
Abstract
Oculomotor nerve palsy (ONP) is an extremely-uncommon complication of endoscopic endonasal surgery (EES). To date, there have been only 6 reports of immediate ONP post-EES in the PubMed/MEDLINE-indexed literature. This report illustrates the clinical presentation of complete, pupil-involving ONP that recovered fully over 6 months after surgery in a 28 year-old man who underwent medial maxillectomy through endoscopic modified Denker’s approach for sinonasal inverted papilloma. An attempt has been made to evaluate the possible etiology for such a complication through a thorough literature review, and following an in-depth introspection of the surgical team. The relevant surgical anatomy and the management aspects are also discussed in detail. This report provides a caveat to the endoscopic endonasal surgeons and the residents regarding ONP as an unexpected and unusual complication of sinus and skull-base surgery. It further underlines the importance of being knowledgeable of the somatic and parasympathetic neural anatomy of the oculomotor nerve in the skull base, and of the finesse and meticulous dissection that are needed for a safe surgery around the confines of the orbit.
Keywords
Introduction
Endoscopic endonasal surgery (EES), the essential surgical armamentarium for addressing various endonasal, paranasal sinus, orbital, nasolacrimal drainage pathway, anterior skull-base and pituitary/sellar disorders, has an established array of complications.1,2 These include the orbital injuries, which, although uncommon, can be devastating and vision-threatening, and an endoscopic sinus and skull-base surgeon is always wary of them. The anatomic proximity to the paranasal sinuses exposes the orbits to intraoperative injuries. The orbital complications of EES may range from an apparently-innocuous orbital fat prolapse following a breach in the lamina papyracea to the devastating optic nerve injury leading to blindness, and a few of the well-documented complications include localized hematomas, lacrimal duct injury, retro-orbital hemorrhage, extraocular muscle injury.1,3 -7 However, oculomotor nerve palsy (ONP) is an extremely-rare complication of EES, with a very few events reported to date. In this clinical report, we describe the clinical features of ONP post-EES that persisted 6 months after the surgery. Such a complication was unexpected, leading us to introspect and search for 1 or more plausible etiologies for the ONP, perform a through literature review, and outline an optimum, interdisciplinary management.
Case Report
A 28 year-old man, a software engineer by profession, underwent endoscopic medial maxillectomy (modified endoscopic Denker’s procedure) under general anesthesia for a biopsy-proven inverted papilloma involving his left nasal cavity and maxillary sinus (Figure 1). He was otherwise healthy and had no known comorbidities. His preanesthetic workup was unremarkable. Prior to surgery, a greater palatine canal nerve block was administered with 4 ml of premixed local anesthetic-vasoconstrictor agent (lignocaine 2% and adrenaline [1:1 00 000]) to control an imminent posterior epistaxis during the EES. The surgery went uneventfully, and the tumor was excised fully along with the medial maxillectomy bone specimen.
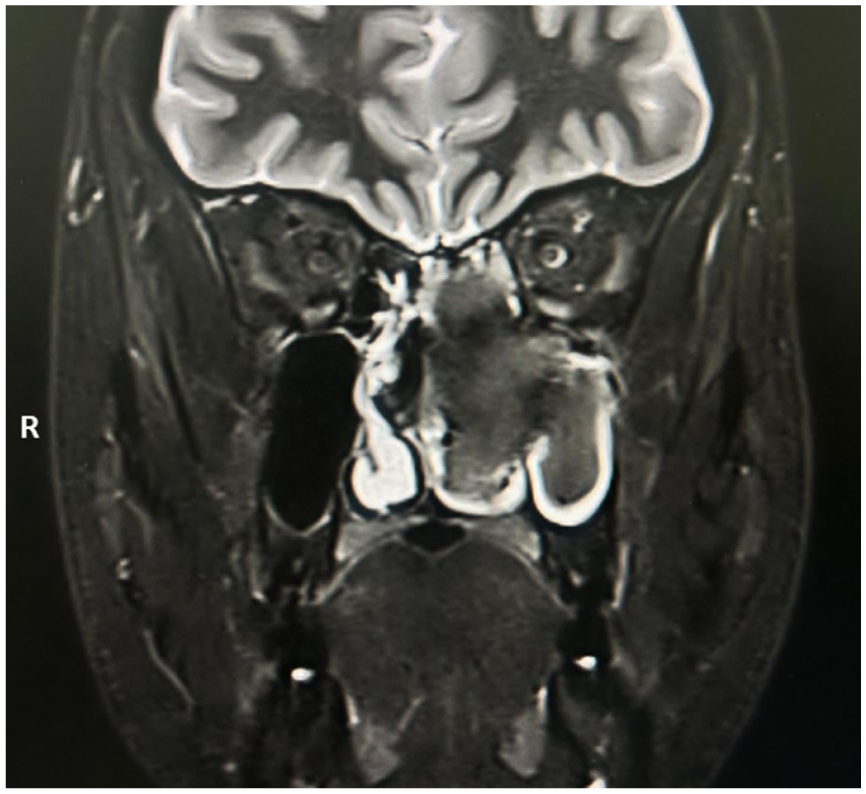
Gd-MRI of the nose and paranasal sinuses in a 28 year-old man showed a mass lesion involving the left nasal cavity and left maxillary sinus; the biopsy of this lesion turned out to be an inverted papilloma. Gd-MRI, Gadolinium-enhanced magnetic resonance imaging.
