
Abstract
Metastatic skull base malignancies infrequently occur but, when present, typically arise from breast malignancies. Pterygopalatine fossa (PPF) metastasis of any malignancy is further seldom reported, and metastasis of gynecologic malignancies to the PPF has not been previously described in the literature. We present a single case of a 42-year-old female with the first likely case of high-grade endometrial sarcoma metastatic to the PPF. The patient presented with facial pain and numbness in the V2 distribution presented for evaluation. History was significant for several months of dysmenorrhea and metrorrhagia. Computed tomography, magnetic resonance imaging, and positron emission tomography imaging revealed a PPF mass with local extension and bony metastases. Endoscopic biopsy was performed, and final pathology was most consistent with metastatic high-grade endometrial stromal sarcoma. This is the first reported case of likely metastatic endometrial sarcoma to the PPF. This case report highlights the possibility of rare distant metastasis of gynecologic malignancy to this area of the skull base.
Keywords
Introduction
Skull base malignancies represent a challenging diagnostic entity due to the wide differential diagnosis upon patient presentation. Cranial nerve involvement with associated symptoms is the most commonly reported presentation of skull base metastatic disease. 1 -5 Pterygopalatine fossa (PPF) metastasis has rarely been reported. Reports of trigeminal neuralgia secondary to breast cancer metastasis to the PPF have been described. 6 -8 Ptosis, visual changes, and paresthesia have all been described secondary to skull base metastasis of endocrine and gastrointestinal malignancies. 1,2,4
Endometrial stromal sarcoma (ESS) is a rare aggressive malignancy accounting for 3% to 7% of uterine malignancies. 9 Endometrial stromal sarcoma is categorized histologically as low grade or high grade, with the latter portending a worse prognosis. 9 High-grade ESS frequently metastasizes to the lungs. 10 To date, ESS metastasis to the skull base has not been described. We report a case of high-grade ESS likely metastatic to the PPF.
Case Report
A 42-year-old female with no past medical history was referred to clinic with 1.5 months of progressively worsening right-sided sharp electric pain and numbness in the maxillary nerve distribution (V2). Associated symptoms included jaw pain with mouth opening, right ear pain, right neck pain, back pain, rib pain, unintentional weight loss, and fatigue. Upon examination, right-sided facial numbness in the V2 distribution was noted. There was no evidence of facial paralysis, ocular motor disturbances, or sinus tenderness. Rigid nasal endoscopy was unremarkable for masses. The patient had been seen by gynecology for an 8-month history of dysmenorrhea and metrorrhagia.
A computed tomography (CT) maxillofacial was obtained and revealed a mass centered in the PPF with extension into the infratemporal fossa, inferior orbital fissure, and sphenoid sinus. A magnetic resonance imaging (MRI) was remarkable for a large necrotic mass involving the right base of the pterygoid and greater wing of the sphenoid with extension to the right masticator and parapharyngeal spaces (Figure 1). Additional local extension was noted to the cavernous sinus, inferior orbital fissure, foramen rotundum, and vidian canal. Abnormal marrow signal with enhancement involving the left parietal bone, clivus, and both occipital condyles was also noted separately from the lesion.
