
Abstract
Introduction
Repairing chronic anterior perforations remains challenging, regardless of whether endoscopic or microscopic myringoplasty is used. Anterior perforations present several challenges:
Anterior canal wall protrusion affects the complete exposure of anterior margins, particularly when the anterior remnants are inadequate.
Anterior margins are farther from the surgeon and more difficult to operate on than posterior margins, especially in anterosuperior perforations. This makes removing the traditional perforation margin more difficult.
Repairing anterior perforations requires raising a tympanomeatal flap with a larger circumference compared with posterior perforations.1-4
Various techniques have been proposed to improve the graft success rate for anterior perforations, including the anterior subannular grafting technique, 5 anterior tab flap underlay technique,6,7 lateral underlay technique, 2 the “U” flap technique, circumferential subannular technique, 8 “Window shade” technique, 9 loop underlay technique, 10 and the Triple-C technique. 11
These techniques often require raising a large tympanomeatal flap or removing anterior protrusions using a drill via an external auditory canal (EAC) incision, which can lead to complications, such as EAC stenosis, EAC cholesteatoma, and altered sense of taste.5,12,13
Recently, Lou et al14-16 proposed myringoplasty with preserved perforation margins and found that preserving these margins does not affect graft neovascularization or outcomes. In addition, Lou et al have reported that the over-underlay technique, where the graft covers the epithelium of the remnant tympanic membrane (TM), achieves high graft success rates without inducing graft cholesteatoma.17,18
Building on these results, we performed endoscopic cartilage myringoplasty with preserved anterior margins and an anterior folding technique of the perichondrium to repair anterior perforations. In this technique, the anterior perforation margins were preserved, while other perforation margins were not. The cartilage graft was placed medial to the anterior annulus, and the anterior free perichondrium was folded and inlaid between the cartilage graft and the anterior annulus. Excess perichondrium of the folds was placed lateral to the anterior annulus. We compared the graft success rate, hearing outcome, and complications of endoscopic cartilage inlay myringoplasty with preserved anterior margins (IPAM) with the cartilage underlay technique with raised tympanomeatal flap (CUTF) for repairing large anterior perforations.
Materials and Methods
Ethical Considerations
Ethical approval was obtained from the Medical Ethics Committee of the 908th Hospital of the People’s Liberation Army, and informed consent was obtained from all participants.
Patients and Methods
This prospective, quasi-randomized controlled trial included consecutive patients scheduled for surgery for chronic perforations and mucosal chronic otitis media at the Department of Otorhinolaryngology, Head and Neck Surgery. The inclusion criteria were adults with a chronic anterior large perforation and at least 1 mm of remnant TM around the anterior margin; a perforation size of 1/4 to 1/2 of the pars tensa area; dry ears for at least 3 months prior to surgery; an air-bone gap (ABG) of <35 dB; and good pneumatization of the middle ear and mastoid region, as seen on computed tomography (CT). Prior to enrollment, CT was performed and audiograms were recorded for all patients. The exclusion criteria were revision cases, cholesteatomas, visible ossicular chain abnormalities, acute inflammation, and fungal otitis externa.
Age, sex, perforation duration, side, anterior wall protrusion of EAC, smoking status, history of diabetes, myringosclerosis, operation time, and preoperative and postoperative hearing levels were recorded.
Audiometric data were obtained preoperatively and 6 months postoperatively. Pure-tone averages (PTAs) were calculated for both air conduction (AC) and bone conduction (BC) by averaging the thresholds at 500, 1000, 2000, and 3000 Hz. In most cases, a threshold of 4000 Hz was used to interpolate the threshold of 3000 Hz, in accordance with the standards of the Hearing Committee of the American Academy of Otolaryngology—Head and Neck Surgery. Preoperative and postoperative ABGs were calculated by subtracting the PTA for AC from that for BC. ABG closure was calculated by subtracting the postoperative ABG from the preoperative ABG.
Participant Grouping and Blinding
All patients underwent endoscopic cartilage-perichondrium myringoplasty and were divided into 2 groups through semi-randomization. Consecutive patients who met the inclusion criteria and provided written informed consent were allocated to the IPAM and CUTF groups based on the order of the visit. The perforation margins were de-epithelialized in the CUTF group, but not in the IPAM group. While the surgeon was not blinded to treatment allocation, the participants and individuals performing the assessment were blinded.
