
Abstract
Pupil-sparing third-nerve palsy is often attributed to diabetic microvascular ischemia; however, brainstem infarction can present with a similar pattern. We report the case of a patient with acute painless horizontal diplopia and partial right oculomotor palsy characterized by impaired adduction, mild vertical limitation, partial ptosis, and mildly impaired convergence, with equally reactive pupils. On left gaze, the right eye failed to adduct and the contralateral eye did not demonstrate abducting nystagmus. Brain magnetic resonance imaging revealed a small dorsal paramedian midbrain infarction on diffusion-weighted imaging, and diffusion-tensor tractography demonstrated reduced integrity of the ipsilateral medial longitudinal fasciculus. The patient received dual antiplatelet therapy for 21 days, followed by aspirin, high-intensity statin therapy, and intensive glycemic control. Diplopia resolved within 4 weeks and remained absent at the 3-month follow-up. This case broadens the clinico-radiological spectrum of midbrain infarction and underscores that pupil-sparing third-nerve palsy does not exclude a central lesion. The combination of adduction deficit, impaired convergence, and absent contralateral abducting nystagmus should lower the threshold for urgent brain magnetic resonance imaging with diffusion-weighted imaging; diffusion-tensor tractography may be helpful where available.
Keywords
Introduction
Partial oculomotor palsy characterized predominantly by medial rectus dysfunction is exceedingly rare in the context of midbrain infarction, with only a few cases reported.1–7
Previous literature has generally attributed medial rectus palsy either to midbrain infarction involving the oculomotor nucleus or fascicles1–3,5–11 or to isolated lesions of the medial longitudinal fasciculus (MLF). 4 However, atypical overlapping presentations—where both the oculomotor nuclear or fascicular fibers and the MLF are simultaneously affected, without the classic sign of contralateral abducting nystagmus—remain underrecognized. Such patterns are at risk of being misdiagnosed as diabetic microvascular ophthalmoplegia, potentially delaying appropriate recognition and secondary prevention of central causes.2,12–14
Here, we present a patient with partial oculomotor palsy dominated by medial rectus involvement, preserved pupillary function, and concomitant ipsilateral MLF damage in the absence of contralateral abducting nystagmus. The etiology was confirmed as midbrain infarction. This case challenges the long-standing “rule of the pupil,” which posits that pupil-sparing oculomotor palsy is typically of microvascular origin, underscoring the need for advanced neuroimaging in atypical presentations.
Case report
A man in his late 50s awoke with an acute onset of painless horizontal diplopia (Figure 1) that resolved when either eye was covered. He denied headache, periocular pain, vertigo, limb weakness, or sensory disturbance. His medical history was unremarkable, and he was not taking any regular medications. Family history was negative for neurological disorders or hereditary conditions, and his psychosocial history revealed no significant stressors or relevant genetic information. The patient was admitted to The Affiliated Changsha Central Hospital, Hengyang Medical School, University of South China, Yuhua District, Changsha, China, in mid-2024. Signed consent to treatment was obtained from the patient. The reporting of this study conforms to the Case Report (CARE) guidelines. 15 All patient details have been de-identified.

Diplopia charting showing uncrossed diplopia. Red indicates the view from the right eye; blue indicates the view from the left eye.
Examination
Vital signs were stable (temperature: 36.5°C, blood pressure: 141/91 mmHg, pulse: 72/min, and respiratory rate: 20/min). Neurological examination revealed partial right oculomotor nerve palsy. Specifically, adduction of the right eye was impaired in all positions of gaze (Figure 2; Supplementary Video 1), accompanied by mild limitation of supraduction and infraduction, partial ptosis, and a “down-and-out” position of the right eye in primary gaze. Convergence was mildly impaired, with incomplete near-point adduction observed clinically. Notably, during leftward gaze, the left eye abducted fully without abducting nystagmus. Both pupils were equal in size (3 mm) and briskly reactive. No other focal neurological deficits were detected, and the National Institutes of Health (NIH) Stroke Scale score was 1.

Eye position during neurological examination, demonstrating partial oculomotor nerve palsy with impaired adduction, mild restriction in supraduction and infraduction, and partial ptosis of the right eye. (a) Upward gaze (mild restriction in supraduction). (b) Rightward gaze. (c) Primary (central) gaze (right eye positioned down and out with partial ptosis). (d) Leftward gaze (impaired adduction) and (e) downward gaze (mild restriction in infraduction).