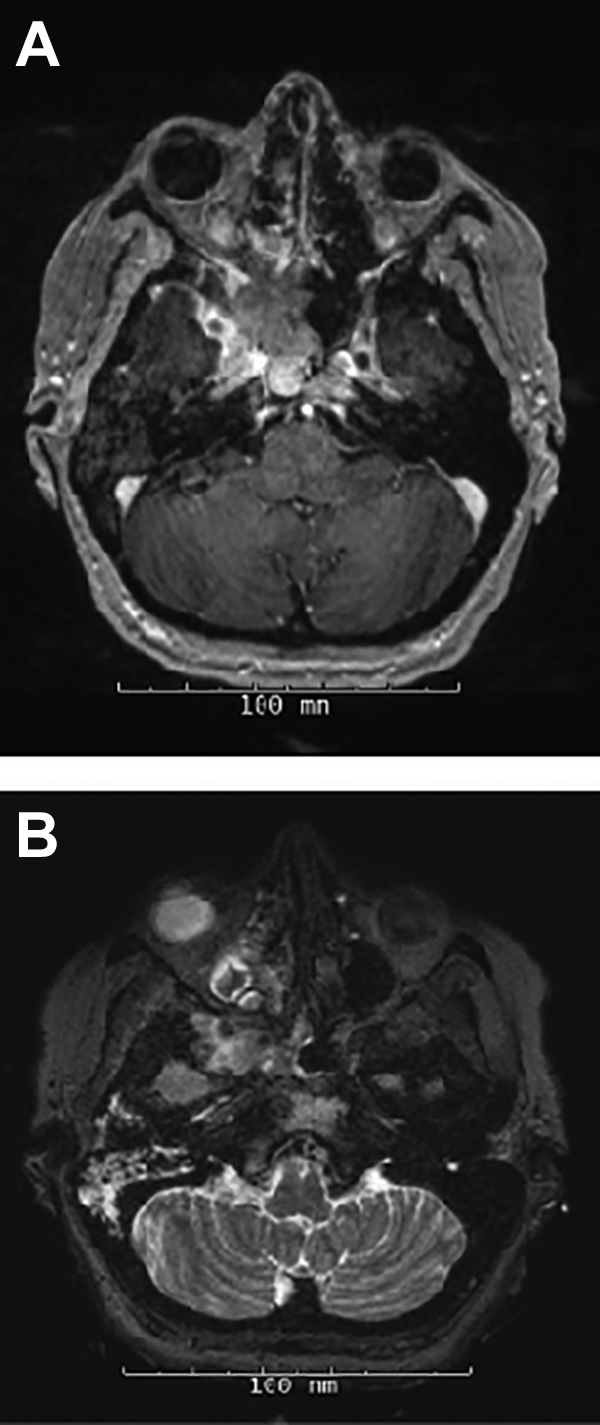
Axial T1-weighted magnetic resonance imaging (MRI) (A) and axial T2-weighted MRI (B) with gadolinium showing pterygopalatine neoplasm involving the right base of pterygoid and greater wing of sphenoid extending into the right masticator and parapharyngeal spaces.
The patient underwent endoscopic approach to the PPF with biopsy of the mass due to concern for aggressive malignancy. The final pathology report was most consistent with metastatic high-grade ESS. Positron emission tomography (PET) imaging demonstrated abnormal uptake in the right lateral and medial pterygoid region, clivus, multiple osseous structures of the spine, pelvis, bilateral femurs, ribs, bilateral humeri, sternum, and retroperitoneum. The largest focus of abnormal uptake was in the uterus, which appeared to be massively enlarged.
After interdisciplinary review, a treatment plan was formulated including hormone therapy with megestrol acetate and neoadjuvant chemotherapy consisting of gemcitabine and docetaxel. The role of surgery will be considered if the patient’s metastatic disease responds favorably to systemic therapy.
Discussion
Here we report the first case of likely metastatic ESS to the PPF. Pterygopalatine fossa metastasis of any malignancy is infrequently reported in the literature. Breast cancer metastasis to the PPF presenting with trigeminal neuralgia has been described. 6 -8 Hepatocellular, prostate, and follicular thyroid carcinomas metastasizing to other regions of the skull base have been reported with patient presentations including ptosis, lateral gaze palsy, diplopia, facial dysesthesia, and facial weakness. 1,2,4 Uterine sarcomas tend to be locally aggressive but can metastasize to distant locations. 11 These tumors most commonly disseminate to the lung, liver, and peritoneum. 11 Gynecological malignancies to the skull base have rarely been reported. Sandruck et al described a case of uterine leiomyosarcoma metastasis to the sphenoid sinus after 2 years free of disease. 11 Metastatic uterine leiomyosarcoma to the anterior cranial fossa with intracranial and intraorbital extension presenting with proptosis and neurological deficits was reported by Mariniello et al. Metastasis of ESS malignancies to the PPF has not been reported. 12
