
Abstract
Angioleiomyoma is a benign smooth muscle and vessel tumor; laryngeal localization is extremely rare with only 24 cases described in the literature; moreover, it should be considered in the differential diagnosis of laryngeal mass. Endoscopic complete surgical excision with dissection along capsule is now considered the gold-standard treatment for small and well-circumscribed laryngeal angioleiomyoma. We present a case of laryngeal angioleiomyoma successfully treated with carbon dioxide laser technology which resulted in a bleeding reduction and adequate hemostasis with less tissue damage and good functional outcome.
Introduction
Angioleiomyoma or vascular leiomyoma is a benign subcutaneous or deep dermal tumor of smooth muscle and vessels. Most vascular leiomyomas are found in the skin, but in the head and neck area, it can also developed in the mucosa, 1,2 more often, it is located in the extremities (lower 59% and upper 15%), uterus, and gastrointestinal tract. 2 Head and neck localization is very rare (13.1% of cases), and there are few reports available in the literature; the most frequent sites are ear, lip, nose, and neck: larynx localization is extremely rare, in fact, the first case in literature was described in 1946. 2 -4 We present a case of angioleiomyoma of the medial wall of the pyriform sinus with a literature review.
Case Presentation
A 67-year-old man accessed to our Ear-Nose-Throat (ENT) department in December 2018 complained of a history of increasing dysphagia and hoarseness for 1 month. The patient past medical history was unremarkable, he was a nonsmoker and a mild drinker and did not present fever or other systemic symptoms and no dyspnea, odynophagia, cough, or hemoptysis.
A complete ENT examination was carried out. Videolaringoscopic examination showed the presence of a smooth submucosal mass in the medial wall of the right pyriform sinus covered by normal mucosa, hypomobility and paramedian position of the homolateral vocal fold was also seen without airway compromise (Figure 1). Based on clinical evidence, a computed tomography (CT) with contrast enhancement of the head and neck was indicated and revealed an expansive, solid, round shape, 17-mm lesion localized in the medial wall of the right pyriform sinus, it showed well-defined margin and excellent peripheral contrast enhancement. The mass did not demonstrate any signs of local involvement or injury of the adjacent structures, none extra laryngeal extension; moreover, no pathological lymph nodes were found (Figure 2).
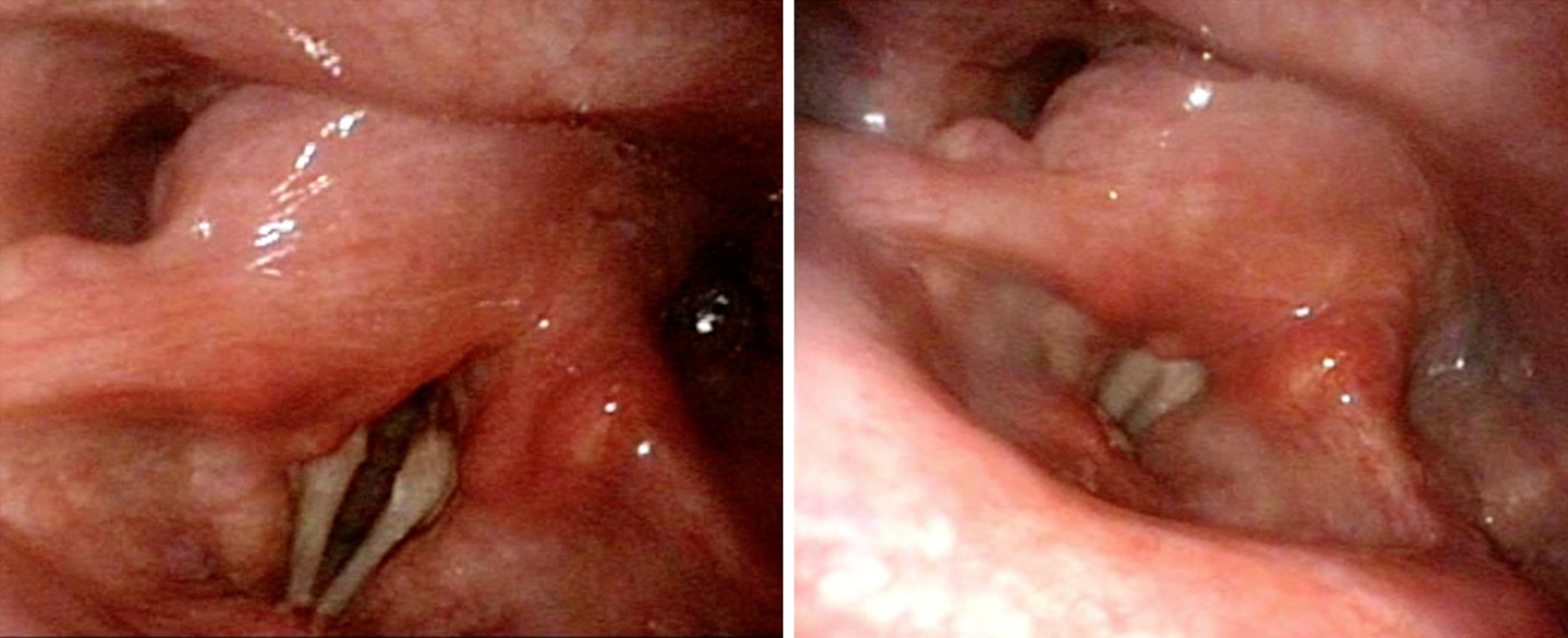
Endoscopic view of the tumor as a smooth submucosal mass covered by normal mucosa in the medial wall of the right pyriform sinus without airway compromise.
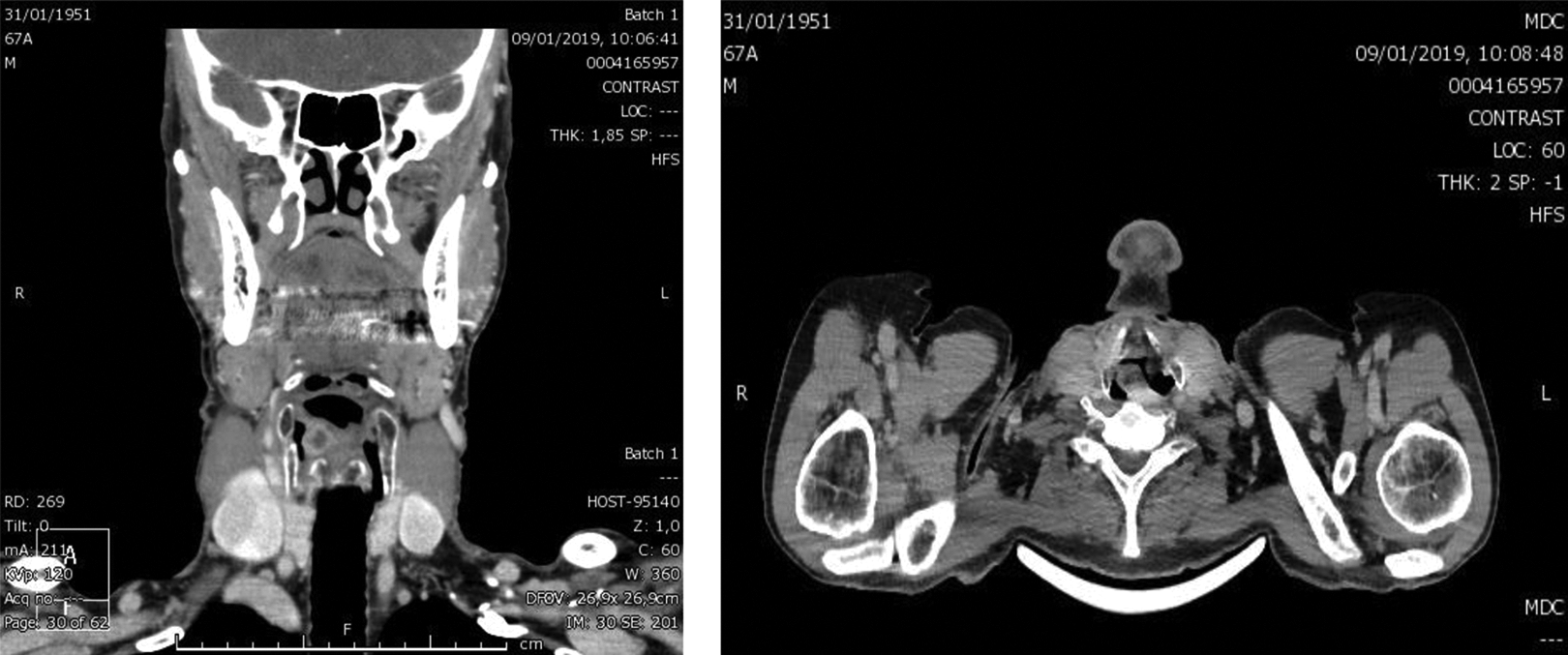
Computed tomography (CT) with contrast enhancement revealed a 17-mm lesion localized in the medial wall of the right pyriform sinus with a well-defined margins and peripheral contrast enhancement without any signs of local disruption.