Laboratory findings
Glycated hemoglobin (HbA1c) level was 7.7% (reference, 4.0%–6.0%); fasting glucose, 8.34 mmol/L (reference, 3.89–6.11 mmol/L); triglycerides, 8.37 mmol/L (<1.7 mmol/L); and total cholesterol, 6.14 mmol/L (3.4–5.2 mmol/L). Full blood count and renal, hepatic, electrolyte, and thyroid function tests were within normal limits.
Timeline
Key clinical events are summarized in Figure 3.

CARE timeline of the patient’s episode of care. CARE: Case Report.
Diagnostic assessment, intervention, and outcomes
Neuroimaging
High-resolution magnetic resonance imaging (MRI) (3.0 T) revealed a small hyperintense lesion in the right dorsal paramedian midbrain on diffusion-weighted imaging (DWI), with corresponding hypointensity on the apparent diffusion coefficient (ADC) map (representative ADC value: 0.45 × 10−³ mm2/s). No hemorrhage was detected on susceptibility-weighted imaging. Three-dimensional time-of-flight magnetic resonance angiography (MRA) showed no aneurysm or stenosis. Diffusion-tensor imaging (DTI) with deterministic tractography demonstrated reduced fiber integrity in the ipsilateral MLF (fractional anisotropy (FA) value: 0.32) (Figure 4), consistent with combined nuclear or fascicular and tract involvement.
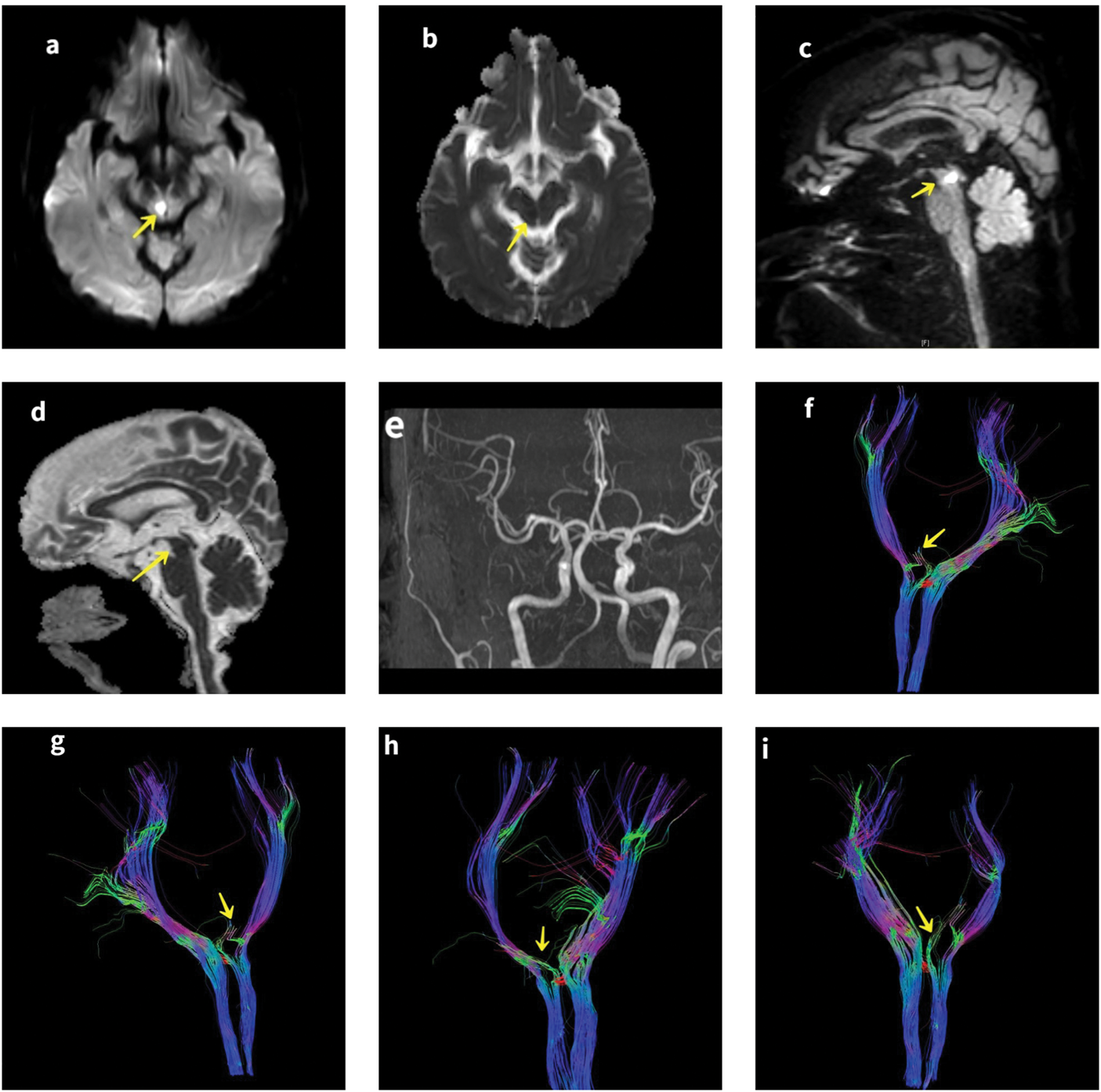
Brain MRI demonstrating a small acute infarct in the dorsal paramedian midbrain. Axial DWI (a) and ADC map (b) showed the lesion. Sagittal DWI (c) and ADC (d) further delineated the lesion (yellow arrows). MRA (e) showed no vascular abnormalities. DTI images (f–i) revealed reduced fiber integrity of the right MLF (yellow arrows), with bilateral structures presented for reference. MRI: magnetic resonance imaging; ADC: apparent diffusion coefficient; DTI: diffusion-tensor imaging; DWI: diffusion-weighted imaging; MLF: medial longitudinal fasciculus; MRA: magnetic resonance angiography.
Differential diagnosis
No significant diagnostic challenges were encountered, such as limited access to testing, financial barriers, or cultural factors, as the patient was promptly evaluated in a tertiary care setting. The main differential diagnoses considered were diabetic microvascular third-nerve palsy, internuclear ophthalmoplegia (INO), demyelinating disease, and compressive lesions such as aneurysm or tumor. Because pupil-sparing ophthalmoplegia involving multiple extraocular muscles can occur in both central and peripheral etiologies, neuroimaging was essential to establish the diagnosis. Brain MRI confirmed a small ischemic infarct in the dorsal paramedian midbrain, establishing the etiology as brainstem stroke.