The patient tolerated the procedure well and recuperated satisfactorily in the immediate postoperative period. However, as he recovered from the postanesthesia sedation, we noticed a left-sided total ptosis with diplopia (evident on manual elevation of the upper eyelid), along with dilated, non-reacting left pupil, suggesting a complete left ONP. His vision, however, was fully preserved. We removed the anterior nasal packs immediately and advised an urgent Gadolinium-enhanced magnetic resonance imaging (Gd-MRI) of the nose, paranasal sinuses, and orbits to exclude any inadvertent iatrogenic breach in the anatomic confines of the surgical limit (lamina papyracea, intra-orbital contents) that could have otherwise injured the oculomotor nerve. Simultaneously, a thorough retrospection among the surgical team members was carried out; however, we had no recollection of any inadvertent/accidental injury to the lamina papyracea and maxillary sinus roof (orbital floor) and the posterior wall (anterior confines of the pterygopalatine fossa). The Gd-MRI corroborated our introspection, and did not show any breach in the confines of the sphenoid and maxillary sinuses, lamina papyracea, or pterygopalatine fossa, nor was there any leakage of dye in the cavernous sinus, indicating the anatomic integrity of the skull base (Figure 2A–C). Ischemic and inflammatory blood workup were also within normal limits.
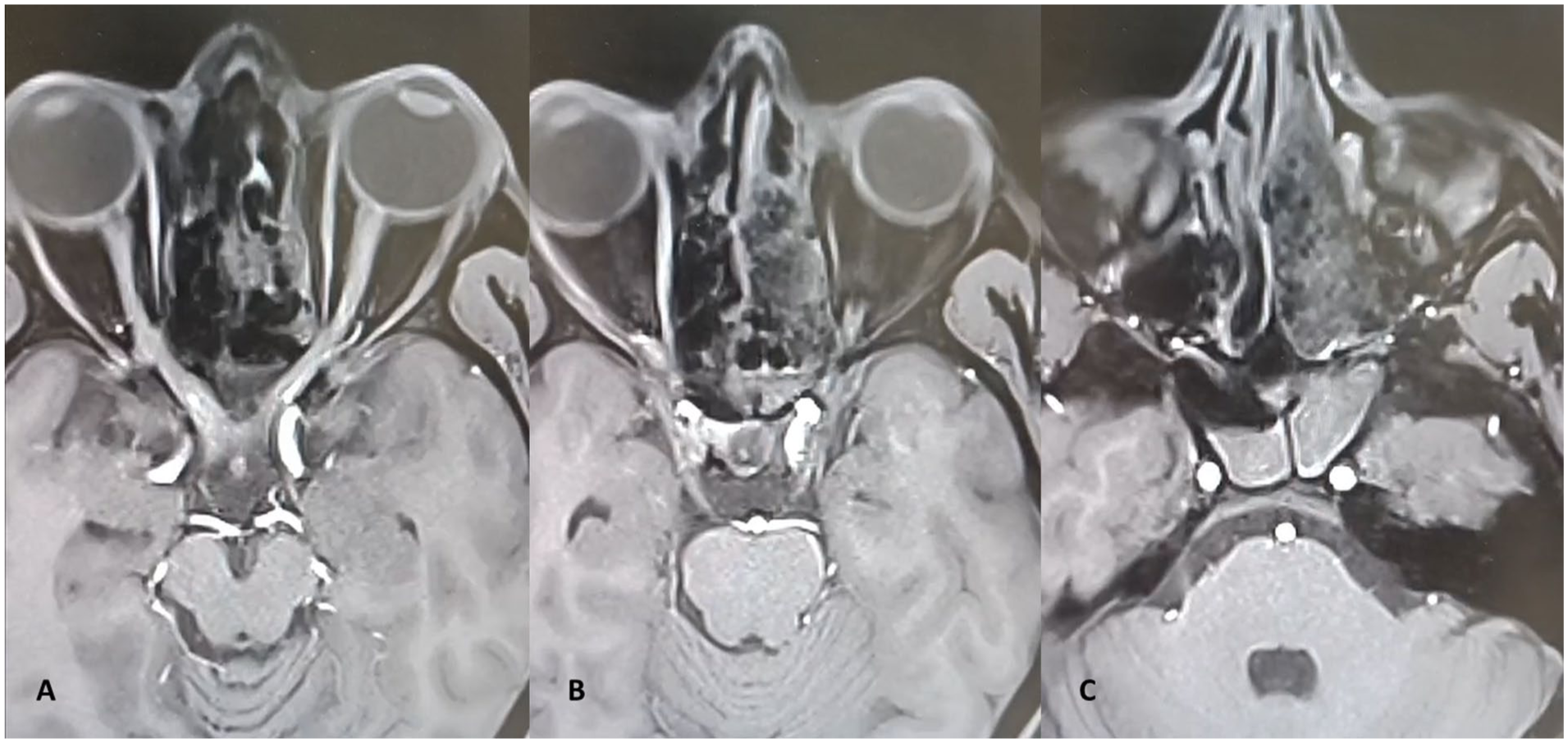
Postoperative Gd-MRI showed no breach in the confines of the left orbit (A, B), sphenoid sinus, and pterygopalatine fossa (C), with postoperative soft-tissue changes in the left sinonasal cavity. There is no spillage of dye into the cavernous sinuses, indicating integrity of the skull base (A, B). Gd-MRI, Gadolinium-enhanced magnetic resonance imaging.
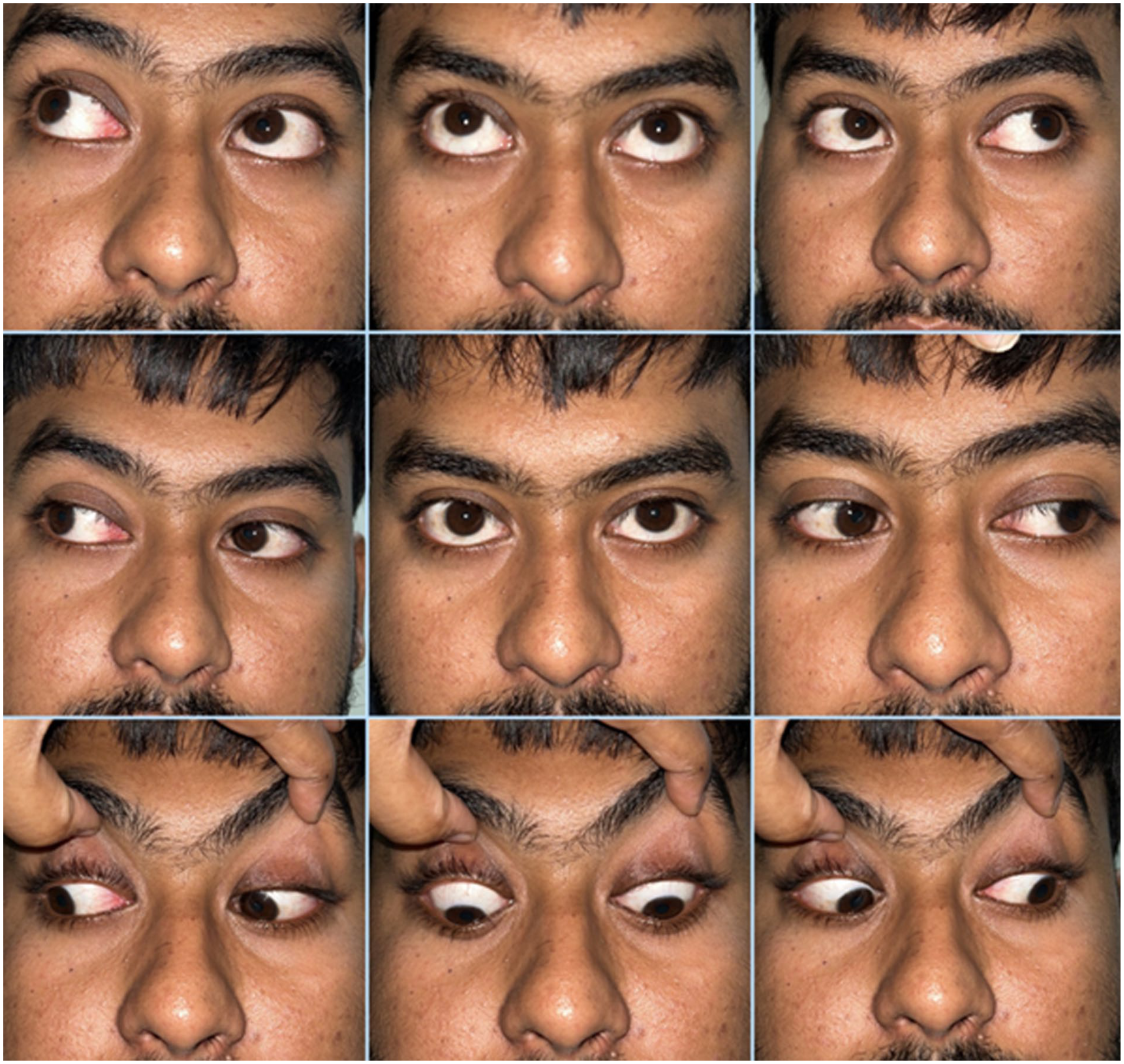
We sought for an immediate neuro-ophthalmology consultation. On detailed clinical examination, the patient was found to have 20/20 vision in both the eyes for distance. However, his near vision was N6 for the right eye and N8 for the left (operated side). Extraocular and intraocular findings for his right eye were within normal limits. The left eye showed total ptosis with exotropia and hypotropia, along with limited extraocular movements (elevation − 5, depression − 4, adduction − 5; Figure 3). Anterior segment examination showed anisocoria with a dilated, non-reacting pupil in the left eye; rest of the anterior and posterior segment findings were unremarkable. Dilated fundus evaluation did not show any abnormality.
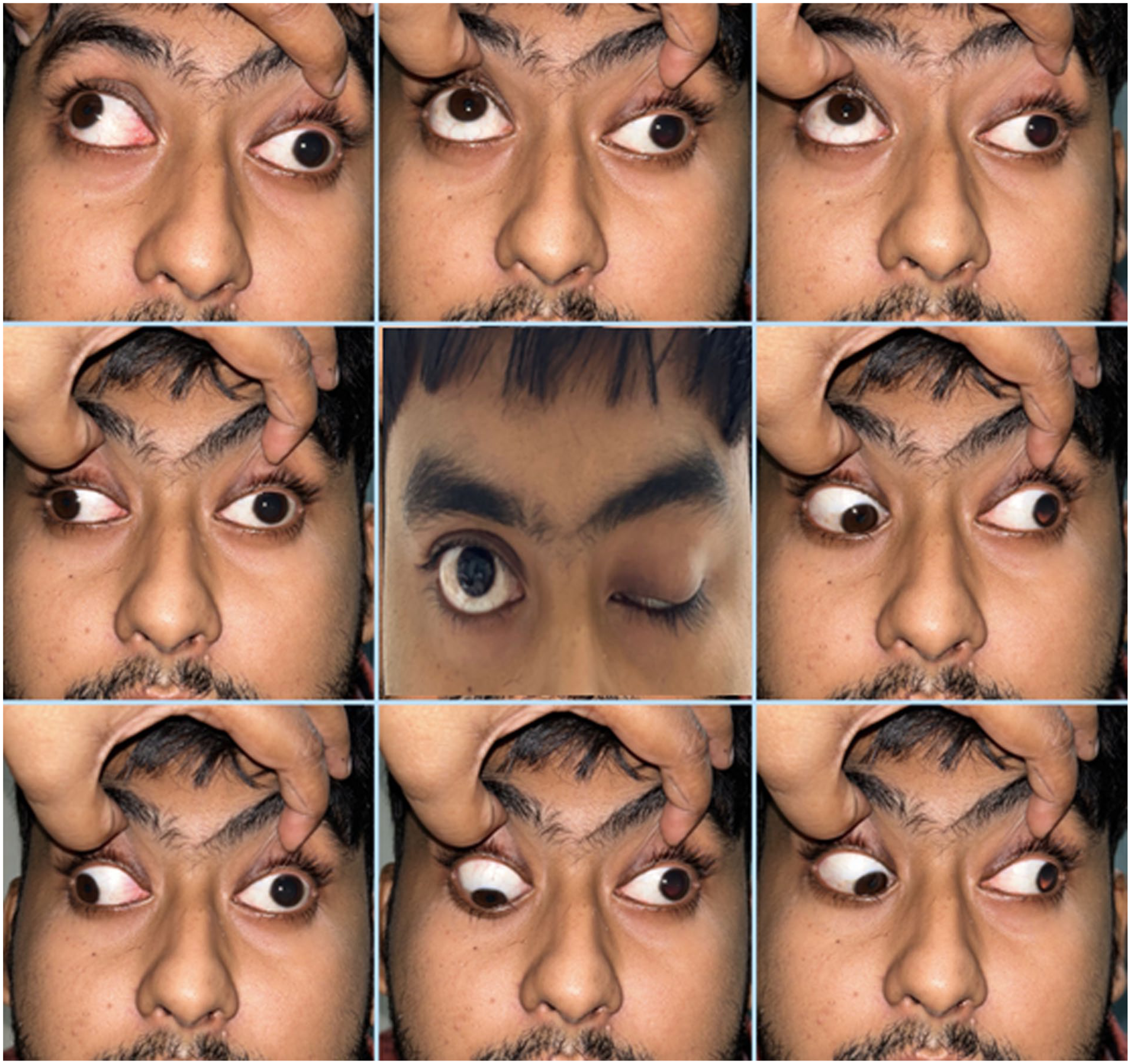
