
Abstract
We describe a case of laryngeal angioleiomyoma, discuss its characteristic features and management, and provide a review of the literature, to improve clinical diagnosis and treatment. We report the oldest patient with a laryngeal angioleiomyoma to date and analyze the clinicopathological features reported in the literature. To the best of our knowledge, a total of 36 cases have been described in the English and Chinese medical literature (including our case). The male-to-female ratio was 5:1 and the mean age was 53.89 years. The most common laryngeal site was the supraglottic region (23 cases; 63.89%), followed by the subglottic region (8 cases; 22.22%), and glottis (5 cases; 13.89%). The most common and serious intra- and postoperative complication was massive bleeding. Angioleiomyoma is a benign tumor that rarely occurs in the larynx. Biopsy of this lesion should not be performed; complete surgical resection is the best treatment. Recurrence and malignant transformation are extremely rare.
Introduction
Angioleiomyoma (also known as vascular leiomyoma or angiomyoma) is a benign subcutaneous or deep dermal tumor consisting of well-differentiated smooth muscle and blood vessels. It frequently occurs in the uterus, extremities, skin, and gastrointestinal system, but is not common in the head and neck region, and is particularly rare in the larynx. 1 In view of the nature of this disease, and to improve clinical diagnosis and treatment, we present a case of angioleiomyoma of the epiglottis, together with a literature review. The patient is an 84-year-old female who, to the best of our knowledge, is the oldest patient with laryngeal angioleiomyoma reported to date.
Case Presentation
In March 2017, an 84-year-old female presented to the Department of Otolaryngology, The First Affiliated Hospital, College of Medicine, Zhejiang University (Hangzhou, China), with a 6-month history of pharyngeal discomfort, and the sensation of a pharyngeal foreign body, odynophagia, and muffled speech for the past 2 months. The patient experienced no expectoration, dysphagia, dyspnea, hoarseness, chest congestion, postnasal drip, or fever. She was a nonsmoker and nondrinker. The patient had a history of hypertension for 40 years, which was well-controlled by medication. She also had a history of a sleep disorder for 8 years, generally controlled by medication. In addition, she had a history of cerebral infarction 8 years prior, causing on 1 side of the body, but had no remaining neurological dysfunction after hospitalization. The medical history was otherwise uneventful.
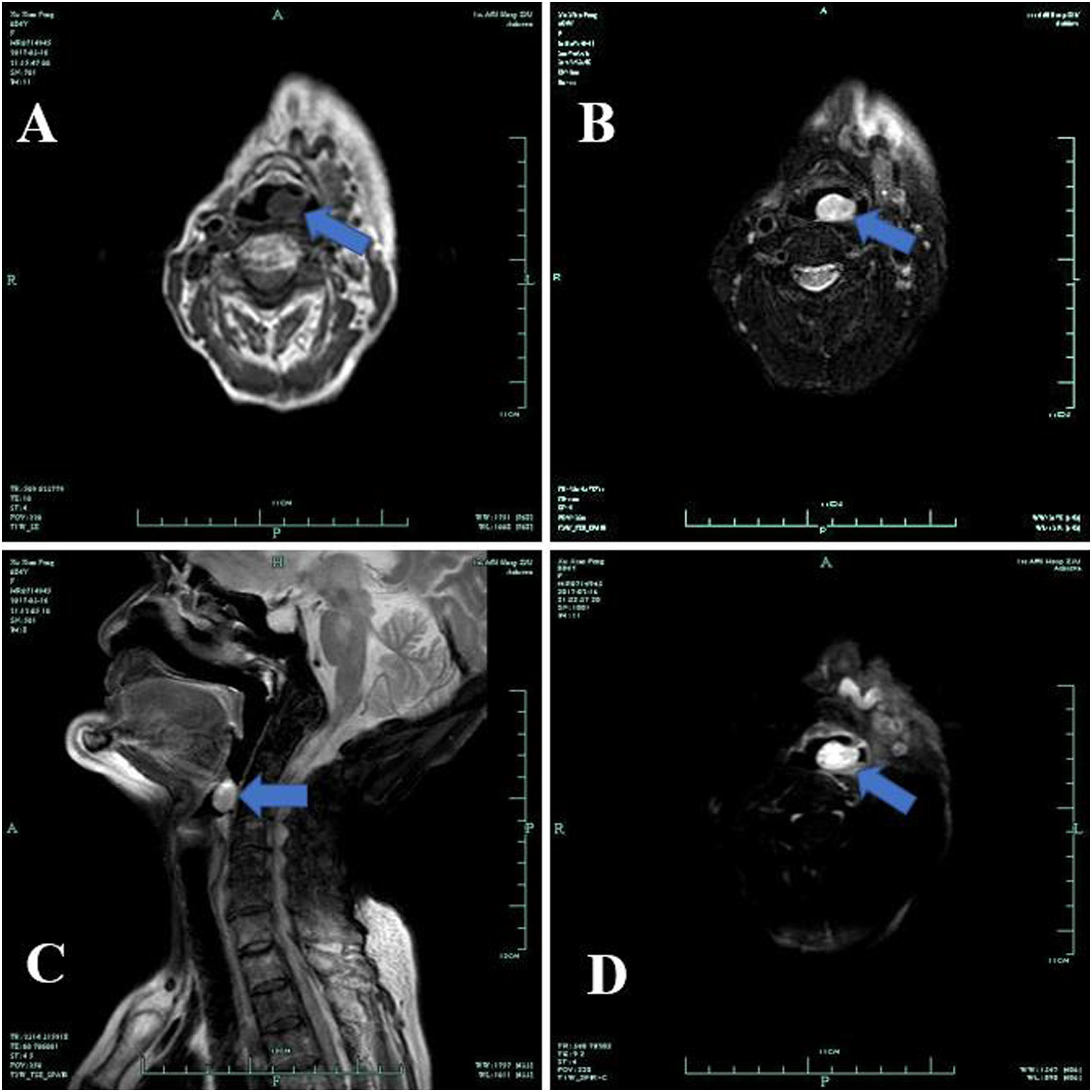
