
Abstract
Objective:
To study terminal bifurcation of recurrent laryngeal nerves (RLNs) with original direction to larynx entry and to decrease the risk of vocal cord paralysis in thyroid patients.
Methods:
The RLNs of 294 patients (482 sides) were dissected according to the branches into the larynx, and the original direction of each RLN trunk in thyroid surgery was recorded.
Results:
(1) About 30.9% of the RLNs gave off multiple branches into the larynx. (2) Two and 3 branches of RLNs into the larynx were found in 25.5% and 5.4% of the cases, respectively. (3) In 0.4% or 2 cases, the RLN trunk combined with the inferior branch of the vagus nerve. (4) Nonrecurrent laryngeal nerve appeared in 2 cases. (5) On the left side, 68.0%, 25.6%, and 6.4% of cases were found with 1, 2, and 3 bifurcations of RLN to larynx entry, respectively. On the right side, 69.8%, 25.8%, and 4.4% cases were identified with 1, 2, and 3 bifurcations of RLN to larynx entry, respectively. (6) The combining dissection approach was proved as successful and safe for protecting the RLN with no permanent RLN paresis.
Conclusions:
Because of the anatomical variation in RLNs with extralaryngeal bifurcation, it is necessary to increase the awareness of surgeons about these variations so as to protect bifurcated nerves in thyroid surgery.
Keywords
Introduction
Vocal cord paralysis caused by recurrent laryngeal nerve (RLN) injury is a not uncommon occurrence after thyroid surgeries, with recent series quoting rates of transient paralysis up to 5% to 10%. 1 Thus, consideration and recognition of every variation is essential to minimizing the rate of RLN injury during thyroid surgery. 2 American Thyroid Association Guidelines recommended in 2015 that RLNs should be identified during dissection in thyroid operation. 3 Bifurcation, a well-known variation in RLN, should be fully identified and preserved integral by surgical dissection for preventing this complication. The 3 main identification approaches for RLN dissection include the lateral, inferior, and superior approaches. 4 Surgeons should know the variations in RLN topography and the technique for preserving trunk and terminal branches of RLN, so as to decrease the risk and enhance the safety of thyroid surgery. 5 In the present study, we attempted to identify and dissect bifurcated branches of laryngeal nerves in 294 Chinese thyroid patients and to anatomically characterize RLNs based on their original directions and extralaryngeal branches to the larynx.
Materials and Methods
We performed 294 thyroid operations at the Yangtze University Hospital, Jingzhou, China, between January 2016 and August 2019 (total thyroidectomy: n = 161; subtotal thyroidectomy: n = 42; right lobectomy: n = 51; left lobectomy: n = 40). The study was approved by our ethics committee of The First Affiliated Hospital, School of Medicine, Yangtza University. Each patient received laryngoscopy before surgery (Table 1). We obtained informed consent from every patient before the surgery and institutional approval in use of examination data for research purpose. The original direction and bifurcation number of each RLN to the larynx were macroscopically determined and recorded. The inclusion criteria were as follows: surgical thyroid diseases, including thyroid cancer, solitar adenoma, or multinodular goiter. The exclusion criteria were as follows: vocal cord impairment before surgery or neck radiation. Standard dissections of RLNs under general anesthesia were performed by the same surgical team. Main parameters were the anatomical characteristics and incidence of RLN original direction and terminal bifurcation number to larynx. All RLNs were identified during operations, and data were recorded when the RLNs were exposed.
Patients’ Information and RLN Identified.
