
Abstract
Hypercalcemic crisis is a rare endocrine emergency that occurs in a small percentage of patients with primary hyperparathyroidism. Although modern diagnostic capabilities allow timely diagnosis and intervention, hypercalcemic crisis still has a high potential for morbidity and mortality. We report an adult patient with a history of kidney stones who presented with heart palpitations, shortness of breath, fatigue, nausea, and 20-pound weight loss over 2 months. Workup revealed hypercalcemia, elevated parathyroid hormone (PTH), and a mediastinal mass on computed tomography angiography. This patient’s hypercalcemic crisis was treated with intravenous hydration using normal saline, zoledronate, and furosemide. After medical optimization, the patient underwent definitive treatment with surgical parathyroidectomy via a transcervical approach. At operation, a large parathyroid adenoma was removed from a posterior–superior mediastinal location dorsal to the recurrent laryngeal nerve with subsequent normalization of calcium and PTH. We discuss the timing of parathyroidectomy in cases of hypercalcemic crisis and the surgical approach to ectopic parathyroid glands in the mediastinum.
Keywords
Introduction
Hypercalcemic crisis is an uncommon presentation of primary hyperparathyroidism (PHPT), occurring in less than 7% of patients with PHPT. The diagnosis is likely under-reported in the literature due to the widely varying symptoms of hypercalcemia as well as the lack of a standard definition for hypercalcemic crisis. 1 While under-reported, hypercalcemic crisis is still an unusual endocrine emergency that has the potential for high mortality if not diagnosed and treated rapidly. Acute medical treatment is guided by the nonsurgical treatment of severe hypercalcemia of malignancy, with goals to lower calcium levels, correct dehydration, and decrease osteoclast mediated bone resorption. In the case of PHPT, definitive therapy requires parathyroidectomy, with ectopic parathyroid adenomas more frequently reported in patients presenting with hypercalcemic crisis.
Hypercalcemic crisis is usually defined as an albumin-corrected serum calcium level of >14 mg/dL associated with the presence of multiorgan dysfunction. 1 Gastrointestinal manifestations include anorexia, abdominal pain, constipation, nausea, vomiting, and pancreatitis. Renal symptoms can be dehydration, oliguria, acute kidney injury, polydipsia, nephrocalcinosis, renal colic, or recurrent stones. Neurologic damage results in muscle weakness, confusion, and personality changes ranging from irritability to coma. The cardiovascular effects result from a shortened QT interval, putting the patient at risk for arrhythmias.1,2 Timely medical management is imperative and in the case of PHPT, definitive treatment involves removal of the offending parathyroid gland or glands.
Case Presentation
A 48-year-old female presented to the emergency department with heart palpitations, shortness of breath, fatigue, nausea, and 20-pound weight loss over the previous 2 months. She had a prior history of bone pain and 2 to 3 kidney stones per year. She denied the use of calcium, lithium, vitamin D, and thiazide diuretics. She denied a history of osteoporosis and family history of multiple endocrine neoplasia (MEN) syndromes or hypercalcemia. She did not have a prior cardiac history, but her mother had a myocardial infarction at the age of 30. Physical examination was significant for a heart rate of 150 bpm and blood pressure of 192/102. Laboratory evaluation revealed a calcium of 16.7 mg/dL, albumin of 4.4 g/dL, phosphorus of 2.7 mg/dL, magnesium of 1.4 mg/dL, creatinine of 1.42 mg/dL, thyroid stimulating hormone of 3.28 uIU/mL, parathyroid hormone (PTH) of 1029 pg/mL, and a 25-hydroxyvitamin D of 6 ng/mL. Computed tomography (CT) angiogram of the chest was obtained to rule out pulmonary embolism and revealed “no acute pulmonary embolus [or] acute cardiopulmonary process.” A “2.9 cm mediastinal heterogeneous mass” was also reported (Figure 1). A diagnosis of hypercalcemic crisis secondary to PHPT was made, and the endocrinology service was consulted.
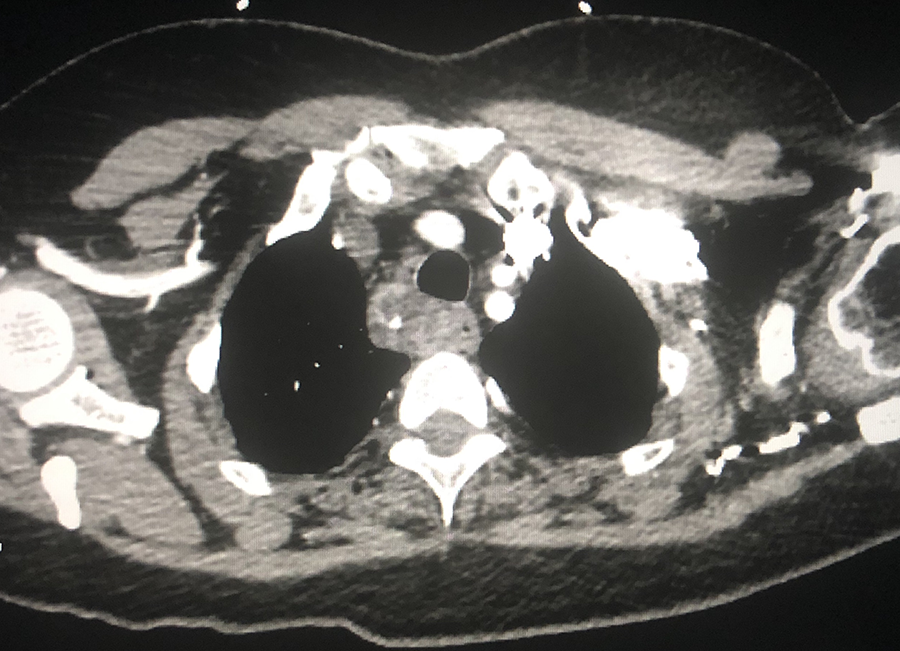
CT angiography of chest showing paraesophageal mass in right superior mediastinum.