Treatment and outcome
The patient was treated with dual antiplatelet therapy (100 mg aspirin plus 75 mg clopidogrel daily for 21 days, followed by 100 mg aspirin monotherapy), atorvastatin (40 mg daily), and intensive glycemic control using a basal–bolus insulin regimen combined with dietary modification. Thrombolysis was not administered due to delayed presentation. Diplopia improved within 14 days and resolved completely by 28 days. At 3 months, he remained symptom-free, with HbA1c level improving to 6.4% and fasting glucose to 6.1 mmol/L. Follow-up assessments were conducted at 14 days, 28 days, and 3 months. No adverse or unanticipated events occurred during treatment or follow-up. The prognosis was favorable given the small lesion size and prompt intervention, with a low risk of recurrence under secondary prevention. Intervention adherence was assessed via patient self-report and follow-up visits, showing good tolerability and no reported side effects.
Discussion
This case illustrates a rare clinico-radiological phenotype of midbrain infarction, characterized by partial oculomotor palsy with medial rectus predominance, preserved pupillary function, and ipsilateral MLF involvement without contralateral abducting nystagmus. Although the clinical features—such as adduction deficit, absent contralateral abducting nystagmus, and mild convergence impairment—can be explained by infarction of the right medial rectus subnucleus, DTI demonstrated concomitant MLF damage, resulting in an overlapping phenotype. Such an overlap of oculomotor nuclear or fascicular and MLF damage is scarcely documented. Most previously reported cases fall into two categories: (a) midbrain infarction involving the oculomotor nucleus or fascicles, typically presenting as isolated medial rectus weakness and (b) isolated MLF infarction, presenting as INO with impaired adduction, often accompanied by abducting nystagmus.1–11
The present case demonstrates overlapping features of both categories, thereby extending the clinico-radiological spectrum of midbrain infarction. Anatomical correlation supports this observation: the medial rectus subnucleus is located ventrally within the oculomotor nuclear complex, whereas the MLF lies dorsally.16,17 A small dorsal paramedian infarct can therefore involve both structures simultaneously.7,18 This anatomical proximity explains the coexistence of adduction deficit and impaired convergence, reflecting nuclear or fascicular involvement, alongside MLF disruption.