Surgical Techniques
Patients were placed in a supine position with the head oriented upward at 30° and turned toward the opposite side, where the video equipment was placed. All operations were performed under general anesthesia by the same surgeon. All patients underwent endoscopic perichondrium-cartilage graft underlay technique, and the postauricular approach was not used in any case.
A 1.0 to 1.5 cm skin incision was made on the medial side of the ipsilateral tragus and a tragal cartilage-perichondrium composite graft (with the perichondrium stripped from one side) was harvested. The lateral perichondrium was peeled circumferentially and rolled up, with the pedicle attached to the center of the cartilage. The cartilage graft was designed based on the perforation size. A notch was made in the cartilage to accommodate the malleus handle. Bioresorbable synthetic polyurethane foam (NasoPore; Polyganics, Groningen, Netherlands) was used to support the graft medially and laterally in both groups. The EAC was packed with erythromycin-soaked gauze up to the tragus incision, which was left unsutured.
Inlay Myringoplasty with Preserved Anterior Margins
In the IPAM technique, the perforation margins were de-epithelialized except for the anterior margin. The epithelium was removed from the distal malleus handle, if present, while preserving sclerotic plaques on the remnant TM.
The perichondrium-cartilage composite graft was placed across the perforation, with the cartilage positioned medial to the remnant TM and anterior annulus. The cartilage notch accommodated the malleus handle, if present.
For the posterior perforation margins, all free perichondrium was placed medial to the posterior remnant TM and the malleus handle, but lateral to the cartilage. For the anterior margins, the free perichondrium was first folded to form upper and lower folds, which were then placed between the cartilage graft and anterior annulus to create a gasket, closing the gap between the cartilage graft and anterior annulus. The excess upper perichondrium of the folds was placed lateral to the anterior annulus and EAC (Figure 1).
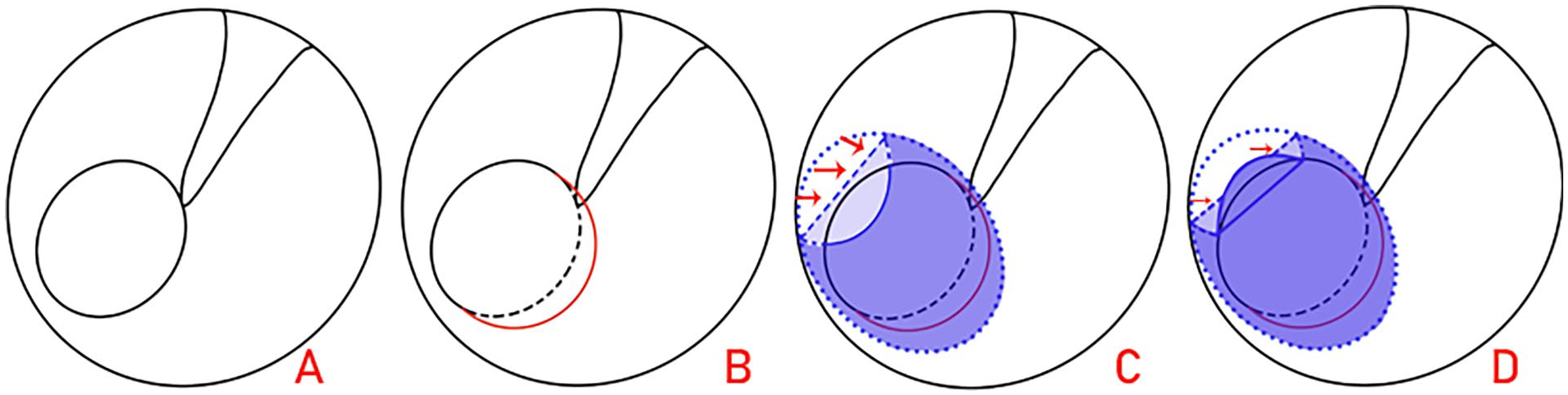
Schematic diagram. Preoperative perforation, (A) posterior margin removal with anterior margin preservation; (B) cartilage placed medial to the remnant TM and anterior annulus, but the folds of the perichondrium were inlaid with the cartilage graft and anterior annulus; (C) upper excess perichondrium of the folds lateral to the anterior annulus; (D) red arrows indicate the perichondrium folds, red arc indicates posterior margin removal, the dotted-dashed line indicates the cartilage graft, and the short dashed line indicates the original perforation edges.