Among clinical and radiological evidence, in the suspect of benign pathology, we performed a surgical excision with a diagnostic and therapeutic goal.
The tumor was excised through direct microlaryngoscopy under general anesthesia with a carbon dioxide (CO2) laser technique; it was exposed and wholly removed along with its capsule without significant bleeding. The surgical specimen was sent to the Pathology Department for diagnosis fixed in a formalin solution.
Histological examination demonstrated ovoid and spindle smooth muscle cells arranged in variably intersecting boundless between slit-like vascular channels. The tumor cells were resulted consistently and diffusely positive for smooth muscle actin, caldesmon, and desmin. All of those findings were consistent with a solid type angioleiomyoma (Figures 3, 4, and 5).
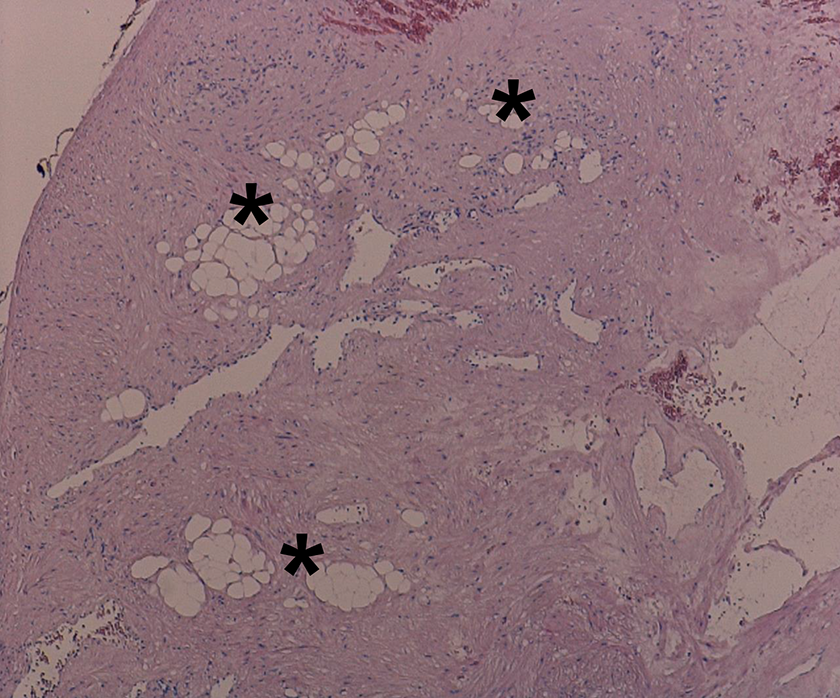
Variably intersecting boundless of typical smooth muscle cells with intervening slit-like vascular channels and small collections of mature fatty elements (*) (Hematoxylin and Eosin, ×10).