The pathophysiological basis of INO lies in damage to the MLF, 19 a heavily myelinated nerve tract that connects the ipsilateral oculomotor nucleus (cranial nerve (CN) III) with the paramedian pontine reticular formation (PPRF) and the contralateral abducens nucleus (CN VI) in the pons. 16 It is situated in the dorsomedial brainstem tegmentum, encompassing the midbrain and pons, ventral to the cerebral aqueduct or fourth ventricle, and lies in close proximity to the midline. 17 This structure comprises both ascending and descending fibers distributed within the brainstem tegmentum. It is intimately linked to the oculomotor control network and contributes to the coordination and synchronization of eye movements in horizontal, vertical, and torsional directions. 20
First, adduction weakness arises from interruption of axons from interneurons in the abducens nucleus, which project via the MLF to the contralateral medial rectus subnucleus of the oculomotor nucleus. 16 Second, the mechanism of abducting nystagmus involves a compensatory process: to overcome ipsilateral adduction weakness, the nervous system augments innervation to the adducting eye. 21 In accordance with Hering’s law of equal innervation, this augmentation synchronously affects the contralateral abducting eye, resulting in increased yoked innervation. 21 Although this may partially ameliorate adduction in the affected eye, it induces abnormal saccadic movements in the other eye, including abducting overshoot followed by backward post-saccadic drift, clinically manifesting as abducting nystagmus. 21
Consequently, damage to the MLF results in an inability to perform conjugate lateral gaze and ophthalmoplegia, clinically manifesting as weakness of adduction in the ipsilateral eye, which may be accompanied by monocular jerk-type abducting nystagmus in the contralateral eye during horizontal gaze.22,23 During convergence attempts, adduction function may be preserved or absent. 24 Furthermore, identification of occult or mild variants of INO can be challenging, potentially presenting solely as mild adduction weakness without abducting nystagmus. 25 This may arise from mild MLF damage, resulting in an adduction deficit insufficient to trigger a significant compensatory mechanism. Conversely, the absence of abducting nystagmus may stem from failure to activate its multifactorial etiology. 22 Abducting nystagmus is not solely attributable to Hering’s law but may also involve superimposed gaze-evoked nystagmus or adaptive adjustments to adduction weakness. 26 If the lesion spares adjacent structures, such as the vestibular nuclei, or if adaptive mechanisms are not sufficiently engaged, nystagmus may not manifest. 27 In most INO patients, orthotropia is maintained in the primary gaze position despite evident medial rectus dysfunction, although the underlying physiological mechanism remains to be fully elucidated. 24
Convergence movements pertain to the near response system, with ascending pathways bypassing the MLF and directly transmitting signals to the medial rectus subnucleus via higher centers such as the mesencephalic reticular formation (MRF) and pontine reticular structures, including the nucleus reticularis tegmenti pontis (NRTP).22,24 Consequently, in most INO cases, convergence remains preserved despite adduction deficits during horizontal gaze, a phenomenon termed dissociation of convergence. The underlying mechanism is that the convergence pathways in INO, including fibers originating from the oculomotor medial rectus subnucleus, are spared.22,28 However, the absence of convergence does not preclude a diagnosis of INO. According to Cogan’s classification, anterior INO occurs at the midbrain level, near the oculomotor nucleus, where lesions may extend to convergence-related ascending fibers or prenuclear structures, thereby interrupting convergence signals and leading to convergence impairment. Posterior INO is localized to the pontine level, confined to the caudal MLF segment, where convergence pathways are relatively independent and typically preserve convergence function.24,29 Moreover, variability in convergence is influenced by factors such as the patient’s subjective convergence effort and the extent of involvement of the NRTP or medial rectus subnucleus.4,25,30 In bilateral INO or wall-eyed bilateral INO (WEBINO), lesions affecting the NRTP or midbrain medial rectus subnucleus disrupt convergence signal transmission, commonly resulting in the absence of convergence. This mechanism accounts for the observed clinical variability: convergence is often preserved in mild or unilateral INO, whereas it is more frequently impaired in bilateral or dorsal midbrain lesions. 30
In this case, convergence was mildly impaired, suggesting partial nuclear involvement. However, DTI findings of reduced MLF integrity (FA: 0.32) support an overlapping phenotype rather than isolated medial rectus palsy.