Following the endoscopic endonasal procedure, the left eye showed total ptosis with exotropia and hypotropia, along with limited extraocular movements (elevation − 5, depression − 4, adduction − 5).
The patient was diagnosed with ONP post-EES of the left side, the etiology being under evaluation. We counseled and re-assured him and his parents, explained them about the unpredictability of the situation, and motivated them for a watchful observation and to be under continuous follow-up for the next few weeks. We also sought help from a professional counselor to counter any possible depression that might set in the young man. We put him on intravenous dexamethasone (8 mg thrice/day for 10 days), followed by a tapering dose of long-term oral steroids (methylprednisolone loading dose @ 48 mg/day, 32 mg/day, and 16 mg/day; each for successive 7 day periods). Meanwhile, we performed endoscopic evaluation of the operated nasal cavity periodically and advised him alkaline nasal douching. The nasal cavity gradually healed, and the histopathology report received confirmed an inverted papilloma. We monitored him closely, carefully, and at regular intervals for his eye condition. He gradually showed signs of improvement of oculomotor nerve function from 1 month after the surgery. The improvement was gradual, but at a steady state, and he had a complete recovery without any diplopia and ptosis at the end of 6 months (Figures 4, 5; Table 1). He is presently under follow-up every 3 months for more than a year of his EES, with no recurrence of inverted papilloma, with normal ocular functions, and leading a normal personal and professional life.
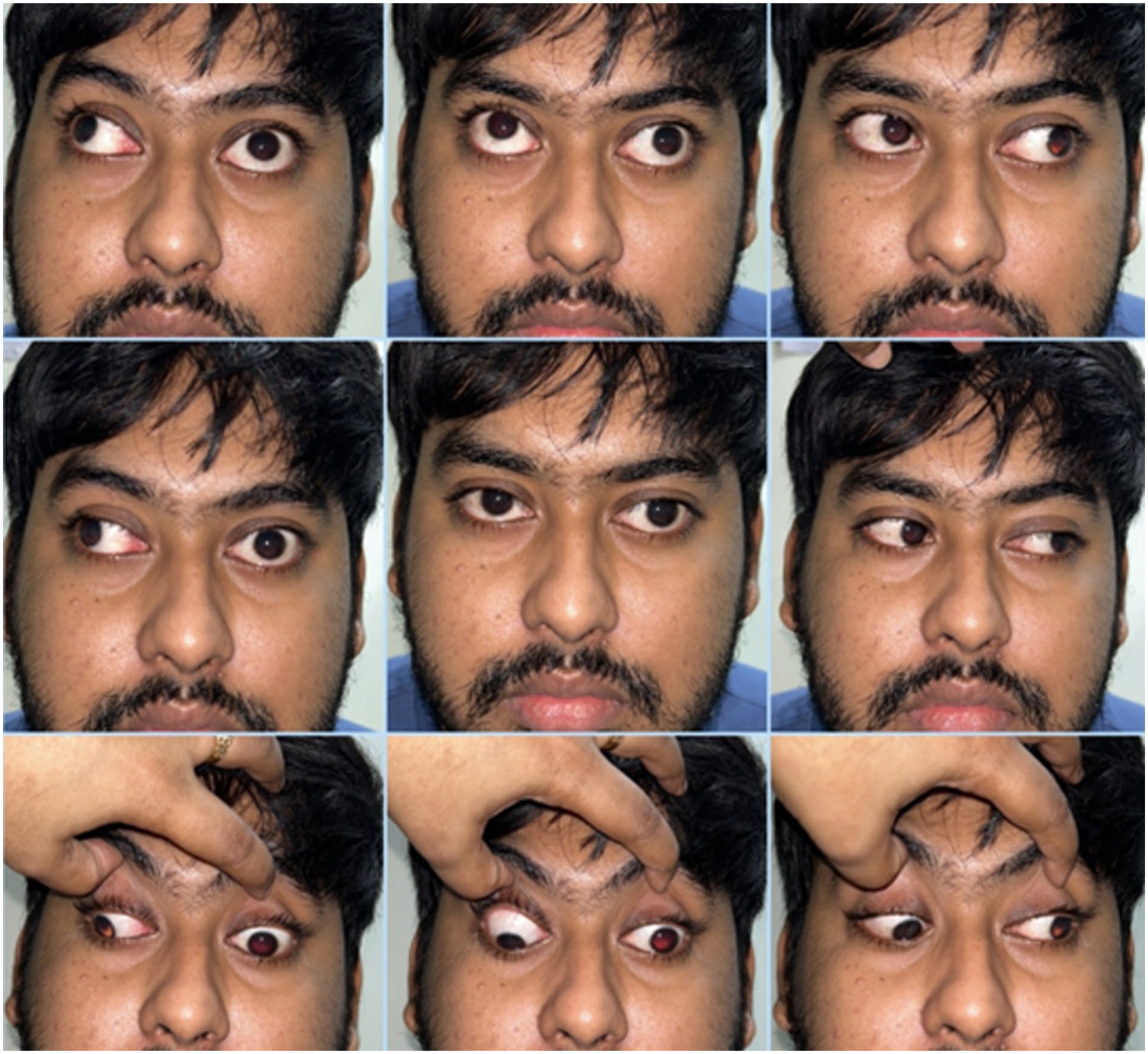
The patient started to show signs of recovery of oculomotor nerve function after 1 month of endoscopic sinus surgery. These were the evaluation photographs at 2 months of the postoperative period that showed partial recovery of ophthalmoplegia and ptosis (elevation − 3, depression − 3, adduction − 4).
At 6 months postsurgery, the patient had a full recovery of oculomotor nerve functions.
Evolution of Left Oculomotor Nerve Function in our Patient During the Follow-up Period (From Complete Ptosis at First Postoperative Day to Full Recovery at 6 months).

We have obtained informed consent in writing from our patient seeking permission to reproduce his clinical details and photographs of his upper face that could potentially reveal his identity but were essential to have documentary evidence.
Discussion
Oculomotor Nerve Paresis as a Rare Complication of EES
Ocular complications following EES are well-documented and can be explained by the anatomic proximity of the orbits to the paranasal sinuses. The implications of an inadvertent orbital injury (including trauma