The patient was hydrated with intravenous normal saline, and the extremely elevated calcium level was managed with zoledronate and furosemide. Potassium and magnesium were replaced, and she was started on cholecalciferol 50 000 IU per week.
Head and neck surgery was consulted once the patient’s calcium was 10.8 and her symptoms had resolved. The case was discussed with cardiothoracic surgery due to the location of the mediastinal mass. Head and neck surgery then proceeded with transcervical exploration and removal of the mass (Figure 2). At operation, the mass was found deep to the recurrent laryngeal nerve and adjacent to the esophagus, along the tracheoesophageal groove. The specimen was submitted for frozen section pathological examination. It was reported to weigh 10 000 mg and was consistent with hypercellular parathyroid tissue. Baseline PTH was 639.7 pg/mL after induction of general anesthesia and dropped to 89.9 pg/mL approximately 10 minutes after resection. Laboratory evaluation on postoperative day 1 revealed a PTH of 11.0 pg/mL, calcium of 9.9 mg/dL, albumin of 3.8 g/dL, and phosphorus of 1.3 mg/dL.

Mass excised from right superior mediastinum was consistent with a parathyroid adenoma.
Discussion
Primary hyperparathyroidism most often presents as asymptomatic hypercalcemia. 2 Another subset of patients presents with low bone mineral density. Workup in these patients reveals elevated PTH levels but normal total and ionized calcium. 2 The classic presentation which includes symptoms such as osteitis fibrosa cystica, recurrent nephrolithiasis, or neuromuscular features is relatively uncommon. 3 In rare cases, hyperparathyroidism can lead to hypercalcemic parathyroid crisis which can cause severe dehydration or coma. 4
The presentation of this patient with a single mediastinal mass, recurrent nephrolithiasis, with high serum calcium, and PTH in absence of other explanations is consistent with PHPT. In these patients, PHPT is most often caused by a single parathyroid adenoma. 5
The only definitive treatment in symptomatic patients is parathyroidectomy with removal of the abnormal glands. For asymptomatic patients, surgical intervention is recommended when 6 : (1) serum calcium > 1.0 mg/dL over the upper limit of normal; (2) osteoporosis with T-score of ≤−2.5 at the lumbar spine, hip, or distal radius; (3) vertebral fracture by radiograph, CT, magnetic resonance imaging, or vertebral fracture assessment; 4) estimated GFR <60 mL/min; (5) 24-hour urine calcium >400 mg and increased stone risk by biochemical stone risk analysis, (6) presence of nephrolithiasis or nephrocalcinosis by radiograph, ultrasound, or CT; and (7) age < 50 years. Asymptomatic patients who do not have one of these criteria can be observed unless they prefer or request to have surgery, they have coexistent illness that complicates surveillance, or they are unlikely to follow-up. 7
Ectopic parathyroid glands occur in approximately 16% of patients presenting with PHPT and most of these are ectopic inferior glands (62%). 8 A posterior–superior mediastinal location dorsal to the recurrent laryngeal nerve is suggestive of an ectopic superior gland, which only occurs in approximately 5% of all ectopic parathyroid glands and in approximately 0.8% of all patients presenting with PHPT. 8 An ectopic superior parathyroid gland as seen in this patient is rare and highlights the surgical issues relative to parathyroid localization.
Surgical approach to ectopic mediastinal glands can be transcervical, transthoracic via median sternotomy, or thoracoscopic. 9 The favored approach depends on surgeon experience and location of the gland.
Following surgical resection, serum calcium commonly falls. This mild decrease is expected to resolve within 2 to 4 days. 10 If the patient remains hypocalcemic beyond this and/or a severe drop in total serum calcium concentration to <2.1 mmol/L occurs, hungry bone syndrome, a common clinical complication following parathyroidectomy, should be suspected. 10 A persistently elevated PTH level stimulates osteoclast number and activity, leading to the increased bone resorption and occasionally the classical manifestations of osteitis fibrosa cystica and brown tumors. When the PTH level drops, osteoclast activity turns off while osteoblast activity continues and new bone is formed. 10 These changes in bone remodeling homeostasis result in an influx of calcium into bone which leads to hypocalcemia sometimes with a drop in phosphorus and magnesium concentrations. The hypocalcemia and hypophosphatemia can last several months postoperatively and cause neuromuscular irritability with carpopedal spasm, perioral paresthesias, Chvostek sign, and/or Trousseau sign. 11 These electrolyte abnormalities must be aggressively replaced with frequent monitoring of total serum calcium level. In patients who are symptomatic, serum ionized calcium should be checked. Treatment should include oral administration of 4 to12 g/d of elemental calcium with 2 to 4 µg/d of calcitriol. 10
This case highlights the value of a multidisciplinary approach to PHPT because calcium abnormality can persist even after surgical removal of the offending gland especially in the setting of vitamin D deficiency. Surgeons must also be aware of the possible ectopic location of parathyroid glands as surgical exploration and parathyroidectomy are considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.