
Abstract
The objective of this study is to evaluate otitis media with effusion (OME) among patients with parapharyngeal tumor. We have experienced 82 parapharyngeal tumor cases and encountered 14 patients complaining of hearing loss due to OME as the initial symptom. These patients showed normal nasopharyngeal findings and the presence of tumor had been detected long time after the beginning of their hearing symptoms (4 months to 13 years: median 2.5 years). Six patients had undergone ventilation tube insertion on the affected ear, which may lead to delay in diagnosis. Pathological examination was performed in 76 of 82 patients. Among these 76 patients, 13 showed OME. Seven patients had malignant lesions, whereas 6 had benign lesions. Therefore, malignant lesions are prone to occur with OME and its relative risk was 2.26 (95% confidence intervals, 1.16-4.42). This difference was statistically significant (P = .044, Fisher test). Otitis media with effusion is a very common disease and is well-known as a primary symptom of nasopharyngeal carcinoma. Therefore, nasopharyngeal observation is necessary for patients with intractable middle ear effusion. However, present 14 patients with OME showed normal nasopharyngeal findings and finally found after an imaging study. From our data, OME is an important but go-by symptom of parapharyngeal tumors. Imaging studies are potently useful for such patients with intractable OME.
Keywords
Introduction
The orifice of the Eustachian tube (ET) is situated in the nasopharynx, so nasopharyngeal disorders, such as adenoid vegetation and nasopharyngeal carcinoma, cause otitis media with effusion (OME). 1,2 Therefore, nasopharyngeal observation is necessary for patients showing middle ear effusion, especially in elderly populations. On the other hand, the ET connects the nasopharynx to the middle ear and is located in the parapharyngeal space. 3 Although rare, various tumors develop near the ET and contact or distort the ET. 3 -5 These conditions may develop middle ear disorders, such as OME. 4,6,7 In this report, we investigated patients with OME with parapharyngeal tumors showing normal nasopharyngeal findings.
Patients and Methods
We encountered 82 parapharyngeal tumors from 2003 to 2016. Interviews concerning hearing disturbance and observation of the tympanic membrane as well as nasopharynx were routinely done. Once any kind of hearing-related problems was found, additional history taking, hearing test, and impedance audiometry were performed. These findings were compared to the imaging study, and surgical and pathological findings. Statistical analysis was performed using JMP 8 (SAS Institute, Inc, Cary, North Carolina). The incidence was analyzed using Fisher exact test. The institution review board of Juntendo University, Nerima Hospital, approved this project (S 19-02).
Results
Fourteen patients showed unilateral hearing loss and/or OME as an initial symptom (Table 1). All patients underwent nasopharyngeal endoscopic examination and showed no abnormal findings and were diagnosed only after imaging studies. They noticed hearing loss beforehand, but the presence of tumor had not been detected until after the beginning of their hearing symptoms. The duration of this interval varied from 4 months to 13 years (median: 2.5 years). Six patients had undergone ventilation tube insertion on the affected ear, which may be related to the late diagnosis. The clue to diagnosis in these 14 patients was imaging examination, the reason for which varied in each patient. Occasional examination of the brain was the most common reason for imaging study, followed by pain or abnormal sensation in the facial region.
Lists of Patients.
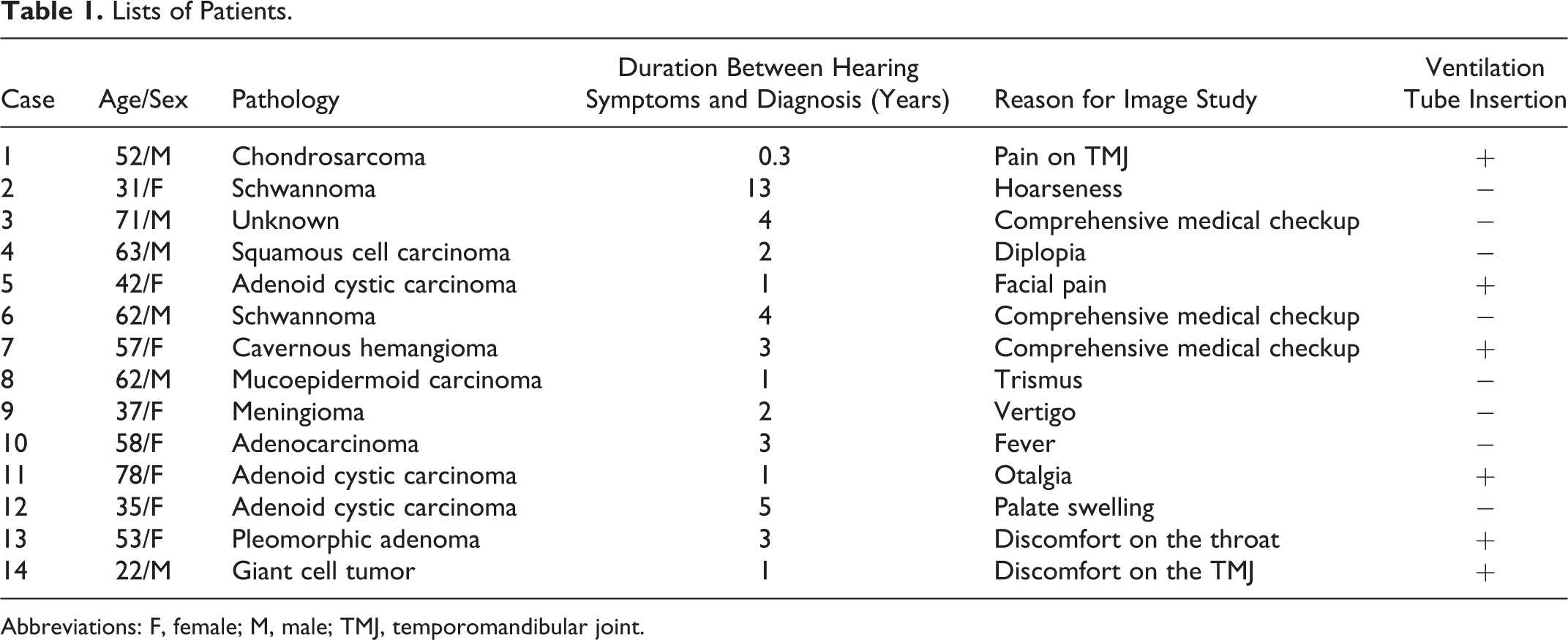
Abbreviations: F, female; M, male; TMJ, temporomandibular joint.