Cartilage Underlay Technique with Raised Tympanomeatal Flap
Based on a previously reported technique, 17 the EAC was infiltrated with 2% lidocaine with 1:100,000 epinephrine. All perforation margins were de-epithelialized. Initially, an incision was made along the posterior half of the EAC from the 6 o’clock to 12 o’clock positions, approximately 5 mm lateral to the annulus. Vertical incisions were then made perpendicular to the TM from the superior and inferior ends of the first incision. The tympanomeatal flap was elevated from posterior to anterior, keeping it attached to the malleus handle.
The cartilage-perichondrium graft was placed through the tympanomeatal flap into the middle ear, with the cartilage positioned medial to the anterior annulus and posterior TM remnant. A notch in the cartilage graft accommodated the malleus handle, if present. The free perichondrium was placed lateral to the long process of the malleus, but medial to the TM remnant, anterior annulus, and the tympanomeatal flap. The tympanomeatal flap was then repositioned.
Postoperative Follow-Up
Patients were discharged the day after surgery. All patients were prescribed oral amoxicillin and clavulanate potassium for 1 week. The gauze pack was removed 1 week postoperatively, and the biodegradable synthetic polyurethane foam was removed 2 weeks later. Endoscopic examinations were conducted in the outpatient clinic at 2 weeks, 4 weeks, 6 months, and 12 months postoperatively. Any intraoperative or postoperative complications were recorded. Audiometric evaluations were performed 6 months postoperatively. Each follow-up was conducted by a surgeon who was not involved in the initial operation.
Outcome Measures
The outcome measures included operation time, graft success rate, audiometric outcomes, and complications. Graft success was defined as the presence of an intact graft, while graft failure was defined as residual or recurrent perforation after surgery. Residual perforation was defined as a visible perforation within 3 months after surgery, and re-perforation was defined as a perforation observed more than 3 months after surgery. Operative time was defined as the duration from the start of surgery following anesthesia induction to graft placement.
Statistical Analyses
Data are expressed as means (with standard deviations) for quantitative variables and as frequencies (with percentages) for qualitative variables. Between-group comparisons were performed using the independent-sample t-test for quantitative variables and the chi-square test for qualitative variables. The paired t-test was used to evaluate the differences in ABGs or AC thresholds. All statistical analyses were performed using SPSS Statistics, version 20 (IBM Corp., Armonk, NY, USA). A P-value of <.05 was considered statistically significant.
Results
Demographic Characteristics and Operation Time
In total, 55 patients with unilateral perforations were included in the study, all of whom completed the 12-month follow-up. Of these, 28 were included in the IPAM group and 27 in the CUTF group. Table 1 lists demographic data. Age, sex, perforation duration, side, anterior EAC wall protrusion, smoking status, diabetes, and myringosclerosis were matched between the groups. The mean operation times were 29.3 ± 2.7 minutes and 46.4 ± 3.9 minutes in the IPAM and CUTF groups, respectively; the difference was significant (P < .001).
Characteristics of Patient Sample.

Chi-square test.
Independent samples test.
Abbreviations: CUTF, cartilage underlay technique with raised tympanomeatal flap; IPAM, inlay myringoplasty with preserved anterior margins.
Graft Success Rate
The incidence of residual perforation within 3 months after surgery was 0 (0.0%) in the IPAM group and 3 (11.1%) in the CUTF group, but the difference was not significant (P = .222). All residual perforations occurred at the anterior margin. One patient (3.6%) in the IPAM group developed acute otitis media at 5 months postoperatively due to an upper respiratory infection, resulting in a small re-perforation. No reperforations were observed in the CUTF group. The overall graft success rate at 12 months postoperatively was 27 (96.4%) in the IPAM group and 24 (88.9%) in the CUTF group, with no significant difference (P = .577). Figure 2 presents the preoperative perforation and postoperative perforation closure using the IPAM technique.