to the anterior ethmoidal artery while working close to the anterior skull base) keep the endoscopic sinus surgeons well-alert during surgery. Thus, the incidence of iatrogenic orbital trauma is not common and is estimated to be <1%. 7 The notable complications documented in the literature include globe perforation, retinal hemorrhage, anisocoria, extraocular muscle injury, orbital hemorrhage, periorbital ecchymosis, breach in the lamina papyracea with orbital fat prolapse, enophthalmos, lipogranuloma, direct/indirect injury to the optic nerve, and damage to the lacrimal drainage system.1,8 However, ONP is 1 of the least common ocular complications of EES and has been seldom documented. To date, there are only 6 such patients on record in the PubMed/MEDLINE database; Table 2 summarizes the key findings from those reports (all single case reports, level 4 evidence) and explores the presentation, etiology, and management of ONP immediate post-EES.9 -14
Reports of Oculomotor Nerve Palsy Immediately Following EES Published in the PubMed/MEDLINE-Indexed Literature.

Abbreviations: ESS, Endoscopic Endonasal Surgery; (F)ESS, (functional) endoscopic sinus surgery; CRSwNP, chronic rhinosinusitis with nasal polyposis; CT scan, computerized tomography scan; CRSsNP, chronic rhinosinusitis sans nasal polyposis; OMC, ostiomeatal complex.