Of the 82 patients, 76 underwent pathological assessment by biopsy or surgery. Fifty-four patients had benign tumors and only 6 patients showed OME. On the other hand, the remaining 22 had malignant tumors and 7 patients had OME. Compared to benign lesions, malignant lesions were more likely to develop OME and this tendency was statistically significant (Table 2, P = .044, Fisher test). Therefore, malignant lesions are prone to occur with OME and its relative risk was 2.26 (95% confidence intervals: 1.16-4.42).
Result of Analysis of Occurrence of OME Between Benign and Malignant Lesion.
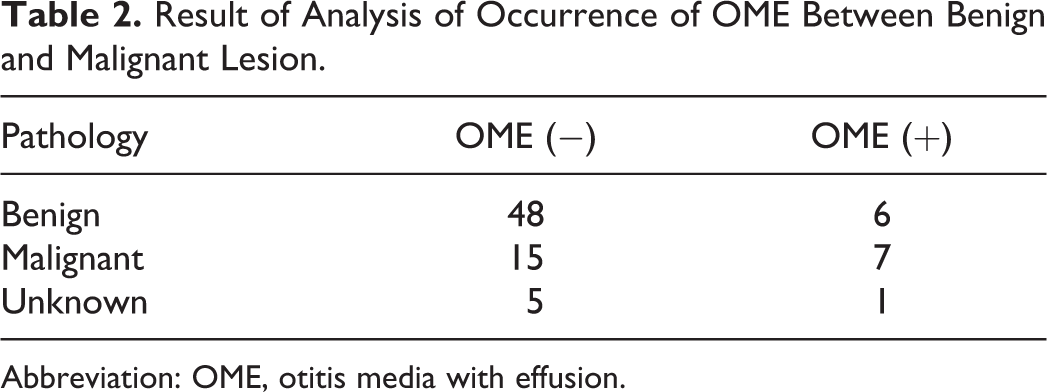
Abbreviation: OME, otitis media with effusion.
Discussion
Otitis media with effusion is a common cause of deafness in children and is also seen in adults. It appears as sequelae of acute otitis media, adenoid vegetation, and sinusitis. It silently affects children or senile populations and causes various glue ear deafness-related clinical problems, such as with language acquisition, communication disturbance, and even dementia. 8 It is also well-known as a primary symptom of nasopharyngeal carcinoma and other nasal and nasopharyngeal lesions. 1,9,10 Therefore, ear, nose, and throat doctors usually consider the possibility of nasopharyngeal carcinoma and perform endoscopic observation of the nasopharynx, especially for adult patients showing intractable OME. However, once the nasopharynx revealed to be normal, additional examination is not usually done. In such a situation, myringotomy may be performed. Ventilation tube insertion is also performed for recurrent cases. Both myringotomy and ventilation tube insertion cure immediately and the latter completely cure OME while tube is inserted. As a result, diagnostic delay for a latent parapharyngeal lesion may occur.
Parapharyngeal tumors are rare, but various pathologies occur in this region. Symptoms of parapharyngeal tumor also vary, such as neck mass, sleep apnea, dysphagia, dyspnea, pharyngeal mass, and OME. 4,6,11 -13 In our previous report, we described that mechanical obstruction of the ET by a benign tumor of the parapharyngeal space does not always cause OME. 3 In the present study, we show that malignant tumors are more prone to cause OME as compared to benign tumors, and the difference was statistically significant. Therefore, otological interventions for OME, such as a ventilation tube insertion, may lead to diagnostic delay for malignant lesions.
Imaging studies, such as computed tomography and/or magnetic resonance imaging, are effective for the detection of latent parapharyngeal lesions causing OME, but the application of such examinations for all patients with OME is considered to be unrealistic. Therefore, clinicians must consider the possibility of a parapharyngeal tumor in patients with OME. In case with intractable unilateral OME showing normal nasopharyngeal findings, imaging study should be considered for the early detection of a parapharyngeal tumor. 7
Footnotes
Acknowledgments
The authors deeply thank Professor Kitamura K. and Dr Sumi T. for their clinical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.