
Abstract
Introduction:
The recurrent laryngeal nerve gains its name because after branching from the vagus nerve, it turns superiorly (recur) around the subclavian artery on the right and around the ligamentum arteriosum on the left, the nonrecurrent nerve has a straight direct course to the larynx and doesn’t follow this course. It presents mostly on the right side. The presence of this variation places the nerve at higher risk of injury during neck surgery especially thyroid operations.
Case Presentation:
A 45-year-old lady presented with painless thyroid enlargement for 1 year. Thyroid examination showed a 3-cm firm nodule at the right thyroid lobe with normal thyroid function tests. Right thyroid lobectomy was done and the histopathology showed a benign follicular lesion. During surgery, we discovered 2 nonrecurrent laryngeal nerves at the right side which were arising from the vagus nerve and both were entering the larynx.
Conclusion:
Failure in identification of the nerve or overlooking the possibility of the non-recurrent laryngeal nerve may result in a serious sequelae of nerve damage, ipsilateral injury may lead to permanent hoarseness and bilateral injury may result in severe dyspnea or aphonia. Currently, there are 3 types of nonrecurrent laryngeal nerve courses. Type 1 passes near to the superior thyroid vessels. Type 2 (2A) passes parallel to the inferior thyroid artery and has a transverse course above it. Type 3 (2B) passes parallel to the inferior thyroid artery and transversely between branches of or under the inferior thyroid artery, we can add to this classification type 4, which are 2 nonrecurrent laryngeal nerves (double nerves) passing above and parallel to the inferior thyroid artery.
Keywords
Introduction
The recurrent laryngeal nerve gains its name because, after branching from the vagus nerve, it turns superiorly (recur) around the subclavian artery on the right side and around the ligamentum arteriosum on the left side, while the nonrecurrent one doesn’t follow this course instead it arises from the vagus nerve in the neck and have a straight direct course to the larynx. It innervates the intrinsic laryngeal muscles except the cricothyroid muscle which is innervated by the external laryngeal nerve. 1
This anomaly was first noticed in 1823 by Steadman when he was doing a cadaveric dissection, he also noticed an anomalous origin and course of the right subclavian artery. 2
Nonrecurrent laryngeal nerve is a rare anatomical variation that present mostly on the right side, its estimated percentages are around 0.3% to 0.7%; in the left side this variation is extremely rare, estimated to be around 0.04%. Studies have shown a significant difference during cadaveric dissection, being twice more common.3,4
This variation is usually associated with an aberrant right subclavian artery in around 85% of cases. 3 Preservation of this nerve during surgery is of utmost clinical importance that will prevent the morbidity and the disastrous sequelae of nerve injury. The presence of this variation places the nerve at higher risk of injury during neck surgery especially thyroid operations.
Patient Information
A 45-year-old lady presented with painless thyroid enlargement for 1 year. The patient had no history of weight changes or voice changes. The past medical and surgical histories were negative.
Clinical Findings
General examination showed normal vital signs and no any extra-thyroid signs, and the patient had no signs of hyper or hypothyroidism. Thyroid examination showed a 3-cm firm nodule at the right thyroid lobe.
Diagnostic Assessment
During workup, the thyroid function tests were normal, histopathological sample from the thyroid nodule by fine needle aspiration cytology showed follicular lesion.
Therapeutic Intervention
Decision was done for surgery, and right thyroid lobectomy and isthmusectomy were performed, i.e. ligation of the middle thyroid vein was done then ligation of the superior thyroid artery was done, identification of the inferior thyroid artery was done, then we searched for the recurrent laryngeal nerve at the tracheo–esophageal groove and was not identifiable at the normal anatomical site, searching of nonrecurrent laryngeal nerve was done, and surprisingly, we identified 2 nonrecurrent laryngeal nerves which were arising from the vagus nerve, their course was above and parallel to the inferior thyroid artery, both nerves entered the larynx. The frozen section examination showed a benign follicular lesion (Figures 1 and 2).
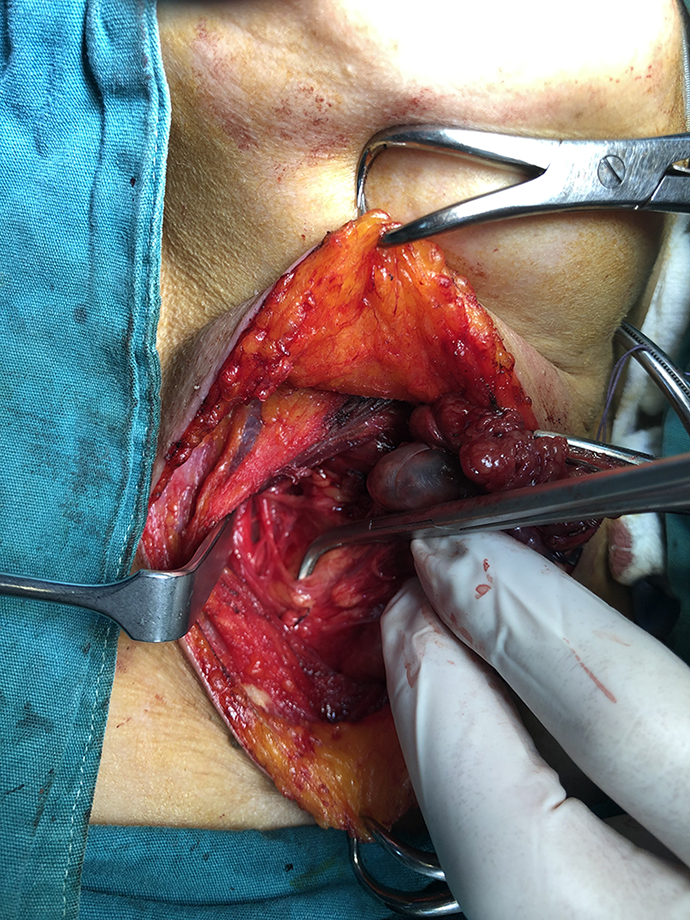
An intraoperative picture showing the double right nonrecurrent laryngeal nerves and the inferior thyroid artery marked with the right angle forceps.