Physical examination revealed no abnormalities within the nasopharynx, tongue, hypopharynx, or interior laryngeal and cervical lymph nodes. Laryngostroboscopy examination revealed a smooth, dark red mass measuring approximately 2.0 × 1.5 cm on a broad pedicle, located at the margin of the epiglottis on the left side [Figure 1]. No dilated vessels were observed on the tumor surface. This appearance mimicked that of an epiglottic hemangioma. Magnetic resonance imaging (MRI) with contrast enhancement of the head and neck revealed an elliptical abnormal signal lesion with clear boundaries, long T1 and T2 signals, and obvious homogenous enhancement [Figure 2]. In view of her prior history of cerebral infarction, color doppler ultrasonography of intracranial and cervical vessels and cranial MRI were performed to evaluate her condition. After consultation, the neurologist concluded that there was no absolute contraindication for surgery. Laryngostroboscopy showed a smooth, dark red, broad pedicle, measuring approximately 2.0 × 1.5 cm mass located on the margin of the epiglottis on the left side. MRI with contrast enhancement revealed an elliptic abnormal signal lesion with clear boundaries (arrow), showing long T1 (A) and long T2 (B, C) signals, and the enhanced scanning was obvious and homogenous (D).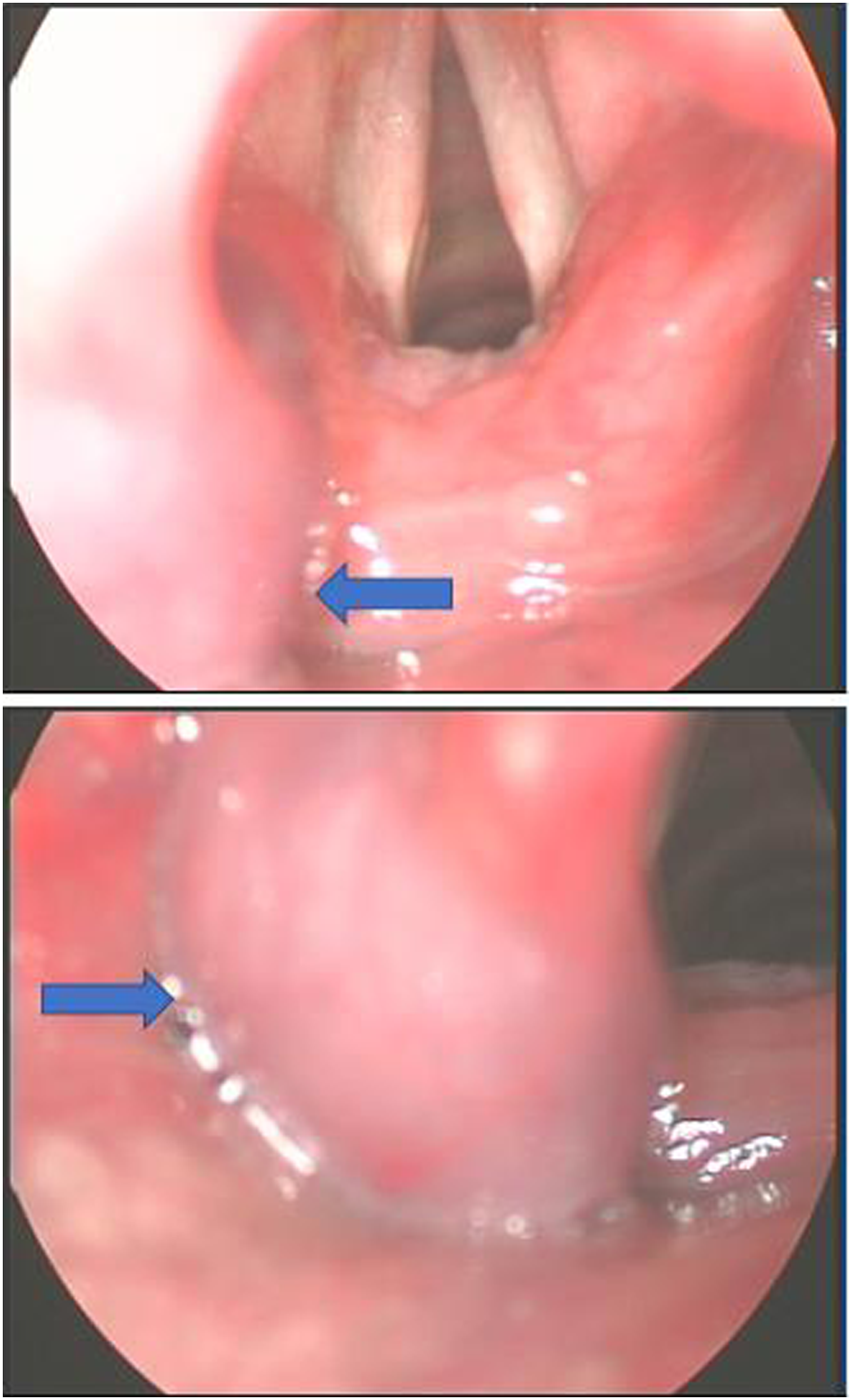
