
Abstract
The parapharyngeal space has been described as an inverted pyramid shape with the base of the skull and the great cornu of the hyoid bone at the top. Tumors of the parapharyngeal space account for 0.5% of head and neck tumors and a wide range of tumor types can occur in this area, 80% of which are benign, the most common being pleomorphic adenomas of the salivary glands and neurogenic tumors. We present a 39-year-old woman who was hospitalized due to left-sided neck pain with a feeling of blockage in the left ear and hearing loss for 10 months. Imaging showed that the mass was not connected to the cranium and the patient underwent surgical resection via a transoral approach, where the contents of the mass were found to be cerebrospinal fluid, and meningocele in the parapharyngeal space is a rare occurrence. The patient presented mainly with painful symptoms, which were eventually relieved by nerve block therapy.
Introduction
Only about 0.5% of all head and neck tumors occur in the parapharyngeal space (PPS),1,2 of which about 80% are benign lesions, the most common being pleomorphic adenomas of the salivary glands and neurogenic tumors,3,4 with rare cases of meningeal bulging into the PPS. Meningoencephalocele is a condition in which the meninges and their contents herniate as a result of an abnormality of cranial closure. If the herniated material is meninges and cerebrospinal fluid (CSF), it is called meningocele, and if the herniated material also contains brain tissue, it is called encephalocele. 5 According to the anatomical location of the occurrence of encephalocele, it can be classified as occipital encephalocele, encephalocele of the cranial vault, frontoethmoidal encephalocele, and basal encephaloceles. 6 Basal meningoencephaloceles are extremely rare congenital malformations and are usually occult. 7 Here, we report a case of meningocele into the PPS.
Report of a Case
A 39-year-old woman presented to our outpatient clinic with a 2 week history of postauricular pain in the left ear. On examination, the patient presented with pressure pain in the left mastoid apical region, narrowing of the aural opening by a bulge in the posterior wall of the ipsilateral external auditory canal, and poor tympanic membrane peeping. Ultrasound of the left postauricular mastoid area suggested bone erosion with swelling of the surrounding soft tissues, and inflammatory changes were considered. To clarify what was causing the patient’s bone erosion and postauricular pain, we further refined the computed tomography (CT). On CT examination, we noted that the patient had a huge occupancy in the left PPS, with bone resorption defects in the left portion of the occipital slope and the rocky and phosphorus part of the temporal bone, and we considered the possibility of encircling the siphon segment of the left internal carotid artery (Figure 1a and b). Enhanced CT showed a mass-like slightly low soft tissue density shadow visible in the left PPS, with uneven density, about 4.2 cm × 2.7 cm × 3.4 cm in size, locally indistinguishable from the parotid gland, and a soft tissue density shadow visible in the left external auditory canal, with corresponding stenosis of the external auditory canal, eccentric stenosis of the nasopharyngeal cavity, and shallowing of the left pharyngeal orifice of the Eustachian tube and pharyngeal saphenous fossa. Magnetic resonance imaging (MRI) suggests that the left PPS can be seen as a mass of mixed long T2 signal shadow, with clear boundaries, within which the signal is not homogeneous, and can be seen as a patchy short T2 signal shadow, surrounded by a ring of high signals (Figure 2a-e). Taken together, the aforementioned findings suggest a neoplastic lesion, the nature and origin of which is unclear.