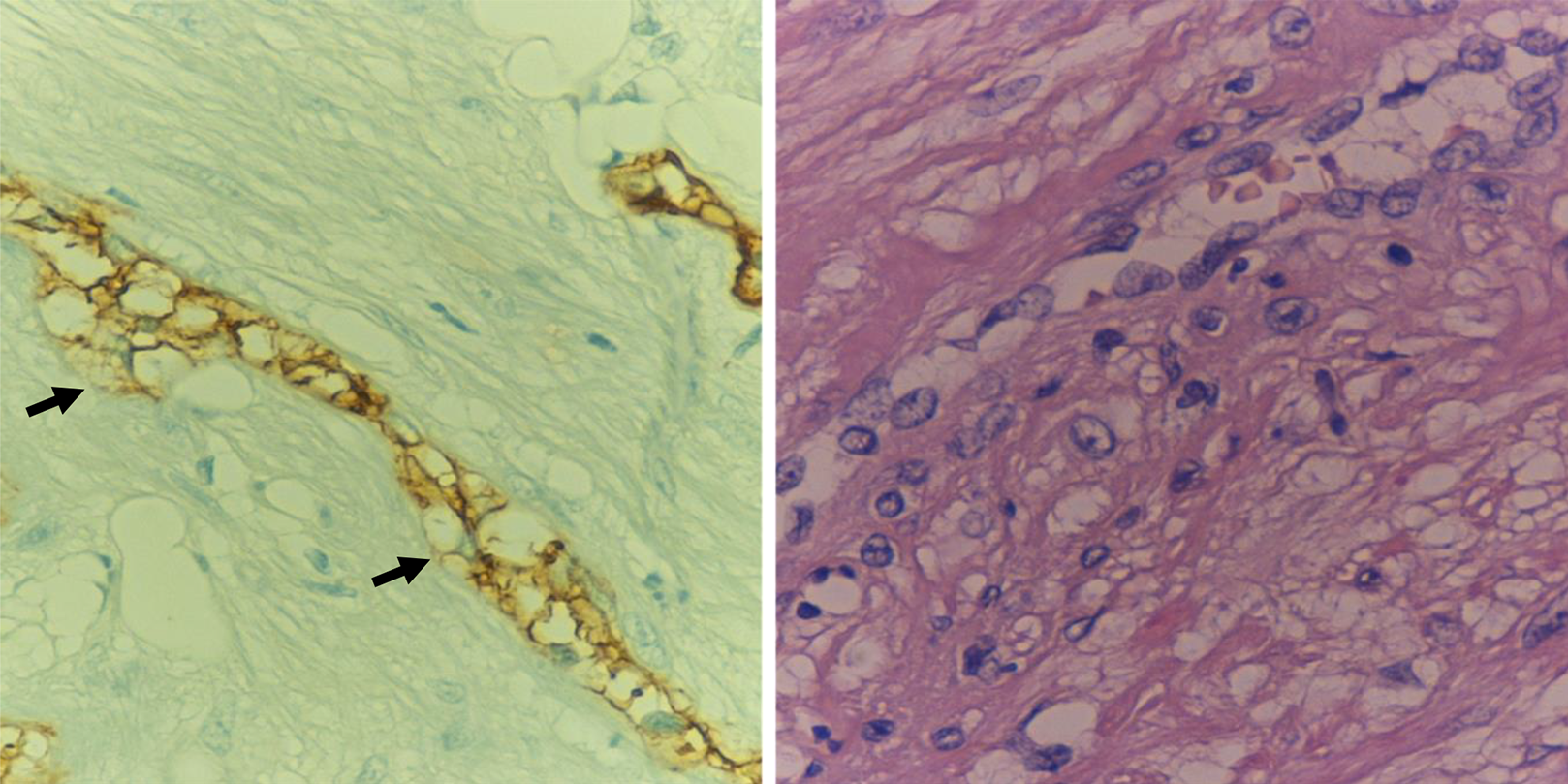
Pseudolipoblastic changes (arrows) characterize CD34 (on the left) positive endothelial cells (immunoperoxidase-avidin-biotin complex; ×20).
