
Abstract
Objectives:
To investigate the outcomes of graft uptake and hearing results in the repair of anterior perforation via a total endoscopic transcanal approach using a single or double perichondrium reinforced cartilage underlay technique.
Study Design:
Retrospective study.
Setting:
Tertiary referral hospital.
Materials and Methods:
We analyzed 65 patients who underwent surgery for anterior perforation. All surgeries were done via an endoscopic transcanal approach using tragal cartilage as graft, underlay technique reinforced with single or double perichondrium. Two groups were created in which group A had single perichondrium reinforcement and group B had double perichondrium. Graft uptake and hearing outcomes were evaluated between the two groups.
Results:
During the study period, 65 patients were included, of which 3 were lost to follow-up, and thus, only 62 patients were assessed. As for the surgical outcome, graft uptake was observed in 95.2% (n = 59) of patients, 6 months after the intervention. Graft uptake was not statistically significantly different between groups A and B and was 95% in both. There was a statistically significant improvement in hearing across the series overall, with no significant differences seen between group A and group B.
Conclusions:
The endoscopic approach for myringoplasty offers superior visualization, especially for anterior perforation avoiding postaural approach and canaloplasty. Endoscopic single or double perichondrium reinforced cartilage underlay technique is a reliable method for repair of anterior perforation. There is no difference in using single or double perichondrium reinforcement. Thus, we recommend using single or double perichondrium reinforcement depending on the need during the surgery.
Introduction
Myringoplasty is one of the common surgical procedures done by otologists to repair tympanic membrane (TM) perforations and restore hearing. 1 It can be done in 2 classical ways, including underlay (medial) and overlay (lateral) techniques.
In the underlay technique, the graft is placed medial to the TM remnant and malleus handle and is more suitable for posterior perforations. It is more commonly used worldwide, easier to perform, and less time consuming. However, disadvantages include decreased mesotympanic space, medialization of graft, and less success rate for anterior perforation. 2 The modifications of underlay tympanoplasty for repairing anterior perforations of the TM include mediolateral graft, window shade, anterior transcanal, loop overlay, and hammock techniques. 3
In the overlay technique, the epithelial layer is elevated precisely, and the graft is placed lateral to the fibrous layer of TM remnant and annulus. Although this technique has a higher success rate, it is technically demanding and has specific complications such as graft lateralization, anterior blunting, slow healing, stenosis of the external auditory canal (EAC), and iatrogenic cholesteatoma. 4
Temporalis fascia has been largely and commonly used as graft material; however, it has been recently replaced by cartilage, especially for anterior and subtotal perforation because of stability and long-term uptake result. 5 The complete closure of a TM perforation also depends on its location, besides the graft and the techniques used. 6 The repair of an anterior or subtotal perforation is associated with a lower success rate than that of posterior or inferior perforations. 4 The reasons for lower success rate in the closure of anterior TM perforation are insufficient visualization, technically challenging procedure, decreased graft viability due to poor vascularization, inadequate anterior membrane remnant, and poor stabilization. 7
Microscopy has been considered to be the gold standard for ear surgery; however, due to its straight-line vision, it limits the exposure of anterior quadrant or marginal perforations. 8 To overcome this, more invasive procedures that enlarge the surgical field are needed, such as canaloplasty or a postaural approach. 9 Because of these limitations, the use of an endoscope is rapidly increasing in the past 2 decades. The main advantage of endoscopes in myringoplasty is its wider field of view, superior visualization, including anterior margins avoiding postaural approach and canaloplasty. 10
When barred cartilage was used as a graft for the closure of perforation using the underlay technique, we noted a gap between the cartilage and the anterior remnant TM or annulus. This was because of the rigidity of the cartilage. So, we reinforced the bared cartilage with perichondrium to ensure the touch of the graft with the annulus. Even with a single perichondrium, there were still cases with a gap or a distance between graft and remnant of TM/annulus. So, to ensure there was a proper touch between the graft and the annulus of TM, the second perichondrium was also used only if the surgeon felt the need. Double perichondrium use was purely based on clinical judgments. The endoscope provided the advantage of a wide-angle view, and all the margins of perforations would easily be seen. Thus, the main aim of this study was to evaluate the morphological and functional outcomes of total endoscopic cartilage tympanoplasty with single or double perichondrium reinforcement and also to see whether the clinical judgment was justified or not.