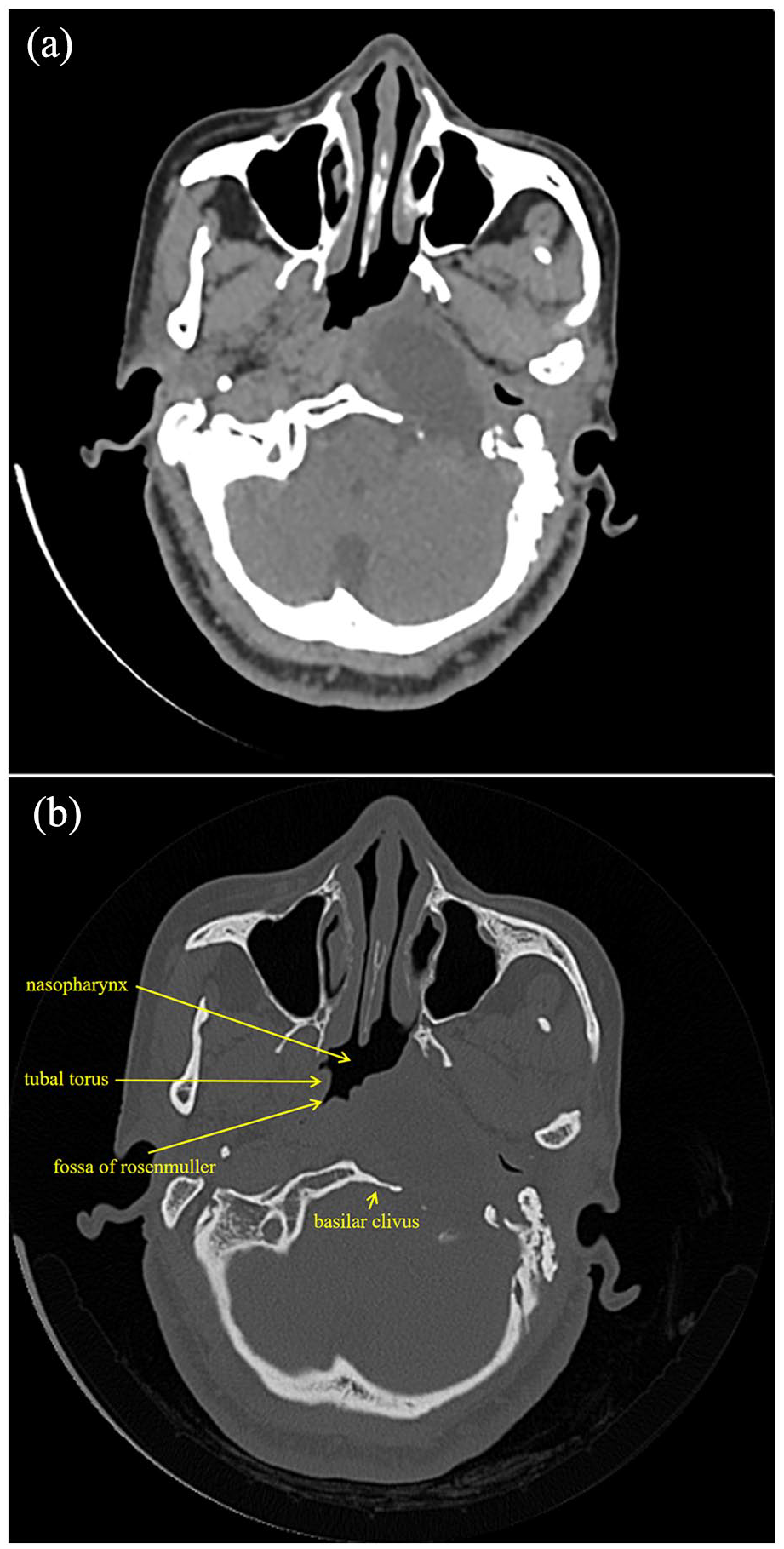
(a, b) Axial CT of the skull and brain showed a huge occupancy of the left parapharyngeal space with peripheral bone resorption defects. CT, computed tomography.