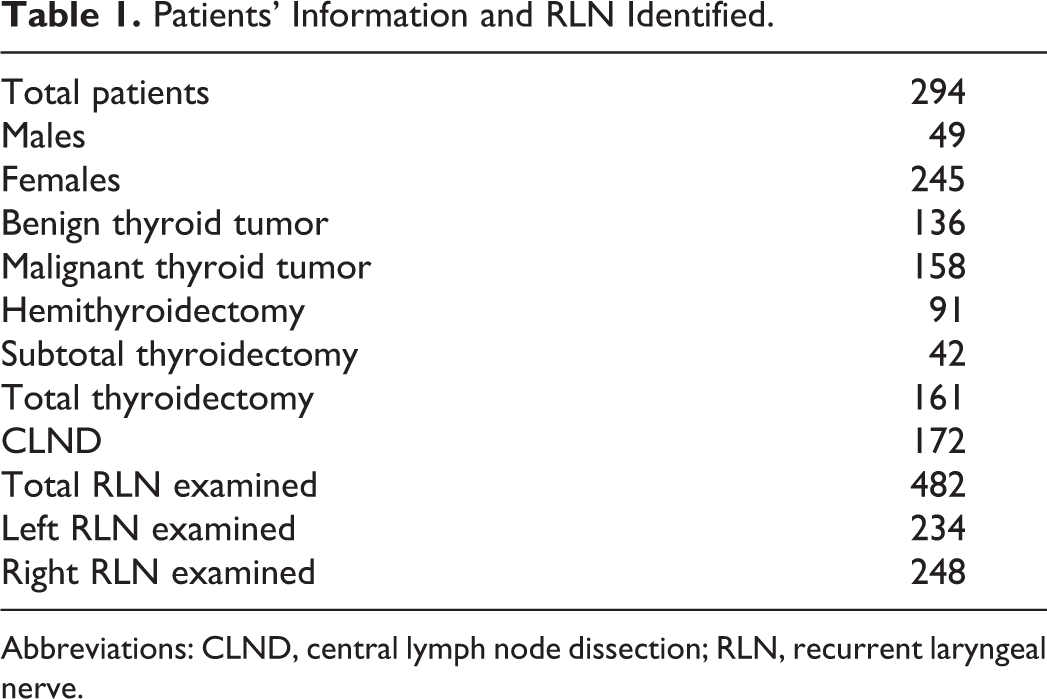
Abbreviations: CLND, central lymph node dissection; RLN, recurrent laryngeal nerve.
Intraoperative Dissection of RLNs
After the sternothyroid muscle was isolated from the thyroid gland in each case, the isthmus was transected and freed to the Berry ligament level along the lateral trachea side. The superior branches of thyroid gland artery/vein were ligated and Berry’s ligament was divided through the cricothyroid space. The cephalad branch of the vagus nerves below the superior thyroid gland was identified with the superior approach. The inferior branches of thyroid gland artery/vein were ligated and dissected separately. With the inferior approach, the RLNs trunks in the tracheaesophageal groove (TEG) were identified. The middle branches of thyroid gland artery/vein were ligated and dissected separately. The nerves with terminal bifurcations were carefully exposed and dissected meticulously from connective structures, Berry ligament and Zuckerkandl tubercle, up to the laryngeal entry point. Operative data including the original direction of RLNs and the terminal branch number to larynx entry were obtained prospectively in the macroscopy.
Terminal Branches of RLNs to Laryngeal Entry
Bifurcation of RLN occurred along its cervical trunk to larynx. The 2 or 3 RLN branches to larynx entry were observed separately during operation.
Types of Anatomical Variations in RLNs
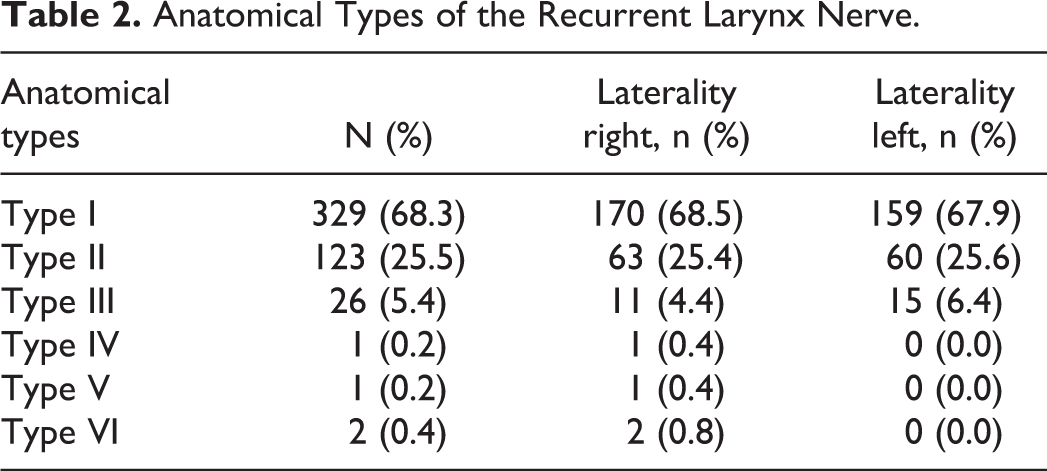
The types of RLN variations were classified according to the original direction of each RLN and its terminal branches into the larynx. The laryngeal entry point and the original direction of each RLN were relatively constant landmarks. Totally 6 types of RLN variations were observed in our operations (Table 2 and Figures 1–6).