Materials and Methods
This is a retrospective study. We analyzed 65 patients who underwent surgery for chronic otitis media with anterior perforation in our hospital from February 2016 to September 2018. Of the 65 cases, 3 patients were lost to follow-up; thus, only 62 patients were enrolled for the study.
The patients with TM perforation involving anterior quadrant requiring primary or revision surgery with a minimum of 6 months follow-up period were included. Patients having cholesteatoma, retraction pockets, atelectasis, active infection, and those involving posterior perforation were excluded from the study.
The surgeries were performed under general anesthesia in patients younger than 13 years and under local anesthesia in patients older than 13 years. Cases done under local anesthesia were performed as a day case basis without admission. Ethical clearance was obtained from the institutional review board for the study.
Instruments
All procedures were performed by a transcanal approach using a high-definition monitor and camera head manufactured by Stryker together with zero degrees, 4-mm rigid endoscope of 18 cm length.
Surgical Procedure
Tragal cartilage was used as a graft in all cases. It was harvested and perichondrium was removed on both sides (Figures 1 and 2). The margin of perforation was freshened. Two vertical incisions were given at 12 o’clock and 5 o’clock, which was connected with a horizontal incision about 10 mm lateral to the annulus. Tympanomeatal flap was elevated from the posterior canal wall. The posterior annulus was elevated out of the sulcus, and the mobility of the ossicular chain was checked.