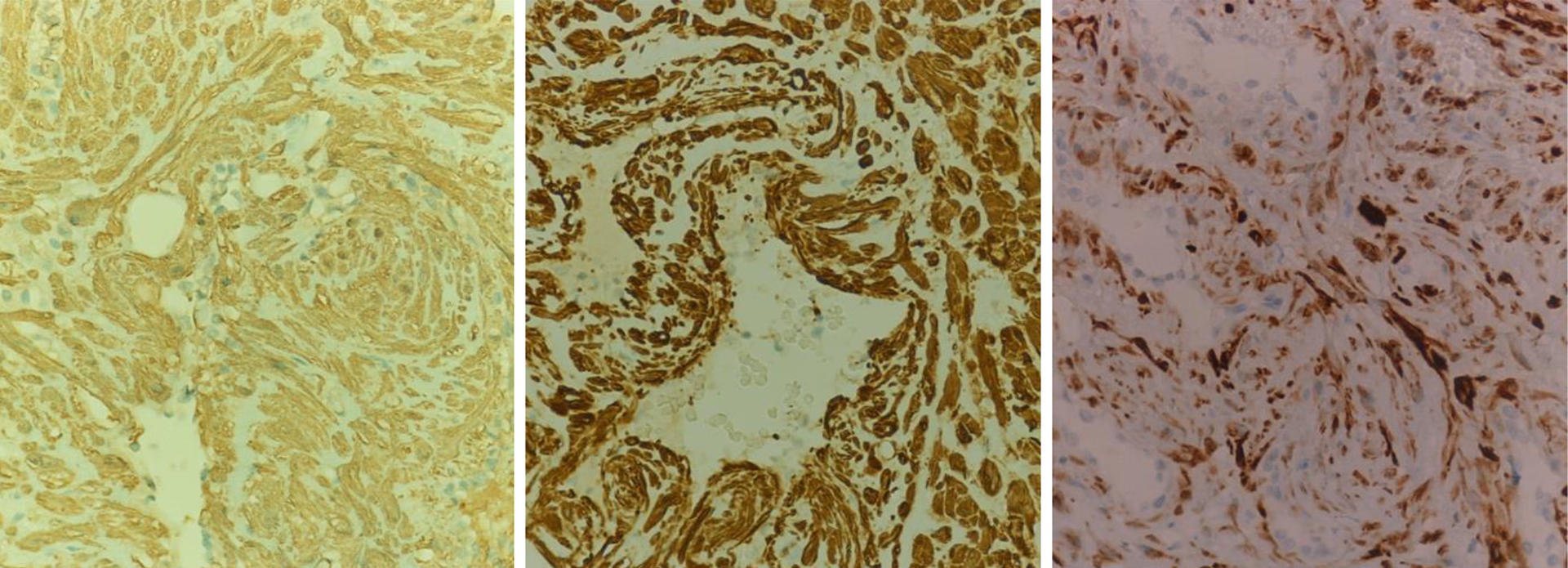
Immunohistochemical staining for smooth muscle actin (left), caldesmon (middle), and desmin (right) (immunoperoxidase-avidin-biotin complex; ×20).
The postoperative period was uneventful, the patient didn’t required a gastric nose tube feeding and was discharged the day after.
At 1 month follow-up schedule control, the postoperative site of the larynx was well recovered, the vocal folds mobility regained and the patient swallowing and quality of voice were thoroughly restored (Figure 6). Moreover, at 12 months control, the patient resulted clinically disease-free.
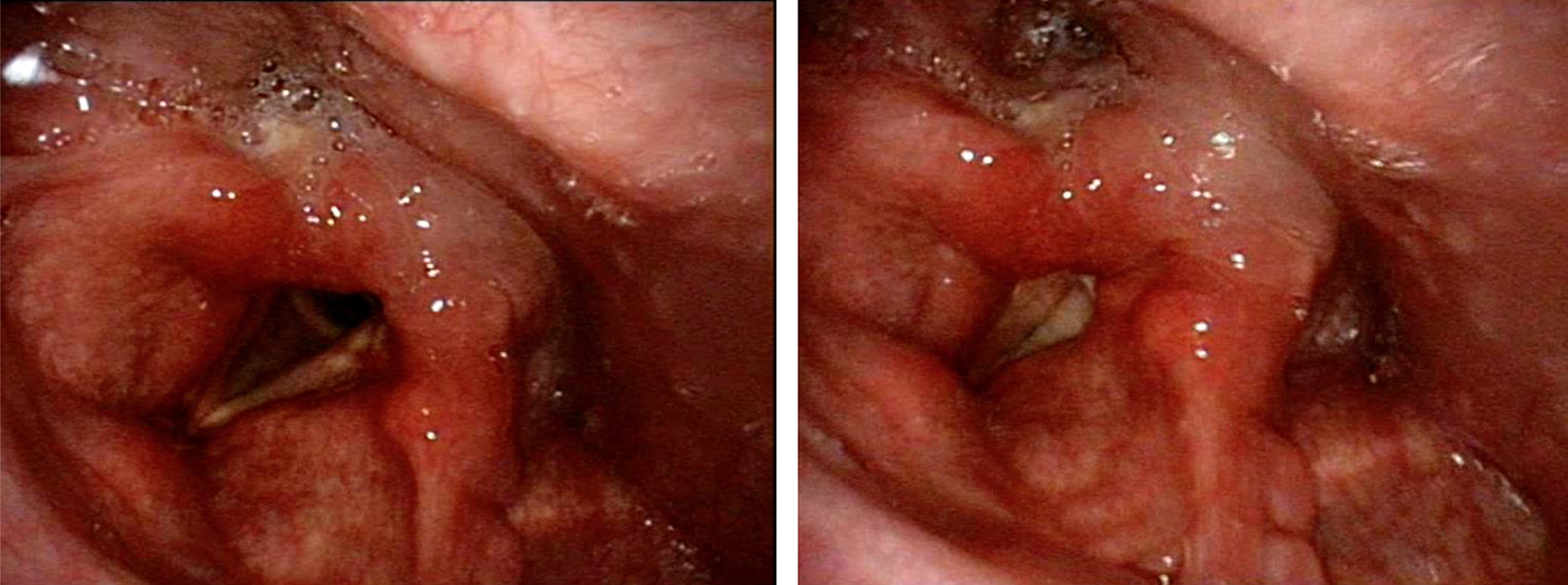
Endoscopic view of the laryngeal site at 1 month follow-up control.
Discussion
We performed an extensive Medline search of angioleiomyoma and vascular myoma in respect of laryngeal localization. The research was limited to the English literature and showed a limited numbers of case reports. Based on these findings, we present a case report with a review of the literature.
Angioleiomyoma or vascular leiomyoma is a benign vascular smooth muscle tumor. It can occur potentially everywhere in the body, but the most common sites are extremities’ skin (lower extremities 59% and upper extremities 15%), uterus, and gastrointestinal tract. 2,5