These were the only 2 instances where imaging definitely suggested an etiology (iatrogenic trauma in these patients).
No more details provided regarding management.
The Relevant Anatomy of the Oculomotor Nerve in Brief
The oculomotor nerve arises at the upper border of the pons.9,12 It contains voluntary motor nerve fibers (extraocular muscles, sphincter pupillae, ciliary muscles of lens) and preganglionic parasympathetic fibers. The nerve fibers penetrate the dura near the posterior clinoid process of the sphenoid and run in the lateral wall of the cavernous sinus before entering the orbit. It enters the intraconal space through the superior orbital fissure and splits into superior and inferior divisions. While the former supplies the superior rectus muscle, the latter divides into 3 branches to supply the medial rectus, inferior rectus, and inferior oblique muscles. The branch to the inferior oblique carries the preganglionic parasympathetic nerves (having their source at the Edinger-Westphal nucleus at pons, adjacent to the oculomotor nucleus) as the oculomotor root, which synapses at the ciliary ganglion within the orbital cavity. Postganglionic fibers from the ciliary ganglion supplies the sphincter pupillae and the ciliary muscles through the short ciliary nerves, resulting in constriction of the pupil and accommodation of the lens. The orbit and cavernous sinus are usually the most likely sites of iatrogenic injury during EES (conventional, and when extended), leading to ONP.
Literature Review of Patients With Post-EES ONP
Of the 6 patients described with partial ONP immediate post-EES, the etiology could be definitely diagnosed as inadvertent iatrogenic trauma in only 2 patients – 1 with bone fragment impinged through the lamina papyracea, and another with breach in the lamina, both resulting in direct/indirect traction on the oculomotor nerve (Table 2).12,13 While 1 of them required endoscopic reexploration and removal of the offending bone fragment, the other recuperated through conservative management. However, in the absence of a definitive etiology, the causations for the partial ONP post-EES in the remaining 4 patients were mentioned as theoretical, based on practical logic, the knowledge of the relevant surgical anatomy, and introspection of the surgical team. The imaging (when executed/available) were noncontributory in these 4 patients, and there was no other way to evaluate the exact etiology of ONP. However, given the fact that the functions of the oculomotor nerve returned in all the patients within a span of weeks to months, and because the nature of the injury was paresis rather than complete paralysis, a reversible cause sustained during the intraoperative period that led to neuropraxia could be speculated. The offending interventions could be local anesthetic drugs or nerve edema due to tissue manipulation.9 -11,14 Two more patients with nontraumatic diplopia post-EES were reported by Lam et al, 15 but they were of late onset (10 days and 30 days after the surgery), and both experienced significant duration of intraoperative hypotension (mean arterial pressure <75 mmHg) for more than 15 minutes. The period for anesthesia in our patient was, however, unremarkable, and cannot explain his postoperative ocular complications.
What Happened to Our Patient?
He too had an immediate post-EES ONP, but his presentation was different and unique in many aspects. His left-sided ONP was complete, with total ptosis, diplopia, and fixed, dilated pupil. He had a protracted recovery (over 6 months), although the nerve functions were fully regained. Interestingly, neither did the postoperative Gd-MRI scan reveal any evidence of violation of the lamina papyracea (breach, impingement of bony fragment, or pneumo-orbita), nor could we, as the surgical team, recollect any inadvertent intraoperative injury. These supposedly ruled out any overt intraoperative trauma to the oculomotor nerve. Similar to the hypotheses put forward by the other authors, our patient could have had an ischemic injury and/or perineural edema secondary to the pressure effect of an expanding anterior nasal pack, or a discrete, undetected microtrauma to the orbital confines (lamina papyracea, orbital floor) sustained during the endoscopic modified Denker’s procedure.
However, because the pupil was involved as a part of the ONP, and that the ONP itself was complete when diagnosed, a traumatic event seemed a strong possibility. The most probable factor at surgery could be the manipulation of the orbital floor when we removed its medial third as part of medial maxillectomy. This could have injured 1 or more branches of the inferior division of the oculomotor nerve that supplies the inferior rectus, inferior oblique, and medial rectus muscles, and also the preganglionic parasympathetic fibers carried through the branch to the inferior oblique as the oculomotor root, and/or the postganglionic fibers as the short ciliary nerves. This could explain both the ophthalmoplegia and ptosis, and also the pupillary involvement. This explanation seems plausible as the fibers supplying the pupil (the pupillomotor fibers) are typically at the periphery of the oculomotor nerve, which renders them prone to trauma (extrinsic injury [iatrogenic or otherwise] or compression [anterior nasal pack, edema]). 16
However, it is interesting to note that although the ONP seemed complete initially, our patient recovered fully at 6 months after being treated with long-term systemic steroids. Therefore, the extent of nerve injury could have been severe, but never caused neurotmesis or anatomic discontinuity.