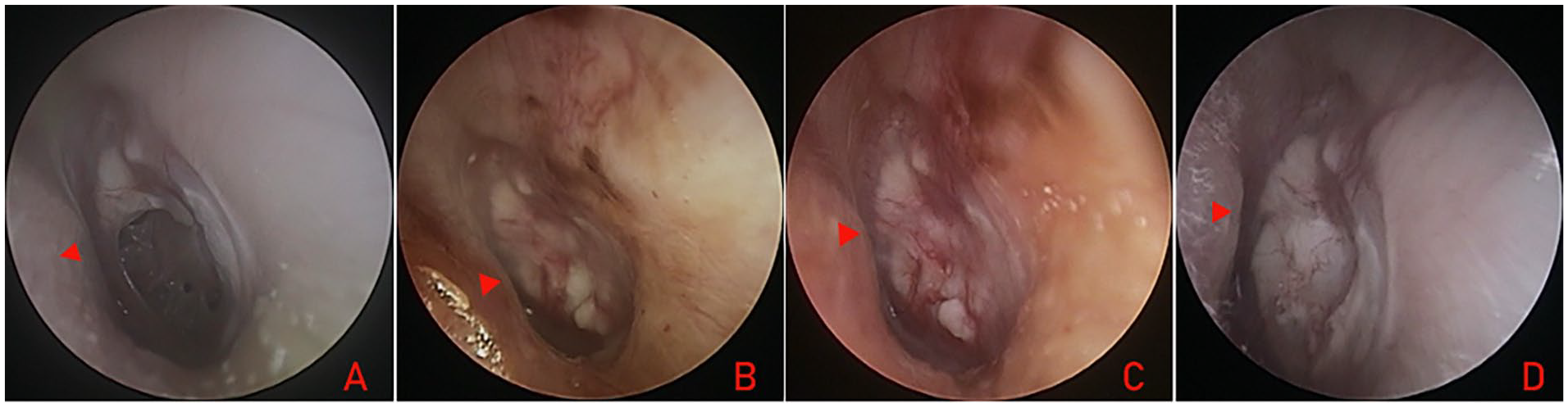
A 28-year-old female was treated using the IPAM technique. Preoperative perforation (A) and the postoperative views at 2 weeks (B), 4 weeks (C), and 12 months (D). The red triangle indicates anterior canal wall protrusion.
Audiologic Outcomes
Preoperative and postoperative audiograms were obtained for all patients. Table 2 compares preoperative and postoperative 4-tone PTAs for AC and BC. No significant differences were observed between the groups in terms of preoperative and postoperative AC PTAs, BC PTAs, ABGs, or ABG changes following surgery. The mean ABG improved by 10.9 ± 5.4 dB and 9.8 ± 7.9 dB in the IPAM and CUTF groups, respectively, with both groups exhibiting a significant difference (P < .001).
Preoperative and Postoperative Audiometric Characteristics of Patient Sample.
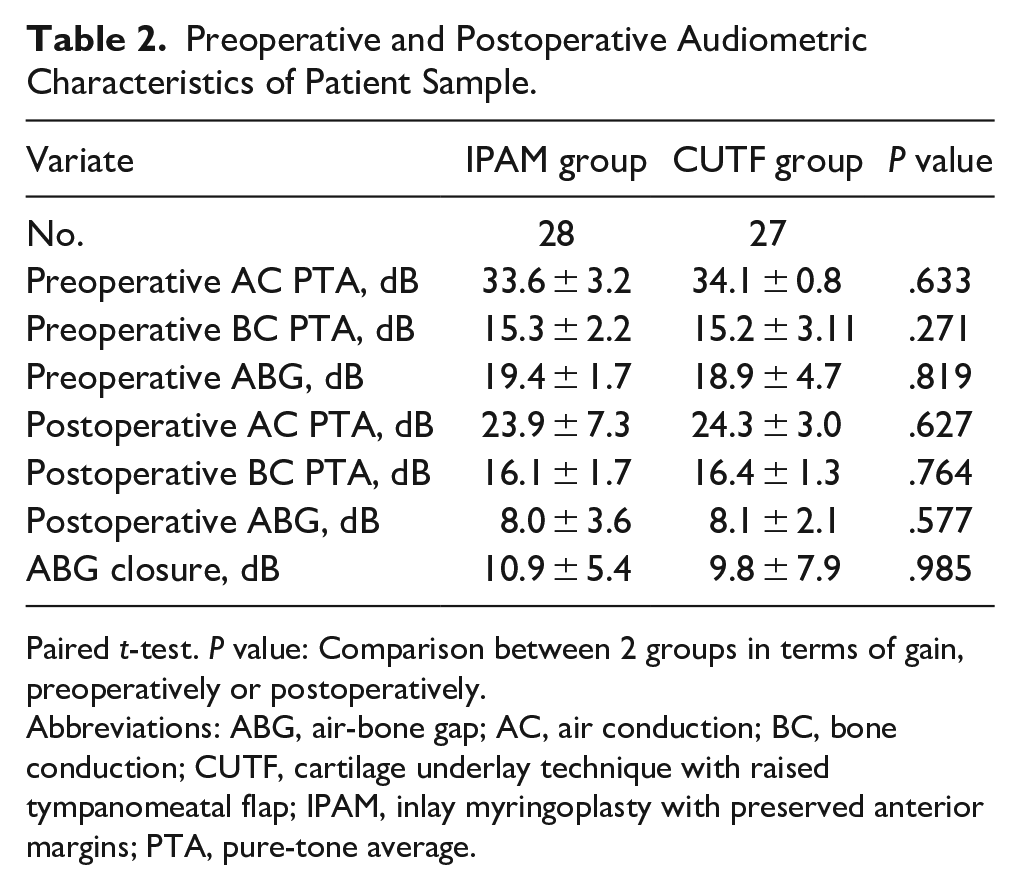
Paired t-test. P value: Comparison between 2 groups in terms of gain, preoperatively or postoperatively.