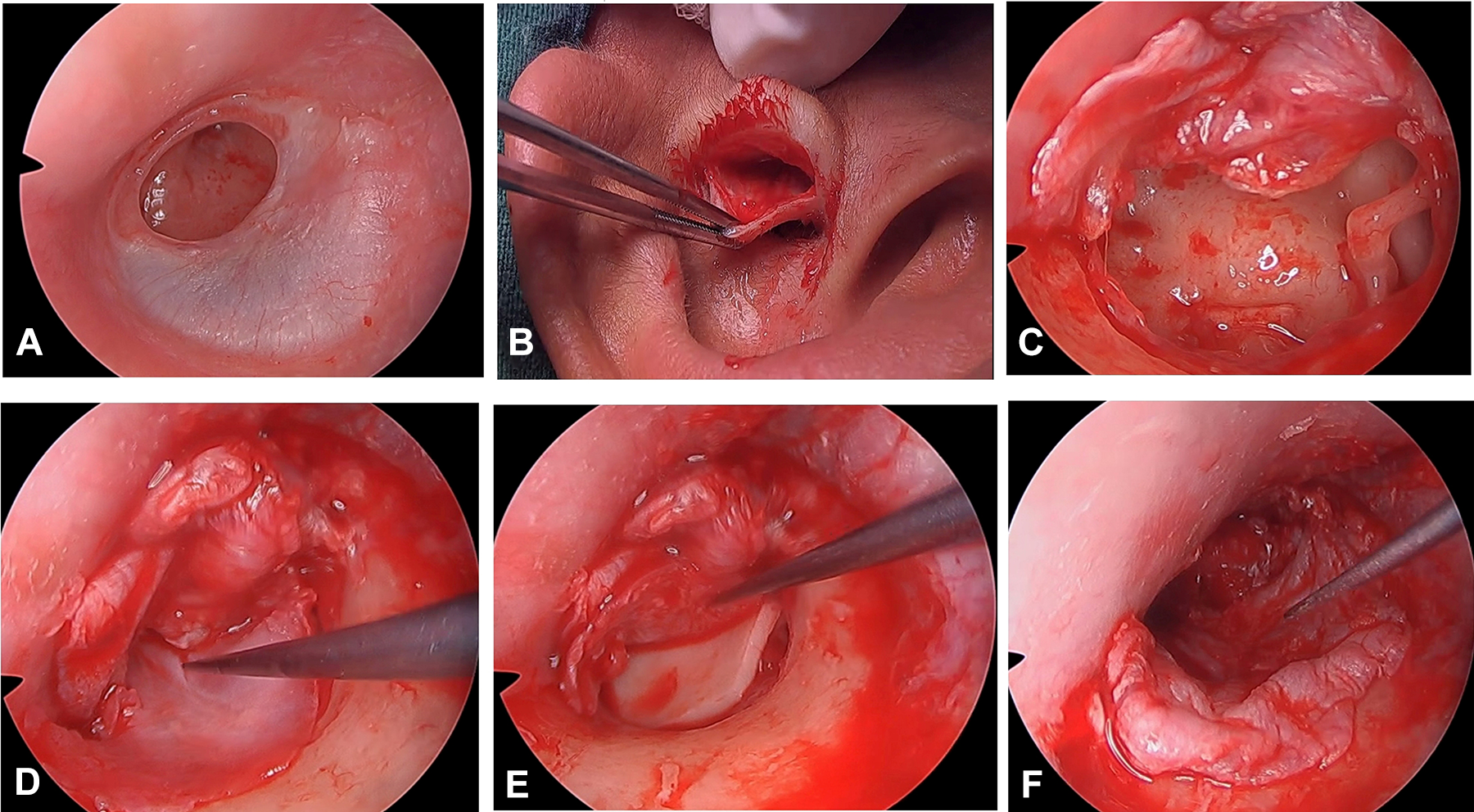
A, Preoperative perforation. B, Tragal cartilage graft harvested. C, Middle ear and ossicles exposed after the elevation of tympanomeatal flap. D, First perichondrium placed under the handle of malleus. E, Barred cartilage placed under the elevated first perichondrium. F, Tympanomeatal flap placed back to posterior canal.
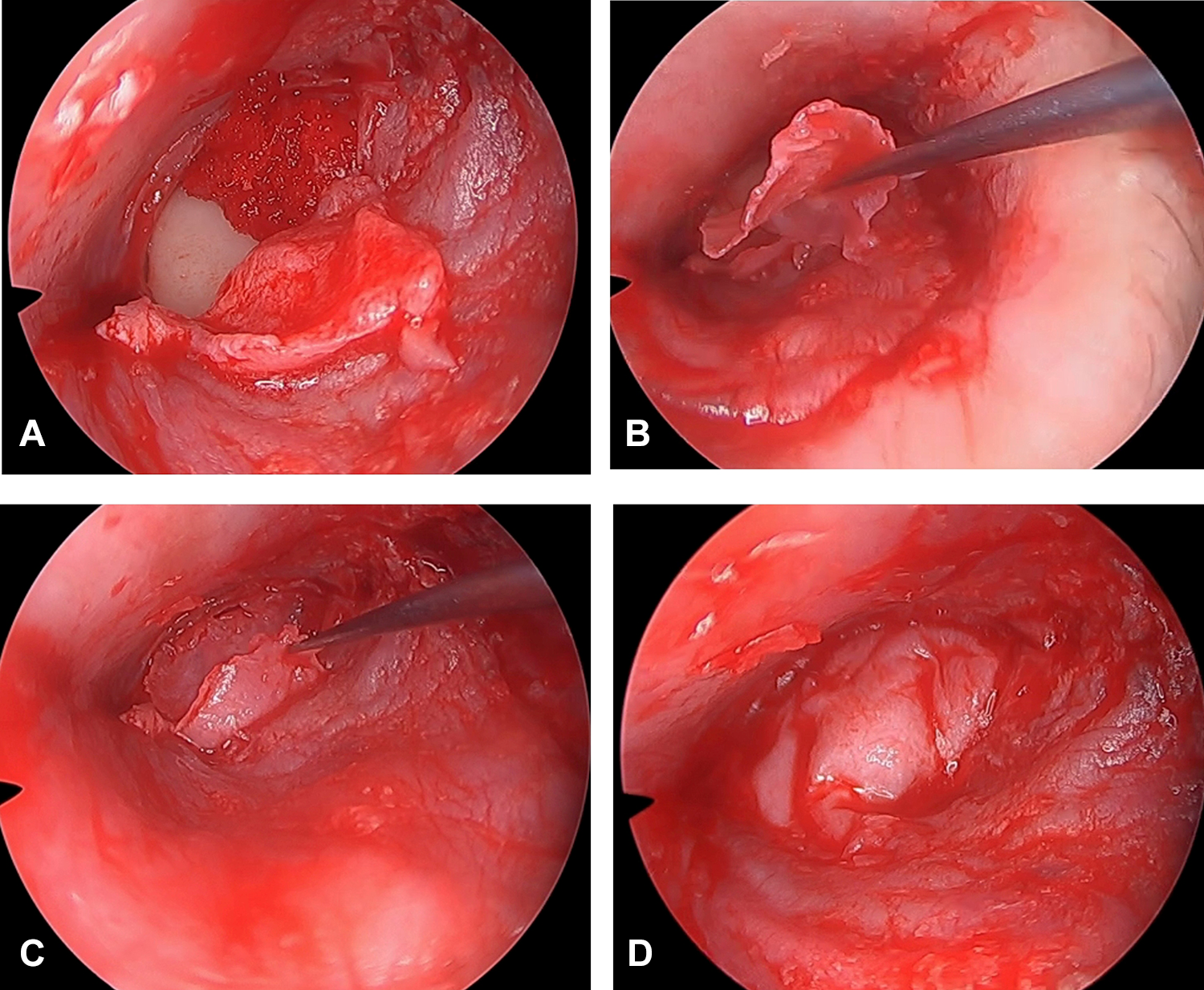
A, First perichondrium reflected laterally to expose barred cartilage. B, Second perichondrium placed over barred cartilage under anterior annulus. C, First perichondrium placed over the second perichondrium and under annulus. D, Final position of graft ensuring all under the margin and anterior annulus.
Gelfoams (SPONGOSTAN Special, Ferrosan Medical Devices A/S) were kept in the middle ear accordingly. At first, the perichondrium graft was placed using the underlay technique under the handle of malleus and pushed anteriorly up to anterior margin. The perichondrium layer was then lifted again. The barred cartilage shaped according to the size needed was negotiated under the malleus handle (underlay technique). If the middle ear space was compromised due to a medialized handle of malleus, the cartilage was notched to fit the handle of malleus. Previously lifted perichondrium was also placed back over the barred cartilage. The tympanomeatal flap was placed back in the posterior canal wall. The perichondrium was adjusted to fit and tug around the margin of perforation. A final check was done to ensure there was a touch of first perichondrium graft with anterior margin and annulus. If the surgeon finds the graft is well tugged around the margin, then the surgery is completed, and this comprised of group A cases, that is, single perichondrium reinforcement.