Although an isolated medial rectus subnuclear infarct could explain some features, DTI-confirmed MLF involvement indicates an overlapping phenotype, differentiating it from pure nuclear lesions. Similarly, pupil sparing in this dorsal paramedian lesion can be attributed to the precise topography, sparing the more central Edinger–Westphal (EW) nucleus due to its rostral–dorsal position and potential collateral perfusion,26,31–33 as reported in similar cases.26,34,35
Clinically, this case underscores the limitations of relying exclusively on the “rule of the pupil.” Although it is traditionally considered a reliable marker distinguishing microvascular from central etiologies, pupil sparing does not exclude brainstem infarction. Therefore, advanced MRI techniques, including DWI and DTI, are critical for accurate diagnosis in atypical presentations. 36 A summary of the reported cases (Table 1) highlights these variations in presentation and supports the need for such imaging. For instance, Yan et al. 4 provided a model for differentiating isolated MLF infarction (with intact convergence) from partial oculomotor palsy using convergence assessment, primary gaze evaluation, and DTI.
Summary and classification of reported cases of midbrain infarction presenting with adduction deficit and pupil sparing.
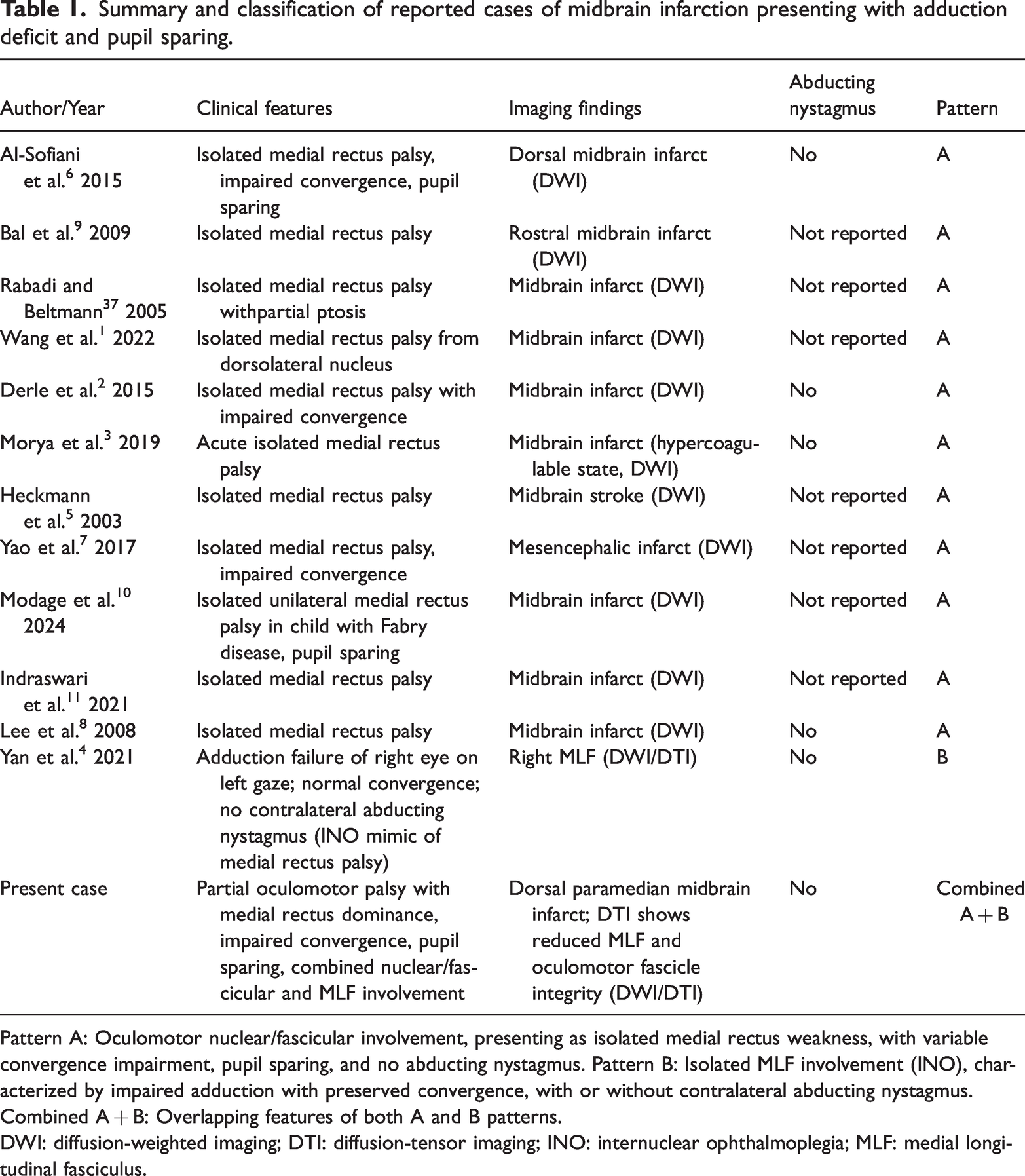
Pattern A: Oculomotor nuclear/fascicular involvement, presenting as isolated medial rectus weakness, with variable convergence impairment, pupil sparing, and no abducting nystagmus. Pattern B: Isolated MLF involvement (INO), characterized by impaired adduction with preserved convergence, with or without contralateral abducting nystagmus. Combined A + B: Overlapping features of both A and B patterns.
DWI: diffusion-weighted imaging; DTI: diffusion-tensor imaging; INO: internuclear ophthalmoplegia; MLF: medial longitudinal fasciculus.
This report has a key strength and several limitations. The strength lies in the use of advanced DTI for precise anatomical correlation. The main limitation of this report is its single-case nature, which precludes generalization. Additionally, due to the absence of video or photographic documentation of convergence testing, the degree of impairment relies on clinical observation, which may introduce subjectivity. Nonetheless, this case enriches the diagnostic spectrum of midbrain infarction and highlights the clinical value of combining conventional examination with advanced neuroimaging.
Patient perspective