Type I: Only 1 RLN branch was observed up to the laryngeal entry point in the TEG (Figure 1);
Type II: Two RLN branches were observed separately up to the laryngeal entry point in the TEG (Figure 2);
Type III: Three RLN branches were observed separately up to the laryngeal entry point in the TEG (Figure 3);
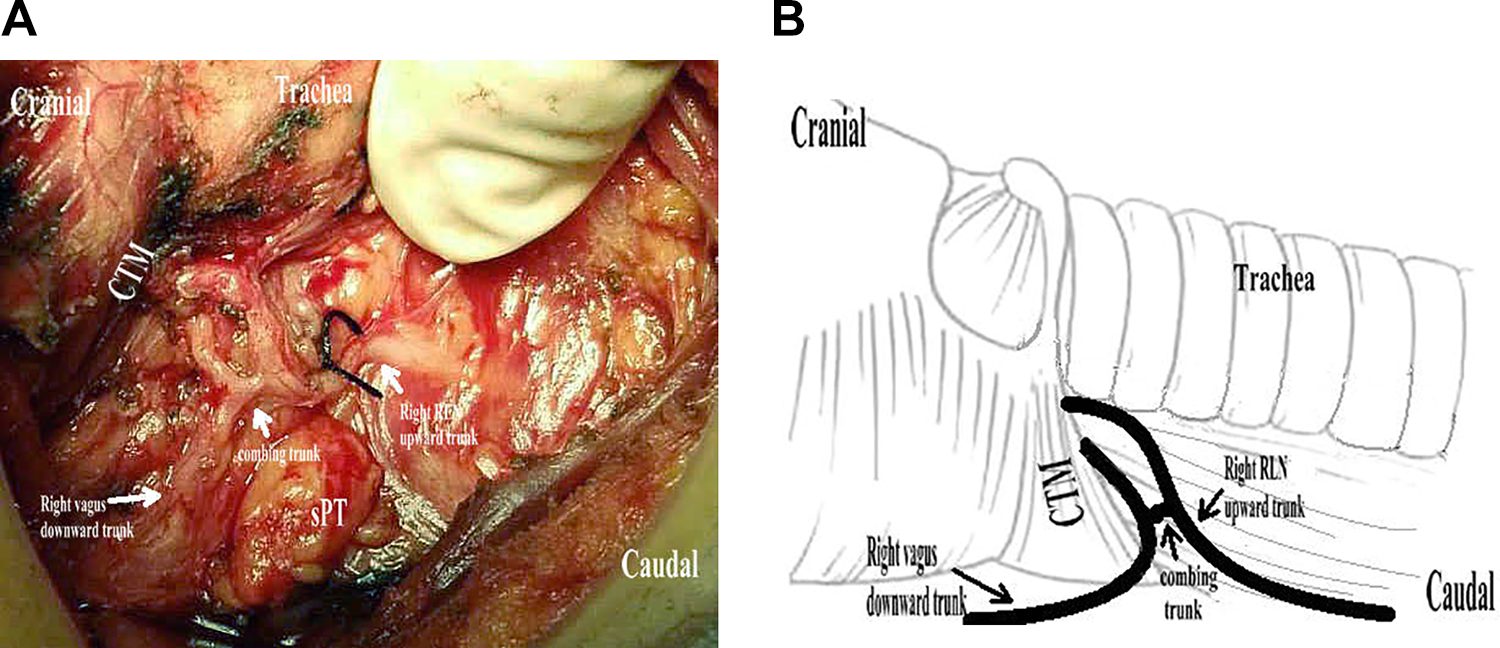