In this context, another possible etiology – the effect of an overdose of local anesthetic-vasoconstrictor premix, was also considered during the introspection of the surgical team. We performed a greater palatine canal block in our patient at the onset of surgery. The greater palatine canal connects the oral cavity and the pterygopalatine fossa, and therefrom the orbit through the infraorbital fissure. Standard local anesthetic-vasoconstrictor premix (lignocaine 2% and adrenaline [1:1 00 000]) was used. The dosage, proportion, and amount of this premix have been standardized for this procedure (ie, 2 ml of lignocaine 2% and adrenaline [1:80 000]). 17 However, it is often individualized by the endoscopic and oral/maxillofacial surgeons depending upon situations.18,19 An overdose during the greater palatine canal block could theoretically lead to vasospasm of vasa vasorum of the oculomotor nerve branches, resulting in ONP.
But, in the context of our patient, there are several points against this speculation. First, the nerve paresis resulting from the local anesthesia-vasoconstrictor premix overdose would not be severe enough to be complete. Second, it is difficult to explain a protracted recovery when the oculomotor nerve is so affected. Third, such an injury should be pupil-sparing. The vasa vasorum of the oculomotor nerve supplies its core, which contains the motor fibers to the extraocular muscles, whereas the fibers supplying the pupil (the pupillomotor fibers) are at its periphery and are supplied independently by the pial blood vessels. 16 Therefore, an ischemic change due to vasospasm of the vasa vasorum would spare the pupil. Fourth, our patient did not complain of hypo-esthesia of the maxillary region (lower face), suggesting sparing of the maxillary division of the trigeminal nerve – the integral content of the infraorbital fissure through which the pterygopalatine fossa communicates to the orbit.
Therefore, it is more logical to accept that there might have been an inadvertent microtrauma during the EES that was not identified at surgery and not detected by the immediate postoperative imaging. Because of its subtle nature, the surgical team could not recollect any event that could have caused an injury to the orbital confines, primarily the floor, which was anyway removed at its medial third. The present experience calls for a cautious approach by the endoscopic surgeons during procedures that involve manipulation with the orbital floor, like endoscopic modified Denker’s approach for medial maxillectomy, total maxillectomy, exploration and repair of orbital floor fracture, and the surgical approaches involving the pterygopalatine fossa. Also, dissection in the ethmoid sinuses close to the lamina papyracea should be carried out meticulously so as to prevent injury to the medial wall of the orbit. Finally, when encountered with such an unexpected and unusual complication of a known, often-performed procedure, the introspection by the surgical team that has an important role to play should be astutely impartial, critical, and honest enough to override self-denial.
Conclusions
ONP is an extremely-rare complication following EES that causes significant apprehension to both the patient and the surgical team. Inadvertent iatrogenic trauma and extrinsic compression by impinged bone fragment, along with the theoretical propositions of perineural edema, compression by anterior nasal packs, and effect of local anesthetic-vasoconstrictor premix have been put forward in the literature as the probable etiologies. ONP due to trauma or extrinsic compression generally involve the pupil; a fixed or sluggish pupillary movement along with ptosis and ophthalmoplegia might differentiate a trauma-induced ONP from an atraumatic one. EES that involves manipulation of the orbital floor and the medial orbital wall at the level of the ethmoids and sphenoid sinus should be executed with utmost finesse and caution. ONP post-EES mandates an imaging at the earliest. Management in almost all instances is observation, removal of the nasal packs, and systemic steroid, unless an emergency exploration is needed for a radiologically-evident extrinsic compression on the nerve or orbital walls. Our report illustrates the approach to a patient with ONP post-EES, and how to analyze the etiology – an exercise that adds to our experience and learning curve as endoscopic sinus/skull-base surgeons.
Footnotes
Ethical Considerations
Written informed consent has been obtained from the patient to publish this clinical report. The clinical and surgical principles adopted for the management of his condition complied with the ethical standards of relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1975, as revised in 2013, at Fortaleza, Brazil.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The clinical data of the patient illustrated in this article are available from the authors and can be reproduced on request.