High-grade ESS is a rare malignancy comprising 0.2% of all uterine malignancies with an occurrence of extrauterine spread as high as 80%. 9,13 Metastasis has been reported to occur 20 years after diagnosis. 13 Endometrial stromal sarcoma is most prevalent in women between the ages of 42 and 58. 13 It comprises less than 10% to 15% of uterine sarcomas. 14 Diagnosis is made with tissue pathology. Histopathology is characterized by stromal cells, high mitotic figures, and areas of necrosis (Figure 2). CD10, a marker of smooth muscle, may be positive in ESS, but it is nonspecific (Figure 3). 15 Tamoxifen therapy and unopposed estrogen exposure are hypothesized to play roles in the pathogenesis. 13 Surgery is the optimal treatment for high-grade ESS. 9,13 Recurrence rate after surgical resection ranges from 70% to 90%. 9 Hormone therapy is indicated in unresectable tumors and may be considered for disease recurrence and stage II-IV disease. 13 Options for hormone therapy include megestrol acetate, GnRH analogues, and aromatase inhibitors. 13 Prognosis is poor for these patients. 14,13 An 11% 5-year survival rate has been reported for patients with distant metastasis. 13
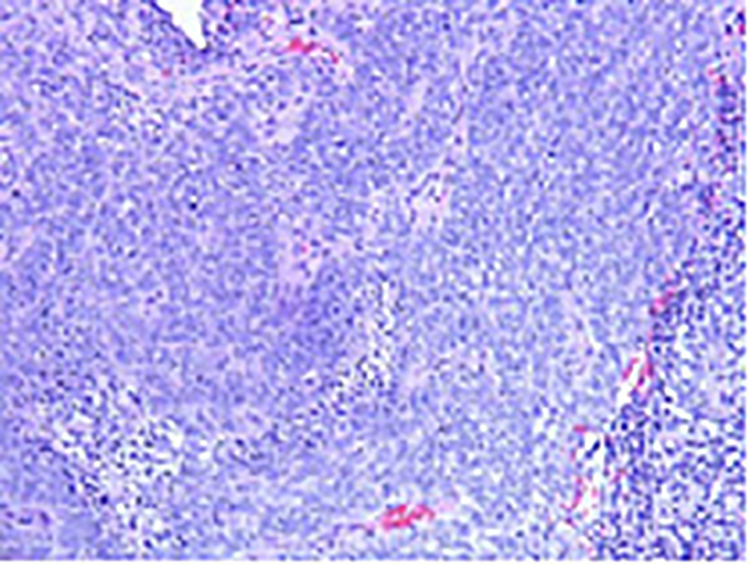
H&E stain of endometrial stromal sarcoma at ×40 magnification depicting jagged edge stromal cells with mitotic figures (short arrow) and areas of necrosis (long arrow).
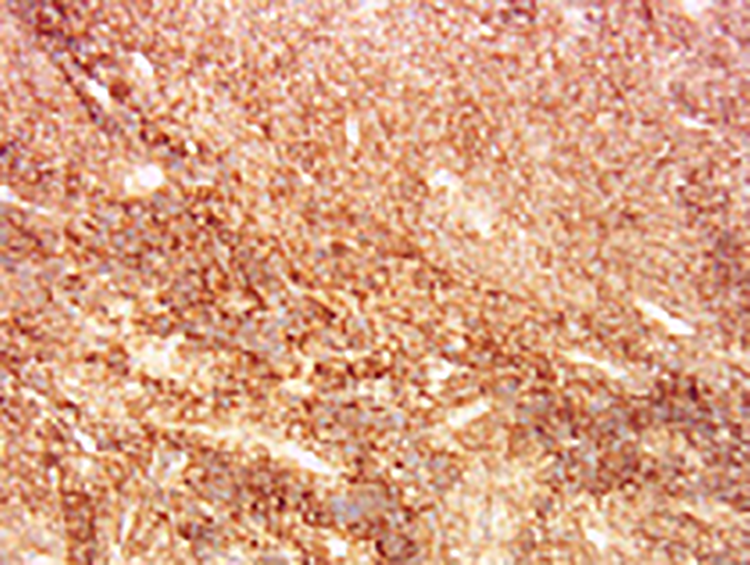
Endometrial stromal sarcoma stained with CD10 at ×20 magnification.
Clinical presentation of lesions of the skull base is dependent upon the type and location of the lesion. 3 Symptoms secondary to cranial nerve involvement may be the initial presentation of malignancy. 2,3 Trigeminal neuralgia, facial weakness, and ophthalmoplegia have all been described in skull base metastatic lesions. 1,2,4 Physical examination findings should prompt imaging with CT and MRI. However, combination imaging with CT and MRI has a reported false-negative rate as high as 25% in patients with metastatic skull base malignancies. 2 Single-photon emission computed tomography or PET imaging of the skull base may be used to improve diagnostic accuracy in such cases. 2 Tissue pathology is paramount in confirming the diagnosis. In the presented patient, a history of gynecological symptoms alerted the physician of potentially metastatic disease.
To our knowledge, this is the first case of ESS metastatic to the PPF reported in the literature. Metastatic gynecologic malignancies should be considered in patients with skull base lesions, particularly in patients with coexistent gynecological symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article.