Head and neck localizations are exceptional, Wang et al analyzed a series of 160 patients treated for angioleiomyoma, of which 21 (13.1%) were found in head and neck, and none were localized in the larynx; the review revealed that the most frequent sites in the head and neck region are ear, lip, nose, and deep space of the neck, such as parotid space, submandibular space, carotid sheath, facial bone, and retropharyngeal space. 2
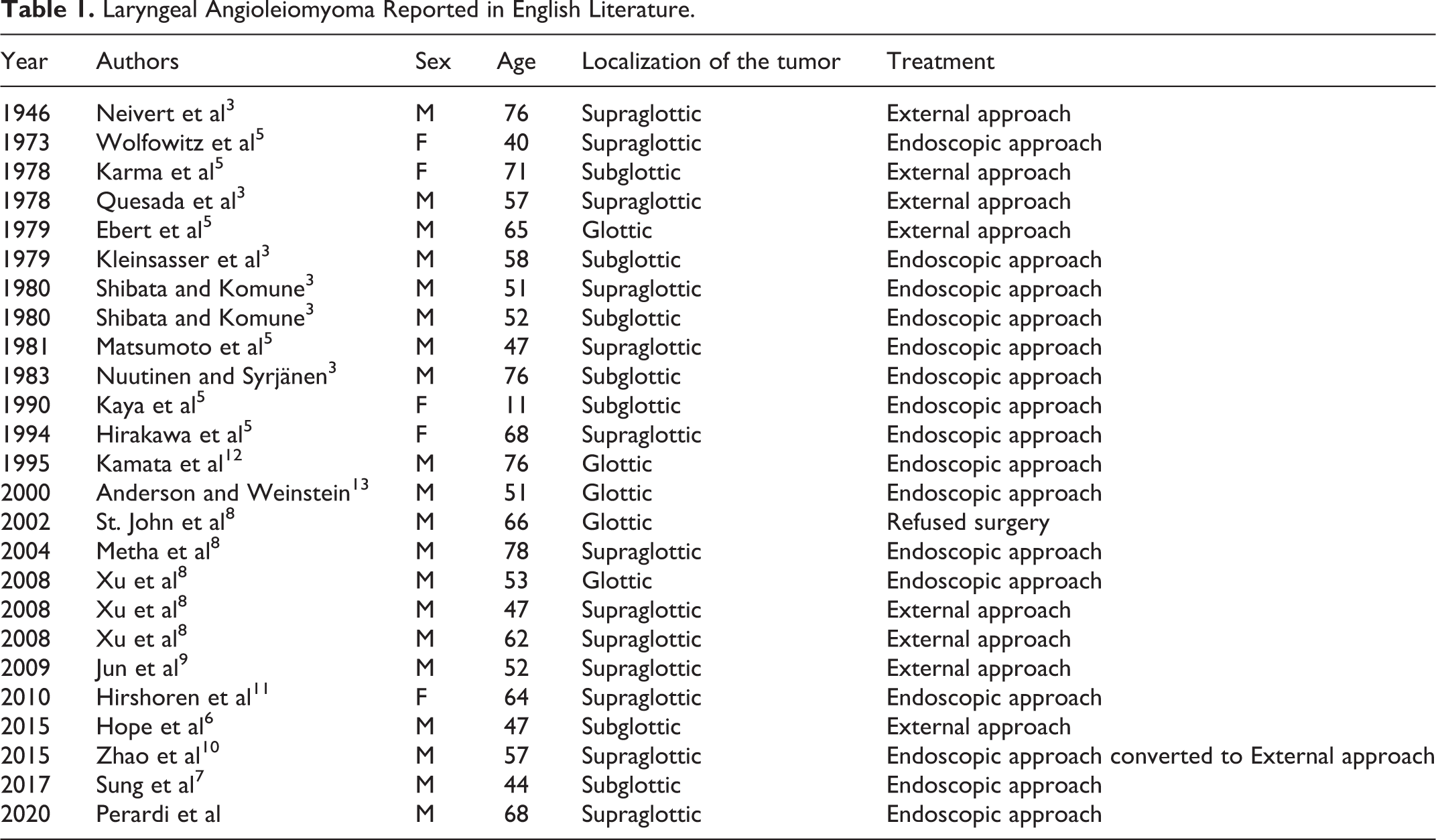
Until now, to the best of our knowledge, 24 cases of laryngeal angioleiomyoma were described in the literature. 3,6 -13 Among these reports, the most common laryngeal site is the supraglottic region with 50% of cases (12/24), followed by the subglottic region with 29.2% of cases (7/24), and glottic region with 20.8% of cases (5/24). Angioleiomyoma is more common in males than in females, the review of the literature showed that 79.2% of cases are male (19/24) and 20.8% are female (5/24), the range of age is 11 to 78 years with a mean age at diagnosis of 57 years (Table 1).
Laryngeal Angioleiomyoma Reported in English Literature.
From a histological point of view, angioleiomyoma is a benign tumor arising from the smooth muscle wall of blood vessels without elastic fibers. Macroscopically it presents as a firm, sharply circumscribed nodule, usually 2 cm or less, when localized in mucosal tissue it should be covered by normal mucosa or appear as a red wine nodule. Microscopically it shows ovoid and spindle smooth muscle cells arranged in variably intersecting boundless between slit-like vascular channels. Intermingled mature fatty elements can be observed too. Blood vessel endothelial cells may express pseudolipoblastic changes. Usually there is no mention of hemorrhage, necrosis, mitotic activity, vasculitis, or fibromuscular dysplasia.
The immunohistochemical examination normally reveals that the tumor cells are consistently and diffusely positive for a positive expression for alpha-smooth-muscle actin, desmin, myosin, trichrome, HHF35, calponin, and h-caldesmon; moreover also vimentin, type IV collagen, and S100 in small nerve fibers. 1
Morimoro et al in 1984 classified angioleiomyoma in 3 main histological subtypes: solid (closely compacted smooth muscle bundles), venous (vessels have thick muscular walls that merge with smooth muscle bundles), and cavernous (dilated vascular channels with minimal smooth muscle that merges with smooth muscle bundles). This classification has not any clinical significance; however, the histological and immunohistochemical examination is the only available instrument to obtain a correct diagnosis. 1,10 Our case was classified as a solid type angioleiomyoma positive for smooth muscle actin, caldesmon, and desmin.