In cases that seemed to have a gap between the graft and the anterior margin, the first perichondrium was lifted and reflected laterally from the anterior margin, while its posterior part was still under the posterior margin of perforation. Extra second perichondrium was reinforced over the barred cartilage and under the anterior annulus. Then, the previously reflected first perichondrium was positioned back to anterior margin to ensure all the margin of perforation was in touch with the graft, and this comprised of group B cases, that is, double perichondrium reinforced (Figures 1–3).

Graft uptake at 6 months follow-up.
Thus, the 2 groups were created in this study. In group A, a single perichondrium was enforced over the barred cartilage, and in group B, double perichondrium was used.
The EAC was packed with gelfoam and then with ear pack (Osseous Ear Pack, Eon Meditech Pvt Ltd), which was removed after 7 days. No suture was applied in the graft site.
Patients were followed up at 6 weeks, 12 weeks, and 6 months. The average on 4 frequencies (0.5, 1, 2, and 3 kHz) of hearing thresholds in air and bone conduction and the air-bone gap (ABG) was evaluated 7 days before surgery and 12 weeks after.
Statistical Tools
Data were analyzed as graft uptake rate and as change between pre- and postoperative hearing. Data were analyzed using the Fisher exact test, and the dependent and independent t test in IBM SPSS Statistics for Windows, version 23.0 (IBM Corp). The level of statistical significance was set at P < .05.
