lesion at the skull base was performed by transnasal endoscopy to confirm the diagnosis and revealed a relatively hard mass.
Pathology
The lesion consisted of atypical cells with enlarged nuclei, which showed cribriform architecture (Figure 2A). These atypical cells were positive for estrogen receptor (Figure 2B), androgen receptor (Figure 2C), progesterone receptor (Figure 2D), CK AE1/AE3, and CK7 on immunohistochemistry but were negative for CK20. These results suggested that the lesion represented postoperative metastatic recurrence of breast cancer.
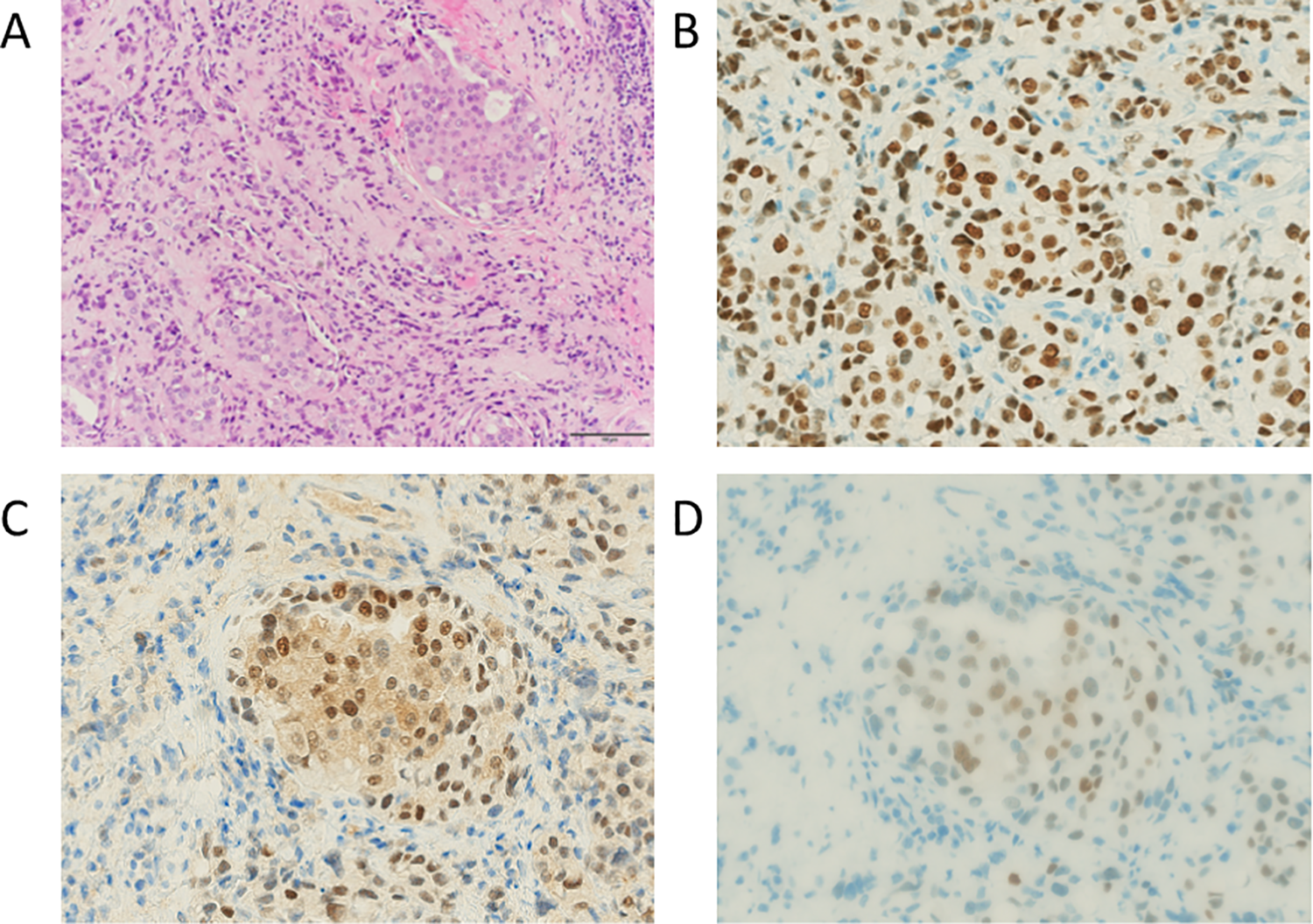
Histology of biopsy specimens of orbital lesions (scale bar size: 100 µm). A, Hematoxylin and eosin staining. B, Immunohistochemical staining of estrogen receptors. C, Immunohistochemical staining of androgen receptors. D, Immunohistochemical staining of progesterone receptors.
Thus, the patient was diagnosed with systemic and skull base metastatic breast cancer, and she was treated with chemotherapy.
Discussion
Although brain metastases are relatively common, metastasis to the skull base is rare; breast, lung, and prostate cancers are the most common malignancies that metastasize to this location. 1
As in this case, skull base metastases typically progress asymptomatically and are eventually identified due to the onset of cerebral neuropathy.2,3 Greenberg et al classified syndromes caused by skull base metastases according to location: orbital (7%), parasellar (16%), middle fossa (35%), jugular foramen (16%), and occipital condyle (21%). 4 Our patient exhibited the orbital syndrome. Although classification by site is useful, the condition sometimes involves areas that are difficult to classify. In the present case, the superior orbital fissure was affected and the patient presented with oculomotor and glenoid nerve paralysis.
A retrospective review of 22 patients with breast cancer metastasis in the head and neck region showed that metastasis occurred in the cervical lymph nodes in 8 patients, followed by orbital soft tissues in 5 and the skull base in 3. 5 There have been reports of sinus metastasis, orbital invasion, and symptoms of orbital syndrome.6,7
Contrast-enhanced MRI is the most important diagnostic imaging tool. Computed tomography is also useful for evaluating the bone itself. In many cases, biopsy may be required. It may also be necessary to differentiate between primary skull base tumors and invasive fungal infections of the sinuses. Endoscopic biopsy is an important technique for this purpose. Even at the base of the skull, however, biopsies may be dangerous in some locations, in which case puncture aspiration cytology or clinical diagnosis with imaging may be used.
Treatment options include radiation therapy, anticancer drugs, surgery, and gamma knife surgery. 8 Early radiation therapy after the onset of symptoms has been reported to be important for improving neurological symptoms. 2 The patient in this case opted for chemotherapy but not radiotherapy because it was difficult to gauge the proximity of the tumor to the optic nerve, and the risk of radiation-induced loss of vision could not be adequately assessed.
Clinicians should keep in mind the possibility of skull base tumor and cancer metastasis to the skull base, especially in patients who present with unilateral cerebral nerve palsy.
Footnotes
Authors’ Note
K.A. and Y.M. contributed equally to this manuscript. K.A. and Y.M. wrote the manuscript. Y.M., M.H., and Y.K. reviewed the literature. K.A., Y.M., and S.N. created the figures. K.N., S.O., A.N., T.T., K.T., E.M., and H.I. provided advice on patient treatment and edited the manuscript. All authors discussed the results and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number T17K113590.