The epiglottic tumor was excised through suspension laryngoscopy under general anesthesia. The lesion was located at the margin of the epiglottis on the left side and was wholly resected without significant bleeding or any other complications. Intraoperative frozen section examination revealed a spindle cell tumor of the epiglottis, and angioleiomyoma could not be excluded. Postoperative histopathological examination showed that the lesion consisted of well-differentiated spindle smooth muscle cells with rich vascular channels of thick vessel walls [Figure 3A]. Immunohistochemically, the tumor cells were positive for CD31, CD34, desmin, and SMA and negative for S-100 [Figures 3B–3F]. According to these histological data, the tumor was finally diagnosed as an angioleiomyoma. Histopathological findings showing the mass consisted of well-differentiated spindle smooth muscle cells with intervening rich vascular channels of thick vessel walls (A). The vascular network is demonstrated by positive immunostaining for CD31 (B) and CD34 (C). The smooth muscle cells are demonstrated by positive immunostaining for desmin (D), SMA (E), and negative for S-100 (F).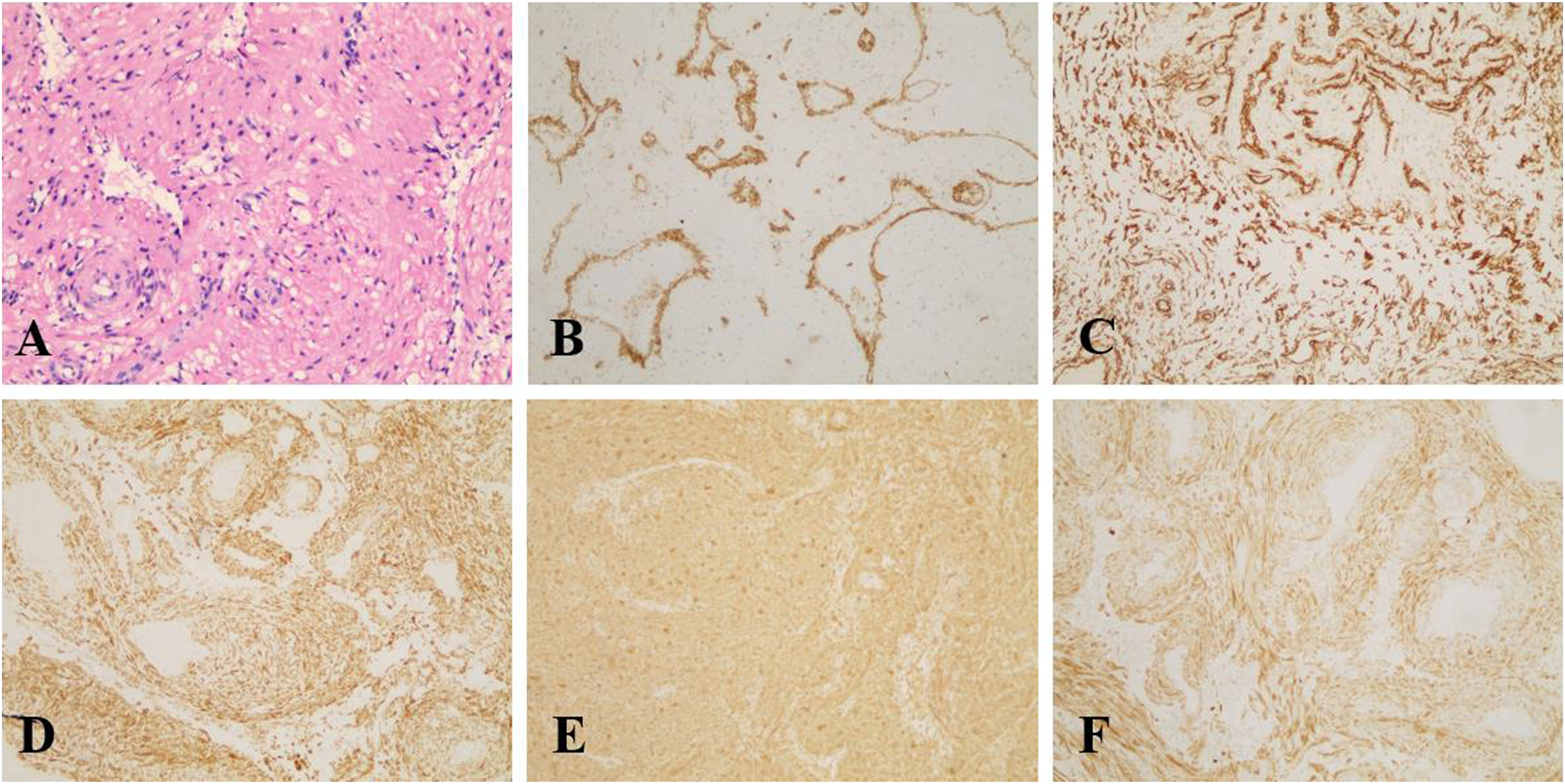
The patient recovered well after surgery and her preoperative symptoms all disappeared, except for residual mild pharyngodynia. She was discharged on the third day after surgery and her sore throat also quickly disappeared. No recurrence or malignant transformation has been found during the 5-year follow-up.