Results
During the study period, 65 patients were included, of which 3 were lost to follow-up; thus, only 62 patients were assessed. The demographic profile between the 2 groups is shown in Table 1. There were 2 groups created depending on single or double perichondrium used. In group A, a single perichondrium was enforced over the barred cartilage, and in group B, double perichondrium was used. Group A comprised of 21 patients and group B had 41 patients. The overall mean age of patients was 29.24 ± 10.38, and the age ranged from 12 to 57 years old. The mean age was 29.14 ± 10.25 in group A and 29.29 ± 10.56 in group B which was statistically not significant (P = .92). There were 10 males and 11 females in group A whereas 25 males and 16 females in group B, and the difference was not statistically significant (P =.418). Regarding the laterality of the disease, 10 cases involved left ear and 11 cases involved right ear in group A, and 18 cases had the disease in the left ear and 23 cases in the right ear in group B. The difference was also not statistically significant (P = .798). Most patients were undergoing surgery for the first time; patients undergoing revision surgery accounted for 3.2% of cases (n = 2).
Distribution of Enrolled Patients.a
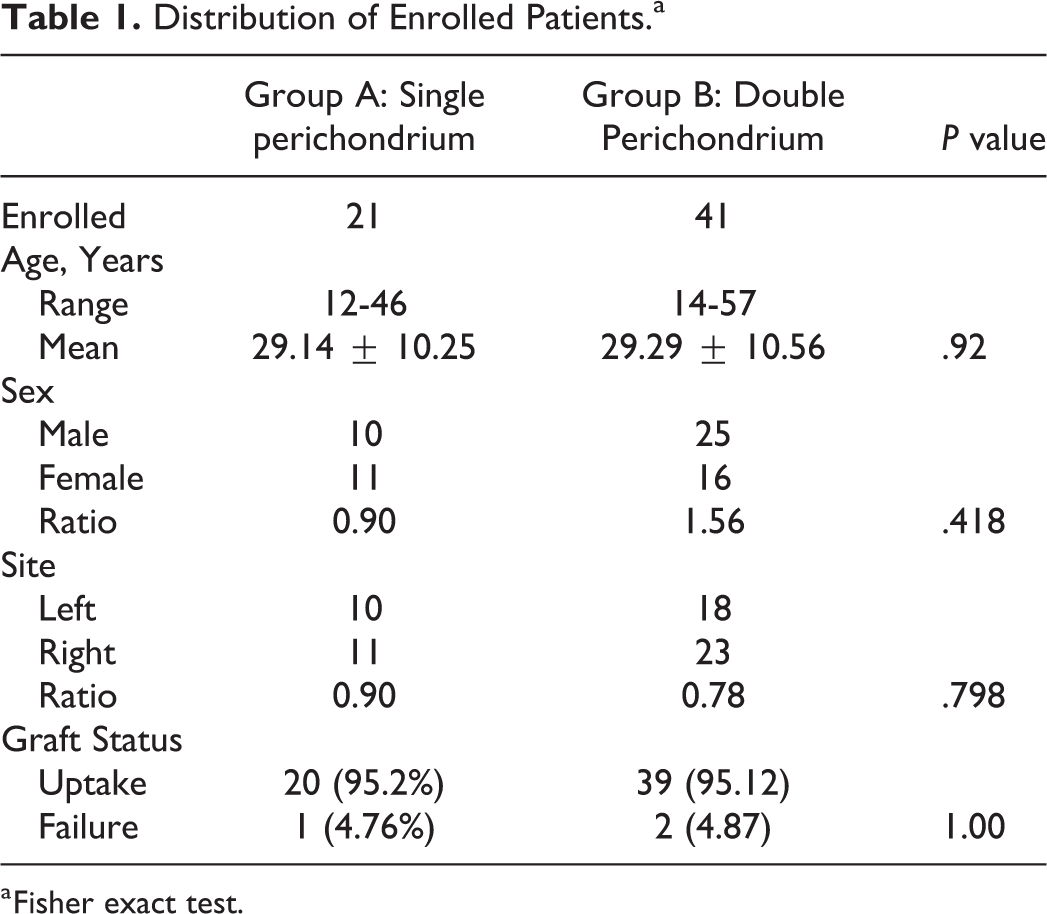
a Fisher exact test.