Type IV: Only 1 combining branch of vagus nerve and RLN was observed up to the laryngeal entry point (Figure 4);
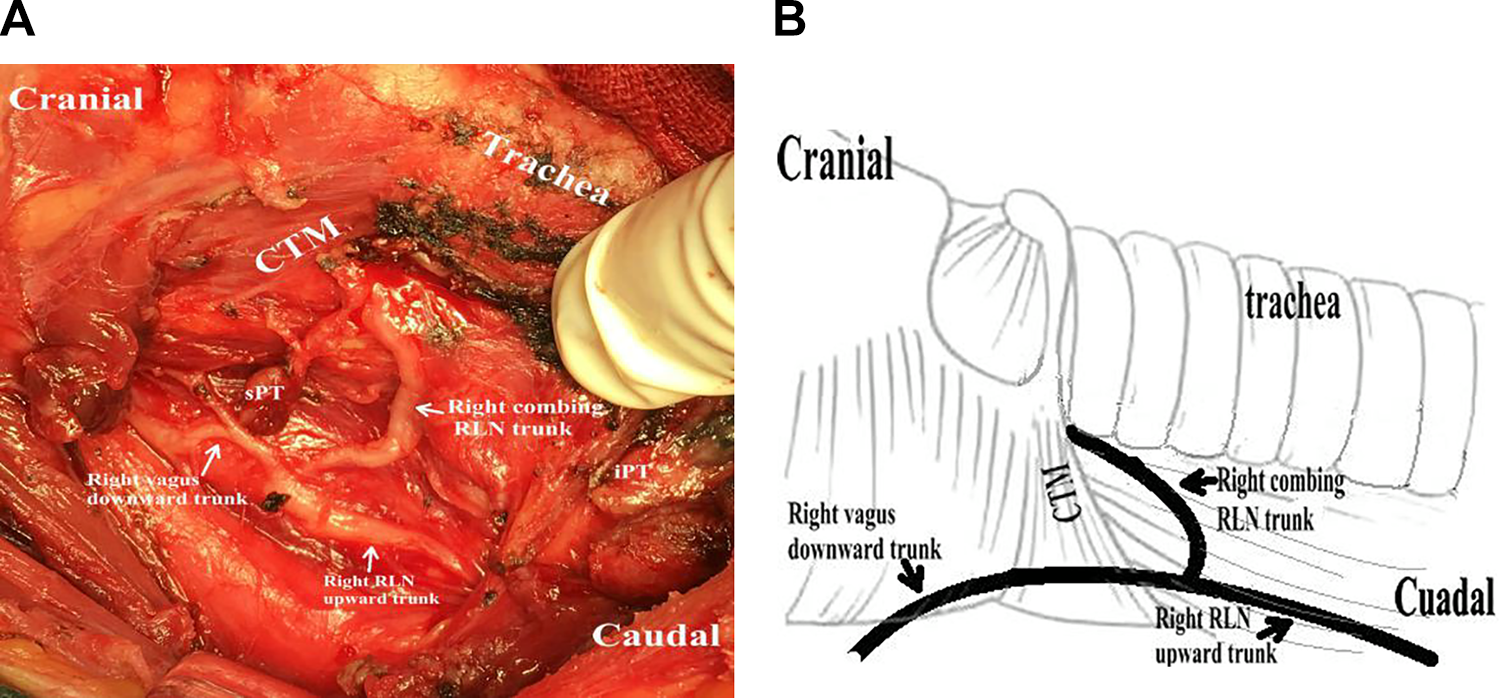
Type V: Two combining branches of vagus nerve and RLN were observed up to the laryngeal entry point (Figure 5);
Type VI: The nerve trunk passed from the vagus nerve up into the larynx entry, namely the nonrecurrent laryngeal nerve (NRLN; Figure 6).