Discussion
We reviewed the English medical literature in the MEDLINE database. With respect to laryngeal localization, the extensive search used the terms “angioleiomyoma” OR “vascular leiomyoma” OR “angiomyoma” AND “larynx.” Articles published in Chinese journals were identified by searching the Wanfang (http://www.wanfangdata.com.cn), CNKI (China National Knowledge Infrastructure: http://www.cnki.net/), and Weipu (http://lib.cqvip.com/) databases.
To the best of our knowledge, a total of 20 cases of laryngeal angioleiomyoma have been described in the English medical literature (including our case).2–17 The review showed that laryngeal angioleiomyoma is more common in males (15 cases) than females (5 cases), with a male-to-female ratio of 3:1. The patients ranged in age from 11 to 84 years at the initial consultation, with a mean age of 56.8 years. The symptoms of these patients were well-documented; 10 (50%) presented with hoarseness, 9 (45%) with dyspnea, 4 (20%) with dysphagia, 6 (30%) with the sensation of a foreign body in the throat, and 4 (20%) with throat pain. Other symptoms included stridor, cough, hemoptysis, and muffled speech. These symptoms mainly related to the part of the larynx affected by the tumor. Among the 20 cases of laryngeal angioleiomyoma, the most common laryngeal site was the supraglottic region (11 cases; 55%), followed by the subglottic region (6 cases; 30%) and glottis (3 cases; 15%). Our patient presented with pharyngeal discomfort, the sensation of a pharyngeal foreign body, odynophagia, and muffled speech. Pharyngeal discomfort and the sensation of a pharyngeal foreign body could be related to the mass affecting the area surrounding the pharynx; in our patient, the tumor was on the epiglottis, very close to the pharynx. Odynophagia is common, and angioleiomyomas of the skin frequently causes pain in the lesion; this may be related to the effect of the mass on the nerves. In our case, the tumor was on the epiglottis, so the patient did not experience hoarseness but presented with muffled speech.
In the Chinese medical literature, a total of 16 cases of laryngeal angioleiomyoma have been reported.18-32 One case was reported in both the Chinese and English medical literature.12,33 A review of the Chinese literature showed that 15 cases were male (93.75%), and only 1 was female (6.25%), for a male-to-female ratio of 15:1. The age range was 24–78 years, with a mean age at a diagnosis of 50.25 years. Among 16 cases of laryngeal angioleiomyoma, 12 (75%) occurred in the supraglottic region, 2 (12.5%) in the subglottic region, and 2 (12.5%) in the glottis.