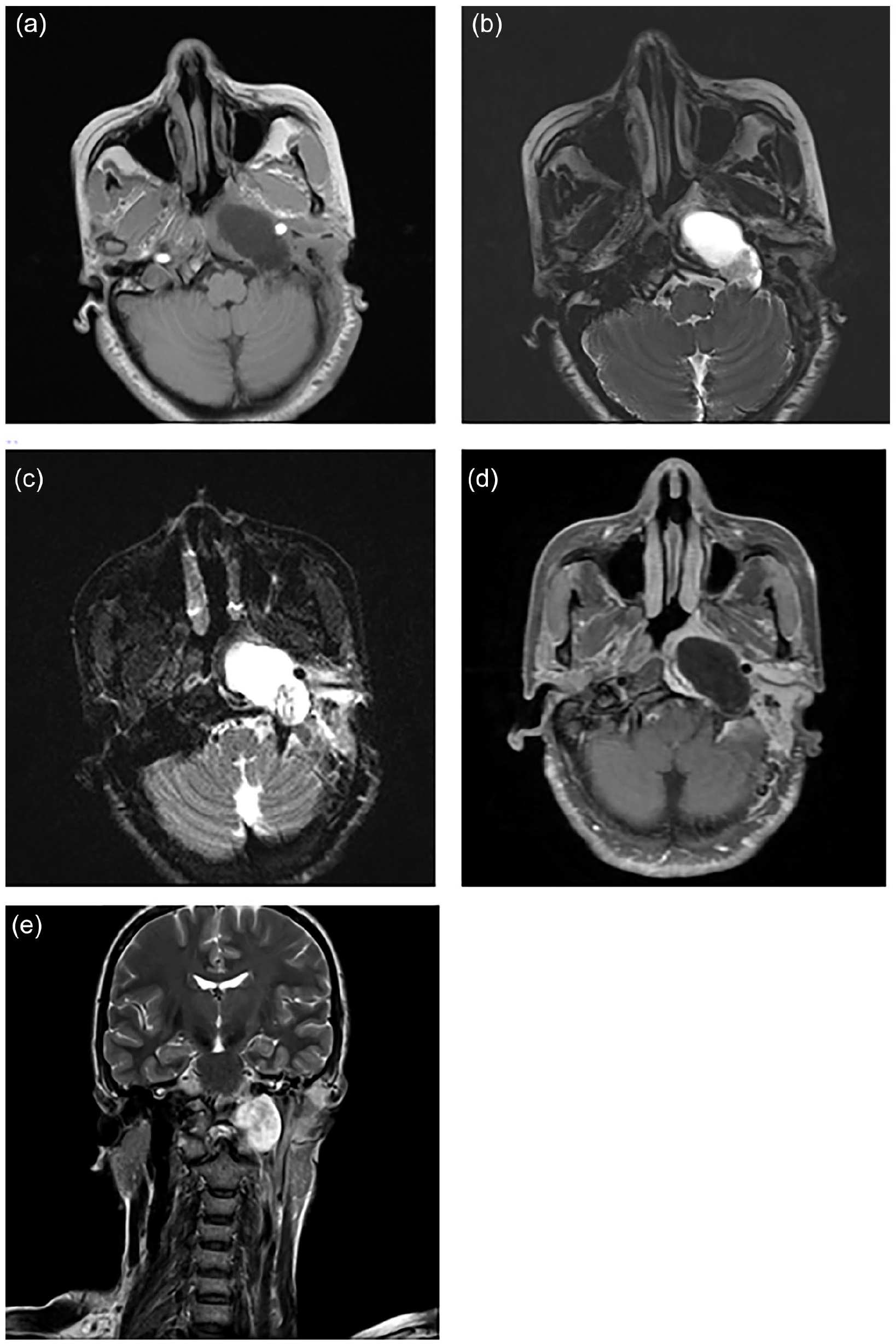
(a-e) On cranial axial and coronal MRI, a mass with mixed long T2 signals was observed in the left parapharyngeal space. The mass had clear borders and inhomogeneous signals within it, and was surrounded by a ring of high signals (a: T1WI; b: T2WI; c: DWI; d: enhanced MRI; e: T2WI). MRI, magnetic resonance imaging. T1WI, T1-weighted imaging; T2WI, T2-weighted imaging; DWI, diffusion weighted imaging.
Notably, on physical examination, it was found that the patient had multiple broad bean to egg-sized nodules and swellings all over the body, which were soft in texture and had no pressure pain. Her mother had a history of similar disease, and her family complained that the patient’s intellectual development was slightly abnormal. The patient’s MRI indicated diffuse foci of abnormal enhancement in the subcutaneous area of the neck, which was considered to be neurofibromatosis in the context of the patient’s medical history, family history, and imaging findings, but no pathological examination was performed. Neurofibromatosis is a dominantly inherited disease that has been reported to be associated with intracranial tumors, and tumors associated with neurofibromatosis may be histopathologically identical to cutaneous neurofibromas.8-11 In this case, the patient has a partially palpable mass on the left side of the neck, hard, with pressure pain, and the imaging data showed that the mass had a clear and definite boundary and had not yet been seen to be connected to the cranial brain, so it was initially considered to be a “schwannoma” or “neurofibroma,” and was considered to be surgically resected. After surgical resection, a pathological examination of the mass should be performed to determine the diagnosis.