Surgical Outcome
As for the surgical outcome, graft failure was seen in 3 cases in which 1 case had initial uptake at 3 months but later failed (Table 1). Thus, complete closure of the perforation was observed in 59 cases (95.3%) 6 months after the intervention.
Out of a total of 21 cases in group A, graft uptake was seen in 20 (95.2%) cases, and out of 41 cases in group B, graft uptake was in 39 (95.1%) cases. The results were not statistically significantly different in both the groups (P = 1.00).
There were no cases that required surgical conversion to the retroauricular approach or use of the microscope in this series. There were no postoperative complications.
Postoperative Hearing
Audiometrically, an improvement in the pure tone average hearing thresholds was observed from the preoperative to the postoperative period (Tables 2 and 3). All the patients had intact ossicular chain mobility. The preoperative air conduction threshold (ACT) and the ABG was 40.83 ± 12.06 and 23.20 ± 8.79, respectively. Postoperatively ACT and ABG closure were 25.56 ± 9.23 and 11.10 ± 6.08, respectively.
Pre- and Postoperative Hearing Outcome.
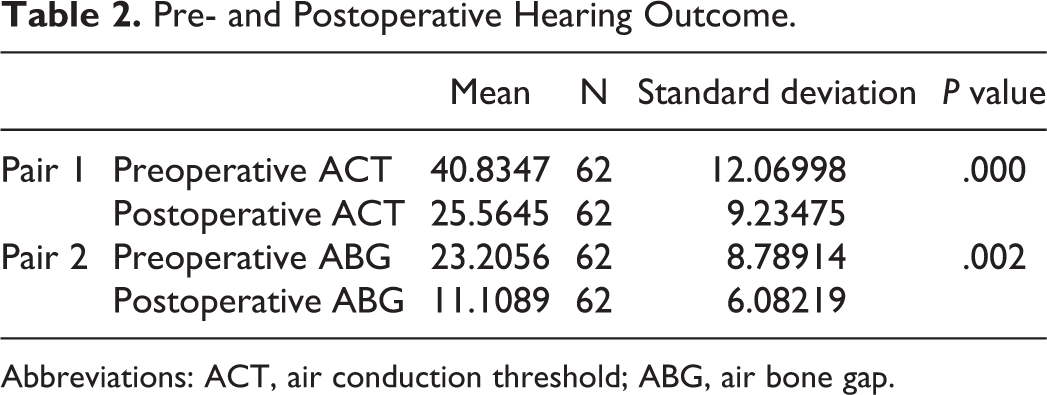
Abbreviations: ACT, air conduction threshold; ABG, air bone gap.
Pre and Postoperative Hearing Outcomes Between Groups A and B.