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction; CUTF, cartilage underlay technique with raised tympanomeatal flap; IPAM, inlay myringoplasty with preserved anterior margins; PTA, pure-tone average.
Postoperative Complications
No complications, such as deteriorative sensorineural hearing loss, vertigo, or tinnitus, were observed in either group during the follow-up period. None of the patients exhibited significant graft blunting, lateralization, medialization, or atelectasis. In the CUTF group, 22.2% (n = 6/27) of the patients reported altered taste perception, 3.7% (n = 1/27) experienced bony EAC stenosis, and 3.7% (n = 1/27) developed EAC graft cholesteatoma, which was removed endoscopically in the outpatient clinic. The IPAM group had no cases of altered taste perception, EAC stenosis, or cholesteatoma.
Discussion
Surgical repair of a TM perforation is a common but challenging procedure in otologic surgery. Various graft techniques and methods have been used, including underlay and overlay techniques, dry and wet grafts, and endoscopic and microscopic methods. Recent reviews and meta-analyses have demonstrated that endoscopic and microscope-assisted myringoplasties lead to similar outcomes in terms of both graft success and hearing improvement, with endoscopic approaches yielding a shorter operative time.19-21 The use of dry or wet grafts does not affect the outcome of myringoplasty, although wet grafts can shorten the operation time.22,23 In addition, the presence of active or inactive otitis media does not affect postoperative mean hearing gain or graft uptake after myringoplasty. 24 However, the underlay technique appears to be superior to the overlay technique in terms of graft uptake rate, audiological success rate, and complications. 25
An important factor influencing the complete closure of a perforation is its location. Anterior or subtotal perforations have a lower success rate compared to posterior or inferior perforations, due to challenges related to access, visualization, and inadequate anterior margin support for graft placement. 26 In our study, we preserved the anterior perforation margins, trimming only the posterior margins, visual inferior margins, and malleus handle epithelium. Posterior margins are prone to cholesteatoma formation and are easier to trim. Therefore, they were routinely trimmed in our study. Previous studies have suggested that acquired middle ear cholesteatoma mostly occurs in patients with posterior marginal perforations and perforations around the tip of the malleus handle, and is rare in cases of anterior perforations.27,28
Lou et al14-16 were the first to propose that preserving perforation margins does not affect graft neovascularization or the short- and long-term graft success rate. Their findings challenged the traditional belief that perforation edges must be trimmed. In our study, preserving the anterior margins provided adequate support for graft placement. In addition, the anterior free perichondrium was folded and subsequently inlaid between the cartilage graft and anterior annulus to close the anterior perforation margins, with the outer perichondrium of the folds placed lateral to the anterior annulus, ensuring no gaps. This technique is similar to the “tuck graft” method described previously. 18 Essentially, the anterior margins were supported by a 4-layered graft, comprising 3 layers of perichondrium and a layer of cartilage, reinforcing the anterior perforation margins. Previous studies have suggested that the graft integrates with the remnant lamina propria of the TM. 29
Lou et al’s clinical findings demonstrated that avoiding de-epithelialization does not affect the inosculation of the graft and remnant TM, graft neovascularization, or graft epithelization following cartilage myringoplasty.14-16 In addition, cartilage lacks blood vessels and has a very low metabolic rate, receiving nourishment by diffusion from the surface with the aid of the perichondrium. However, removing the perichondrium from one side does not affect the metabolism or nourishment of chondrocytes.30,31 In our study, the perichondrium was peeled circumferentially from the cartilage, with the pedicle attached to the cartilage. The excess perichondrium was not removed in the anterior perforation area but was folded lateral to the anterior remnant TM and anterior annulus, ensuring that graft nourishment was not affected.