Informed consent for surgery was obtained from the patient. She was scheduled to undergo transoral approach tissue biopsy and resection. Intraoperatively, we punctured the mass with a syringe and withdrew clear fluid, which was considered CSF (Figure 3). Biochemical examination of the CSF indicated CSF protein 222 mg/L, glucose 4.83 mmol/L, and chloride 124.3 mmol/L, suggesting that the contents originated from meningocele, and the operation was stopped and the operative cavity was closed with sutures. The postoperative diagnosis was “parapharyngeal space mass (meningocele).”
The clear liquid obtained from the puncture of the mass.
Postoperatively, we irrigated and changed the patient’s left soft palate incision, which healed well. The patient had pain in the left ear and pain in the left side of the neck, and the examination showed signs of pain in the innervation area of the auriculotemporal and auriculo-major nerves, which was relieved by nerve block treatment.
Discussion
This anatomical region of the PPS is quite complex and has been described as an inverted pyramid, with its base located in the skull and the hyoid bone forming its apex. 12 The boundaries of the PPS are defined as follows: superiorly, the inferior surface of the temporal bone; inferiorly, the greater cornu of the hyoid bone and the posterior belly of the digastric muscle; anteriorly, the pterygomandibular ligament and the submandibular gland; posteriorly, the prevertebral fascia; medially, the nasopharynx and oropharynx; and externally, across the mandibular branches. 13 PPS is a relatively rare primary pathological site, accounting for 0.5% of head and neck tumors.1,2 A variety of tumor types can occur at this site, 80% of which are benign, the most common being pleomorphic adenomas of the salivary glands and neurogenic tumors,3,4 which are usually located in the pre- and post-styloid PPSs, respectively, 14 which are bounded by the styloid process and its attached muscles.
Because of the deep location of the PPS, its clinical manifestations are usually caused by the occupying effect, and the most common clinical symptoms are neck mass and/or intraoral asymmetry with tonsillar displacement and/or palatal protrusion, and the patients may complain of pain, dysphagia, hoarseness, otalgia, and snoring, etc. Due to the compression of the Eustachian tube, a plasma effusion of fluid in the middle ear can be seen on the side of the lesion. 15
Differential diagnosis can be made on the basis of the contents of the space and its resulting magnetic resonance manifestations. MRI is the imaging modality of choice for the evaluation of soft tissue masses, and provides better tissue characterization than CT, but final diagnosis requires a pathohistological biopsy. Pleomorphic adenomas of the salivary glands are the most common primary parapharyngeal interstitial lesions, accounting for almost half of all lesions in this location, 16 which may appear on MRI as T2 high signal, isosignal, or low signal with varying degrees of enhancement. Schwannomas are usually well defined, with heterogeneous T2 long signal and may have a T2 long signal rim, whereas neurofibromas have similar features but tend to enhance less than schwannomas and are usually not associated with a T2 long signal rim. 17 MRI is also preferred to identify meningocele due to the superior anatomical resolution of magnetic resonance in characterizing malformations of the central nervous system. 18 Meningoencephalocele can show cranial defects on imaging, as well as the same signal as brain tissue or CSF.19,20
Meningoencephalocele is the protrusion of neural tissue, CSF, meninges, and other cranial contents due to congenital or acquired pathologies.21,22 Approximately 70% to 90% of all encephaloceles occur in the occipital region of the skull, 23 whereas basal meningoencephalocele are very rare, and potential causes include congenital defects, trauma, infection, and intracranial hypertension.24-26 Depending on the type of disease and the location of the brain tissue involved, patients may present with headaches, seizures, meningitis, CSF leakage from the nose and ears, etc.27,28 CSF nasal or ear leakage can be confirmed by the presence of β-2-transferrin or glucose. 29 Surgery is usually the preferred treatment modality,20,30 and endoscopic intranasal approach may be used as a treatment option for specific patients such as anterior skull base defects. 31
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Basic Scientific Research Projects of Central Universities - the Project of Major Needs Cultivation [31920220107]; the Project of Lanzhou Science and Technology Plan [2023-4-2].
Ethical Approval
Ethical approval is not applicable for this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Verbal informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.