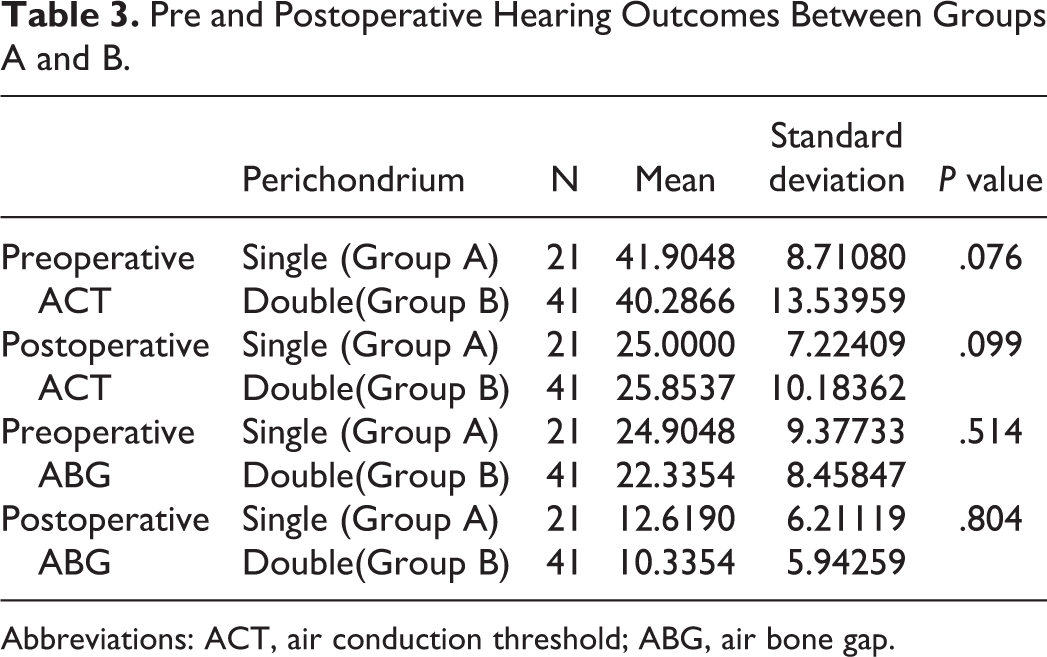
Abbreviations: ACT, air conduction threshold; ABG, air bone gap.
This difference was statistically significant (P < .001; Table 2). Similarly, hearing outcomes between groups A and B were as shown in Table 3. There was a statistically significant improvement in hearing postoperatively within the group and no significant difference seen between the groups. Thus, double perichondrium did not hamper in hearing outcome.
Discussion
Microscopes have been widely used for the otological procedures, including myringoplasty. It provides advantages of stereoscopic vision, better depth perception, and bimanual handling. 11 But it has disadvantages of giving straight-line vision, limiting exposure of anterior quadrant or marginal perforation, especially if the canal is narrow or has a prominent anterior canal wall. 12 This makes surgery difficult and might require a postaural approach and canaloplasty.
Anterior perforations are also difficult to handle due to its difficult access, reduced vascularity, and graft instability leading to residual perforations. All these factors affect the outcome, making it a surgical challenge. 13
Because of these limitations of the microscope, the use of an endoscope is rapidly increasing in the past 2 decades. The main advantage of endoscopes in myringoplasty is its wider field of view, superior visualization, including anterior margins avoiding postaural approach, and canaloplasty. 10 The first reported case of endoscopic myringoplasty was by el-Guindy in 1992. 14
Although temporalis fascia is still being used as graft material, it has been largely replaced by cartilage, especially in conditions as anterior perforation because of its stability and long-term uptake result. 9 In our study, we had overall graft uptake of 95.2%. In group A with a single perichondrium, the graft uptake was seen in 20 cases out of 21, and in group B with double perichondrium, the graft uptake was seen in 39 cases out of 41, both with 95% uptake rate. There was no statistically significant difference observed in both the groups. There was a statistically significant improvement in hearing outcomes with the ABG improvement of 11.9 ± 8.4.
There are few studies published on total endoscopic transcanal ear surgery for anterior perforation with graft uptake rate comparable to ours. However, we did not find any studies that had a similar surgical technique like ours.
In the study done by Gülşen and Erden, they compared endoscopic butterfly-inlay (34 cases) versus endoscopic push-through (37 cases) myringoplasty for anterior perforation and had graft uptake rate of 94.1% and 91.8%, respectively, with follow-up of 6 months. They had statistically significant improvement in hearing after the surgery. 7 Similar prospective study using the “Push through” technique was also done by Celik et al and had graft uptake of 87.5% (total cases: 32) with a mean follow-up of 12.4 months. 8 Endoscopic Transcanal Inlay myringoplasty (Butterfly technique) was done for anterior perforation by Eren et al. They had graft uptake of 95.5%, that is, 21 of 22 cases, at follow-up of 6 months. 15 In all of the abovementioned studies, tympanomeatal flap was not raised, and ossicular status was not assessed.