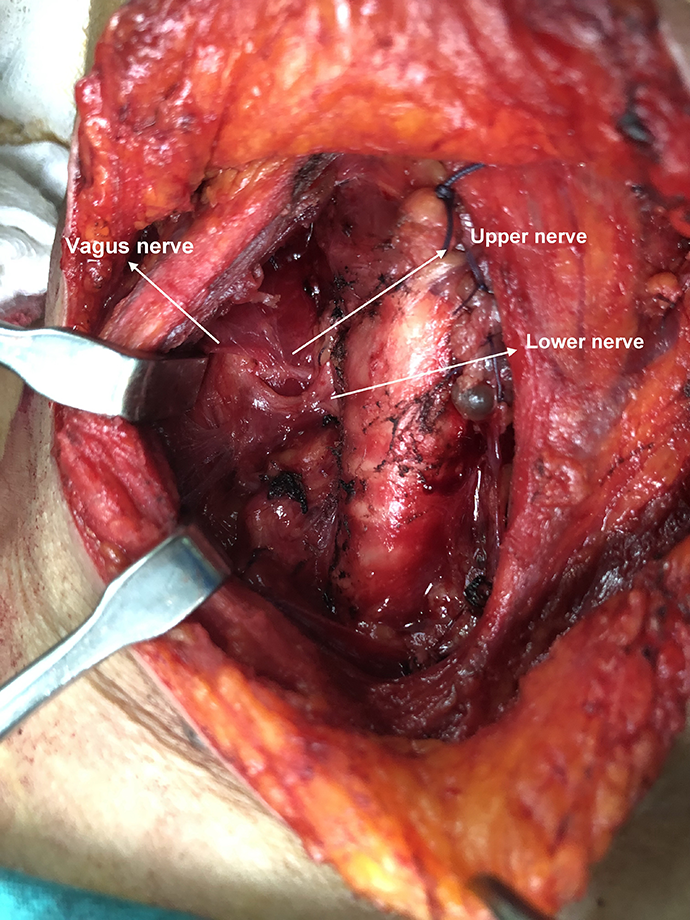
An intraoperative picture showing the double right nonrecurrent laryngeal nerves, marked as the upper and the lower nerves.
Follow-Up and Outcomes
After surgery, the patient was admitted for 3 days and she was discharged home with no postoperative complications.
Discussion
There are 3 types of nonrecurrent laryngeal nerve courses. Type 1 passes near the superior thyroid vessels. Type 2 (2A) passes parallel to the inferior thyroid artery and has a transverse course above it. Type 3 (2B) passes parallel to the inferior thyroid artery, and transversely between branches or under the inferior thyroid artery. We can add to this classification type 4 course, which are 2 nonrecurrent laryngeal nerves (double nerves) passing above and parallel to the inferior thyroid artery. 5
This anomaly could be suspected clinically preoperatively in patients with situs inversus and patients with dysphagia lusoria which is caused by an aberrant retro-oesophageal subclavian artery in the right side. 6 It may also be suspected after doing different imaging modalities, such as barium swallow, preoperative ultrasound of the neck, and computed tomography scan of the neck and chest which showed associated vascular anomalies.7-9
Intraoperatively, the course of the nerve is searched in the trache0-esophageal groove after identification of the inferior thyroid artery and applying some lateral traction over it because it is closely related to the artery, failure of identification should raise the possibility of this anomaly, in such situation, some authors recommend doing an orderly dissection, starting by careful identification and mobilization of the vagus nerve before proceeding to do thyroidectomy which may enable the surgeon in identifying the nerve, it may also be detected intraoperatively by intraoperative nerve monitoring.6,10,11
Failure in identification of the nerve or overlooking the possibility of the nonrecurrent laryngeal nerve may result in serious sequelae of nerve damage, ipsilateral injury may lead to permanent hoarseness and bilateral injury may result in severe dyspnea or aphonia. 4
Footnotes
Authors’ Note
An informed consent was taken from the patient to report the case and the accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.