We found that the graft success rate in the IPAM group was comparable to other techniques for repairing anterior perforations. Recent evidence-based systematic reviews on anterior perforation closure have reported graft success rates of 88.8% to 97% for anterior anchoring techniques, 97% to 98% for lateral graft tympanoplasty, 96% for “hammock” tympanoplasty, and 96% for rotational flap technique. 26 However, we found that the IPAM technique was superior to the pull-through technique for repairing anterior perforations. Celik et al 32 and Harris et al 33 reported graft success rates of 87.5% and 84.6%, respectively. Although the pull-through technique avoids raising the tympanomeatal flap and shortens the operation time, trimming the perforation margins reduces the contact area between the graft and the remnant TM.
We observed no significant differences in graft success rates between the IPAM and CUTF groups, but 11.1% of the residual perforations were observed within 3 months after surgery in the CUTF group, whereas none occurred in the IPAM group. Leaving the anterior perforation margins intact increased the contact area between the graft and the anterior remnant TM in the IPAM group, thereby reducing the incidence of anterior residual perforation. Conversely, raising the tympanomeatal flap in the CUTF group improved the visual field of the anterior margins, but reduced the contact area between the graft and the anterior remnant TM due to trimming of the anterior margins. Moreover, graft displacement toward the posterior quadrant is possible due to tympanomeatal flap contracture after surgery, increasing the risk of anterior residual perforation. In addition, patients with anterior wall protrusion were prone to tympanomeatal flap rupture; in these cases, the graft cannot be reinforced, which may lead to graft misplacement.
The choice of graft technique did not significantly affect hearing improvement in patients with a normal ossicular chain. We observed no significant differences in hearing improvement between the 2 groups, and the results were comparable to other techniques reported in the literature. 26 In the IPAM group, the primary concern was the risk of graft cholesteatoma due to the excessive perichondrium placed lateral to the anterior annulus and EAC. However, Lou et al17,18 reported that graft placement lateral to the remnant TM and annulus did not induce graft cholesteatoma. On the contrary, the CUTF group had one case of EAC cholesteatoma. Similar findings of EAC cholesteatoma with the tympanomeatal flap technique have been reported by other scholars. Ungar et al 13 reported 5 cases of iatrogenic cholesteatomas originating from a misplaced tympanomeatal flap.
Another concern with the tympanomeatal flap technique is the potential for injury to the chorda tympani nerve, leading to temporarily altered taste, 12 which was also observed in our study. In the CUTF group, 22.2% (n = 6/27) of the patients reported altered taste perception. None of the patients in either group exhibited significant graft blunting, lateralization, medialization, or atelectasis during the follow-up period.
The main strength of this study was its comprehensive 12-month follow-up for all patients. However, it also had some limitations, including a small sample size and a follow-up period limited to 12 months. In addition, although this was a prospective controlled study, the 2 groups were not completely randomized and data were obtained from a single center.
Conclusions
Endoscopic cartilage myringoplasty with preserved anterior margins and anterior perichondrium folding is a simple, effective, and minimally invasive technique for repairing large anterior perforations, yielding a high graft success rate and acceptable hearing improvement.
Footnotes
Authors’ Contributions
ShiQi Li: Interpretation of data, study design, data analysis, drafting the manuscript, and final approval for the version to be published. Xiaohua Li: Data analysis, drafting the manuscript, technical aspects of the diagrams, and final approval for the version to be published. Yuguang Li: Data interpretation, study design, and final approval for the version to be published. All authors agree to be accountable for all aspects of this study.
Ethical/Consent Statement
The study protocol was reviewed and approved by the Institutional Ethical Review Board of the 908th Hospital of the People’s Liberation Army. Written informed consent was obtained from all participants.
Data Availability Statement
All data generated or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.