Tseng et al performed endoscopic transcanal myringoplasty for anterior perforation in which the tympanomeatal flap was raised, but they used temporalis fascia and/or perichondrium for the surgery. It was a retrospective study involving 59 patients with an uptake rate of 93% and a follow-up of a minimum of 6 months. 3
Özdemir et al performed endoscopic transcanal cartilage tympanoplasty in 104 patients, of which 35.6% had anterior quadrant involvement. They had overall graft uptake of 93.2% with a minimum follow-up of 6 months. The graft used was the tragal cartilage perichondrium composite graft. 9
A prospective study done by Mohanty et al on transcanal endoscopic cartilage myringoplasty for anterior perforation in 87 patients had an uptake rate of 91.9% with a minimum follow-up of 1 year. In his study, the graft used was composite cartilage perichondrium island graft with underlay technique. They also raised anterior canal wall flap along with posterior canal tympanomeatal flap under which the graft was tugged for stability. 13
Kulkarni et al published a retrospective study describing the use of barred cartilage anteriorly to support temporalis fascia for the repair of perforation. The study population was 748, of which 165 had anterior perforation. The graft uptake rate was 98.3%, with a follow-up average of 24 months. The procedure of this study is a bit similar to ours; however, they used barred cartilage reinforced by temporalis fascia and in our study, we used cartilage reinforced by perichondrium. Also, the study of Kulkarni et al was done via a postaural approach using a microscope. 16 Our procedure is minimally invasive than Kulkarni et al, as we had a single incision for tragal cartilage and all the procedures were completed by the permeatal approach.
A systemic review was published by Visvanathan et al on techniques of successful closure of anterior TM perforation. They described various techniques such as anterior anchoring, anterior hitch method, anterior interlay, anterosuperior anchoring, endoscopic push through, butterfly, lateral graft tympanoplasty, hammock tympanoplasty, Felix tympanoplasty, and endoscopic transcanal techniques. The success rate ranged from 87% to 98% with a minimum follow-up of 6 months. 6
All of the studies mentioned earlier had significant hearing improvement pre- and postoperatively, including those studies that used perichondrium and cartilage perichondrium composite graft. None of these studies had used cartilage with double perichondrium reinforced as in our study. However, our study signifies the fact that there is no negative impact on hearing outcomes using double perichondrium.
In our study, we raised the tympanomeatal flap to evaluate the status of the ossicular chain, other middle ear pathologies, and to perform underlay myringoplasty. This ensures the graft stability and avoids graft lateralization. Perichondrium was reinforced as well to avoid the theoretical risk of graft failure as the gap was seen between the barred cartilage and remnant of TM and/or annulus. The decision to use single or double perichondrium was purely dependent on the surgeon’s judgment during the surgery. If the barred cartilage with single perichondrium graft was well in touch with TM remnant and annulus then double perichondrium was not used. In both groups A and B, the uptake result was excellent with 95% and statistically no significant difference. This justified the surgeon’s decision of using single or double perichondrium during the surgery.
All of our cases were done exclusively via the transcanal approach using the endoscope, and we did not require a microscope nor postaural or endaural approach. Because of the wide view of the endoscope, all margins of perforation could be visible.
However, there are disadvantages to endoscopic ear surgery as well. It is a one-hand surgery and requires a learning curve to overcome. Sometimes instruments get crowded and at times get contaminated with bleeding. It provides 2-dimensional vision that impairs depth perception, but this can be overcome by experience and by high definition camera systems. 11
There are a few limitations to this study. First, this study has a short follow-up period and second is a relatively small sample size, resulting in a lack of generalizability of the findings. The study is retrospective which decreases the level of evidence. It would be better to perform a prospective and randomized study to decrease the bias.
Conclusion
The endoscope provides superior visualization, especially for anterior perforation making it a wonderful tool to perform surgery, avoiding postaural approach and canaloplasty. Tragal cartilage reinforced with single or double perichondrium underlay technique can be used to treat anterior perforation with excellent graft closure rate and improved functional outcomes. There is no difference in using single or double perichondrium regarding graft uptake and hearing outcomes. Thus, we recommend using single or double perichondrium reinforcement depending on the need during the surgery.
Footnotes
Authors’ Note
The research was done at Civil Service Hospital, Department of Otorhinolaryngology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.