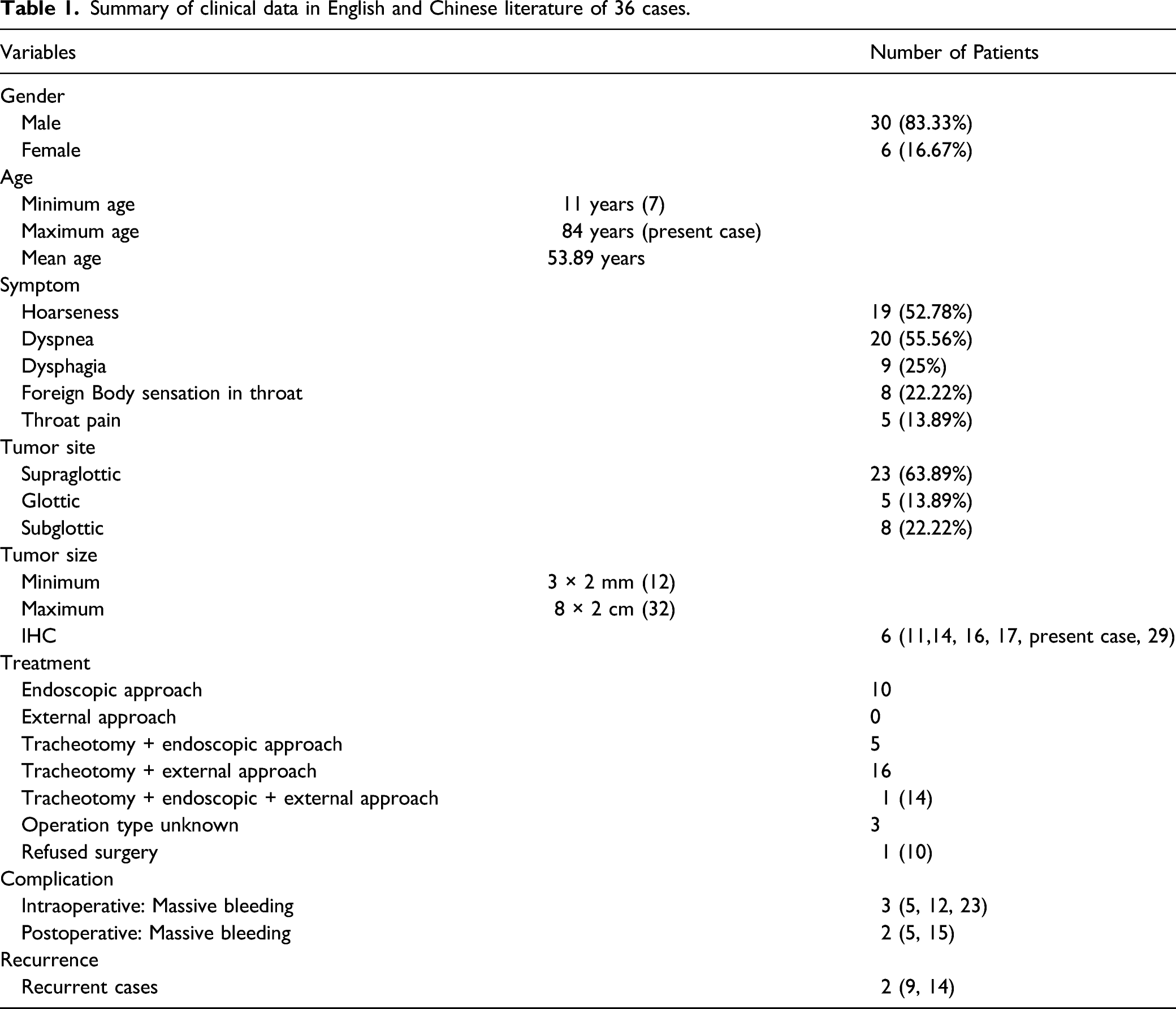
Summary of clinical data in English and Chinese literature of 36 cases.
Most laryngeal angioleiomyomas are smooth, pedicled, and red, dark red, light red, pink, purple, or gray-red in color, with or without superficial blood vessels, and their appearance sometimes mimics a laryngeal hemangioma. Our case presented with a smooth, dark red mass located at the margin of the epiglottis on the left side, which led to the initial diagnosis of epiglottic hemangioma. However, on careful examination, most laryngeal hemangiomas have uneven surfaces and irregular shapes, which can help distinguish them from laryngeal angioleiomyoma.
The etiology of angioleiomyoma formation is still unclear. Histopathologically, an angioleiomyoma is a benign spindle cell tumor arising from the smooth muscle cells of blood vessel walls, which is composed of well-differentiated smooth muscle bundles and numerous variform blood vessels, and lacks mitosis.1,12-14 Whorls of smooth muscle fibers are observed surrounding the blood vessel endothelium, sometimes with mucoid changes. 12 Immunohistochemical examination also plays an important role in the diagnosis of vascular leiomyoma. Diffuse alpha-smooth muscle actin, desmin, myosin, trichrome, HHF35, calponin, and h-Caldesmon are consistently seen in the tumor cells. 1 The expression of desmin and α-actin smooth muscle antibodies confirmed the presence of smooth muscle cells, while the expression of CD34 and CD31 verified the presence of vascular endothelium. 16 A total of 6 case reports (including ours) provided immunohistochemical results (Table 1). The immunohistochemical examination of our case revealed SMA(+), desmin(+), CD31(+), and CD34(+) in tumor cells, in accordance with the immunohistochemical findings of previous studies of angioleiomyoma patients.