The etiology of angioleiomyoma is unclear where some studies hypothesized the role of estrogen hormones with a mechanism similar to uterine myoma, however, other reports considered their role to be unlikely in myomas localized outside of the uterus. 10 The most common symptoms at the time of diagnosis are hoarseness, dysphagia, dyspnea, odynophagia, laryngeal pain, a sensation of a foreign body in the throat, cough, and hemoptysis. 7 -9 In our case, the patient presented with increasing dysphagia and hoarseness for 1 month without other symptoms.
Ear-Nose-Throat complete examination with flexible nasolaryngoscopy is mandatory for a correct characterization and localization of the mass. Preoperatively, CT and/or magnetic resonance imaging with contrast enhancement should be obtained to help in diagnosis and surgical plan identifying nature, vascularity, and extent of the lesion.
The complete surgical excision is still considered the gold-standard treatment for angioleiomyomas of any localization. Surgical modality options depend on some factors such as localization and size of the mass, risk of bleeding, and patient comorbidities.
The review of the literature demonstrated that among a total of 24 patients, 23 underwent surgical treatment, 13 (56.5%) underwent a pure endoscopic surgical excision, 10 (43.5%) underwent an external surgical procedure of them we have to mention that 1 patient was planned for endoscopic surgical plan; however, the treatment was converted in external approach due to the occurrence of profuse bleeding 6 -13 (Table 1).
In some cases, angiographic examinations should also be considered in lesions suspected to have a high bleeding risk in order to plan an embolization procedure or a sclerotherapy treatment before surgical excision preventing serious hemorrhage. 6,8,10 Still, there are not mentioned any cases of laryngeal angioleiomyoma’s embolization in the literature, infact, this technique has proven to be effective in this type of lesions in other sites, moreover, it could also be considered as a preliminary treatment in those cases when a transoral resection is indicated with a high predictable bleeding risk. 8 Hope et al described the unique laryngeal angioleiomyoma case in literature treated initially with sclerotherapy and subsequently with a successful surgical excision. 6
Improvements in instrumentation, technique, and surgeon’s experience in the last 2 decades permitted laryngomicrosurgey to be now considered a safe procedure for small and well-circumscribed laryngeal angioleiomyomas with advantages in minor tissue damage, better functional outcomes of speech, swallowing and pain control, reduction of hospitalization stay.
Never the less, there are still reports in the literature that described profuse bleeding during and after surgery or biopsy procedures. In 2000, Anderson and Weinstein presented a case of angioleiomyoma of the right vocal fold treated with CO2 laser technology resulting effective in reducing the risk of hemorrhage and better hemostasis outcome. 13 In our case, the lesion resulted less than 2 cm and well-circumscribed, therefore, based on radiological and clinical aspect, with strong suspicion of benign lesion, we planned a pure endoscopic approach with the use of CO2 laser technology that permitted a successful excision of the mass with rapid recovery in the absence of any intraoperative or postoperative bleeding.
When dealing with larger size tumors, the risk of profuse bleeding is greater; moreover, they can prevent a correct endoscopic field of view, in those cases, an external approach should be suggested. In this type of surgery, coagulating wounded surface with electrosurgical units demonstrate a reduction in intra and postoperative bleeding. 9,10
Recurrence of angioleiomyoma is a rare event, at the time of our review just 2 cases are described in the literature: the first case the tumor was diagnosed at the age of 39 and experienced the recurrence 12 years from surgery; the second case reports a recurrence in 12 years after a CO2 laser technology endoscopic debulking of the mass. 11,13 These reports suggest the importance of complete excision of the mass by a meticulous dissection along its capsule followed by ad appropriate endoscopic follow-up program. A malignant transformation of such tumor is considered to be an exceptional event and described in the literature in only 2 cases in the upper extremities. 10
Conclusions
Angioleiomyoma is a benign smooth muscle and vessel tumor, laryngeal localization is extremely rare. We describe a literature review upon this issue and, in particular, a case of angioleiomyoma of the pyriform sinus’s medial wall successfully treated in our centre with an endoscopic laser CO2 surgical excision. Our review shows that in most cases, including also our patient, this type of lesion can be successfully managed with an endoscopic approach. Based on our experience, the use of CO2 laser technology could also be suggested.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.