“I was frightened by the onset of double vision but relieved to learn it was a treatable small stroke. The MRI images helped me understand the issue. My vision returned within weeks, and I now monitor my blood sugar and adhere to medications to prevent recurrence.”
Conclusion
In summary, pupil-sparing oculomotor palsy should not be automatically attributed to microvascular ischemia. When atypical features such as convergence impairment or INO-like signs are present, clinicians should promptly perform advanced MRI, including DWI and DTI, to identify central lesions and initiate secondary stroke prevention.
Supplemental Material
sj-mp4-1-imr-10.1177_03000605251405100 - Supplemental material for Pupil-sparing partial oculomotor palsy with ipsilateral medial longitudinal fasciculus involvement: A novel midbrain infarct phenotype–a case report
Supplemental material, sj-mp4-1-imr-10.1177_03000605251405100 for Pupil-sparing partial oculomotor palsy with ipsilateral medial longitudinal fasciculus involvement: A novel midbrain infarct phenotype–a case report by Li-Chao Zhou, Qiong Wu, Yu-Jing Liu, Wei Xu, Tie-Qiao Feng, Zhen Wang, Fang-Yi Li and Wen-Gao Zeng in Journal of International Medical Research
Footnotes
Acknowledgments
Generative artificial intelligence (AI) tools were used to assist with language improvement in the manuscript. No other AI tools were employed.
Author contributions
Li-Chao Zhou: data curation; Qiong Wu: data curation, writing—original draft, investigation; Yu-Jing Liu: data curation; Wei Xu: investigation, methodology, data curation; Tie-Qiao Feng: investigation, methodology; Zhen Wang: supervision; Fang-Yi Li: supervision; Wen-gao Zeng: supervision, writing—review & editing.
Consent
Written informed consent was obtained from the patient in accordance with institutional policy and the Declaration of Helsinki, covering both participation and publication (text, images, and video).
Data availability
De-identified data are available upon reasonable request.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Ethics
In accordance with local regulations, case reports do not require approval from an ethics committee. However, an institutional review board waiver was obtained from the Medical Ethics Committee of Changsha Central Hospital, Yuhua District, Changsha, China (Waiver No. 20250305, Date: 1 March 2025).
Funding
The study did not receive any specific funding from public, commercial, or not-for-profit agencies.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.