The optimal treatment for angioleiomyoma is complete surgical excision. The best surgical option depends on many factors, such as the localization and size of the tumor, morphology, risk of bleeding, and patient comorbidities. Some small tumors can be resected through endoscopic surgery under direct laryngoscopy or suspension laryngoscopy, which have the advantages of less invasion, more rapid recovery, better functional results in terms of the voice, swallowing, breathing, and shorter hospital stays, whereas larger tumors or anticipated massive bleeding may require an external approach such as laryngofissure or lateral pharyngotomy.1,10,12,13,16 If the patient has severe dyspnea or a high risk of anesthetic intubation, tracheotomy may be necessary. In our case, the tumor (located at the margin of the epiglottis) was not > 2 cm, and was smooth and well-circumscribed, with no dilated blood vessels on the surface. Therefore, the radiological and clinical data indicated a high probability that it was a benign and confined tumor. Finally, we used an endoscopic approach under suspension laryngoscopy that permitted complete excision of the tumor, and rapid recovery without intra- or postoperative complications.
Regarding the other treatments for laryngeal angioleiomyoma, carbon dioxide laser, YAG laser, semiconductor laser, cryotherapy, and bleomycin injection have also achieved good outcomes.6,11,12,14,15,24,32
Due to the rich blood supply of angioleiomyomas, the most common and serious intra- and postoperative complication is massive bleeding. Shibata et al. reported 2 cases of laryngeal angioleiomyoma resected through laryngomicrosurgery. One patient had 600 mL of intraoperative bleeding and the other had 1000 mL of postoperative bleeding. 5 We previously reported a case of epiglottic angioleiomyoma with 300 mL of bleeding after biopsy at another hospital; that patient required emergency tracheostomy and local hemostasis, followed by transfer to our department. Three days after being transferred, there was a further 500 mL of sudden bleeding, requiring an emergency lateral neck incision and tumor resection. 12 This suggests that any smooth red mass found in the larynx by indirect laryngoscopy should be considered a vascular tumor, and no biopsy should be undertaken due to the risk of hemorrhage.
Recurrence of angioleiomyoma is rare. To date, only 2 cases of recurrent laryngeal angioleiomyoma have been reported in the literature.9,14 Therefore, complete resection of the tumor along the capsule is important. Malignant transformation of angioleiomyoma is highly unlikely, and no malignant laryngeal angioleiomyoma has been reported to date. Patients should be regularly followed up for recurrence after surgery.
In conclusion, angioleiomyoma is a benign tumor that rarely occurs in the larynx. We report a case of epiglottic angioleiomyoma and reviewed the literature for clinicopathological features. This type of tumor has an abundant blood supply, and biopsy should not be performed; complete surgical resection is the best treatment. Although recurrence and malignant transformation of laryngeal angioleiomyoma are rare, close long-term follow-up is still recommended.
Footnotes
Acknowledgments
We would like to thank for the support by Zhejiang Province Public Welfare Technology Application Research Project (No. LGF19H180018) and Scientific Research Fund of Zhejiang Provincial Education Department (NO. Y202045601). All authors contributed to the article and approved the submitted version.
Author Contributions
BYY and SXJ designed and wrote the manuscript. DLB reviewed the references and made the Figures. GY made the tables. YHT made the immunohistochemical pictures. ZSH analysis of the data, revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Zhejiang Province Public Welfare Technology Application Research Project (No. LGF19H180018) and Scientific Research Fund of Zhejiang Provincial Education Department (NO. Y202045601).
Informed Consent Statement
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.