Anatomical Types of the Recurrent Larynx Nerve.
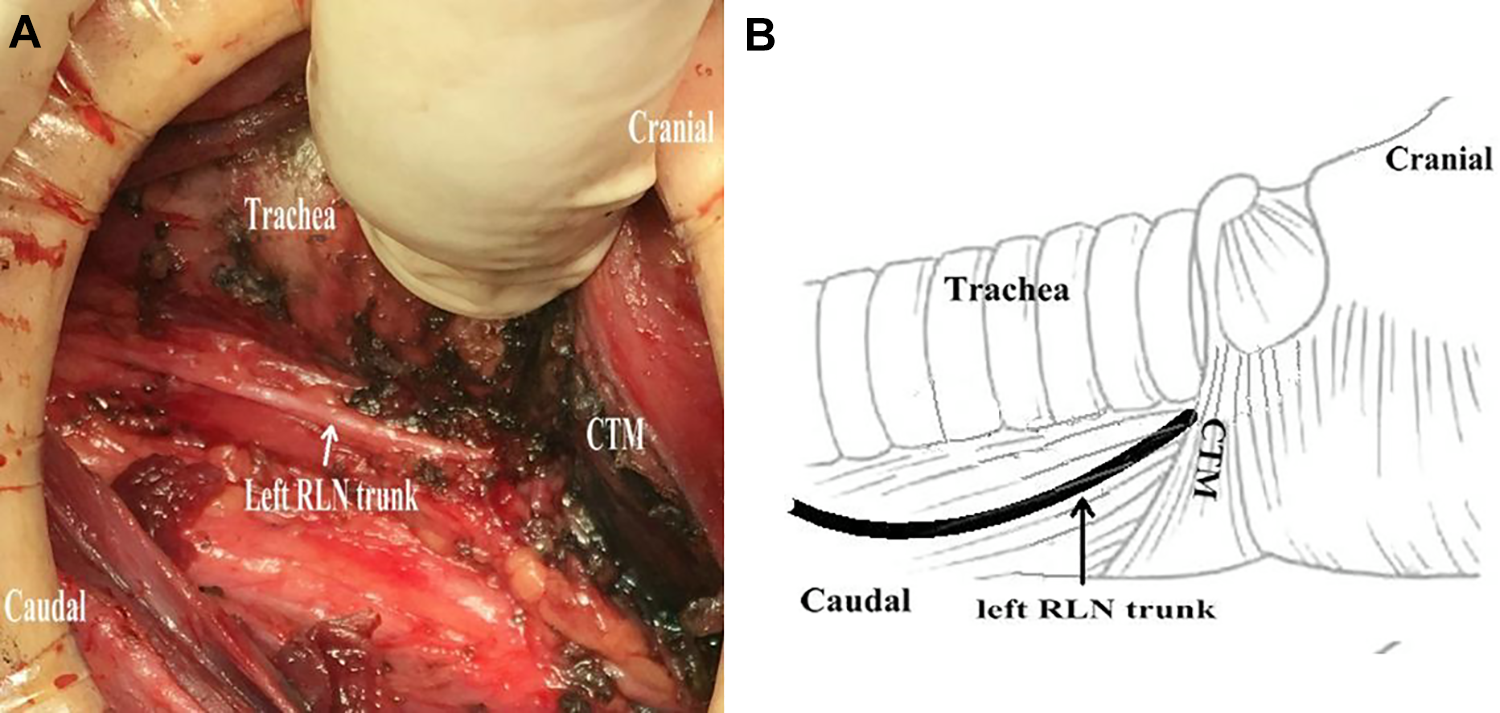
Type I RLN was characterized by a single upward nerve branch into the larynx, which is the most common variation in our cases. This type is easily found superiorly toward larynx entry. PT indicates parathyroid gland; RLN, recurrent laryngeal nerve.
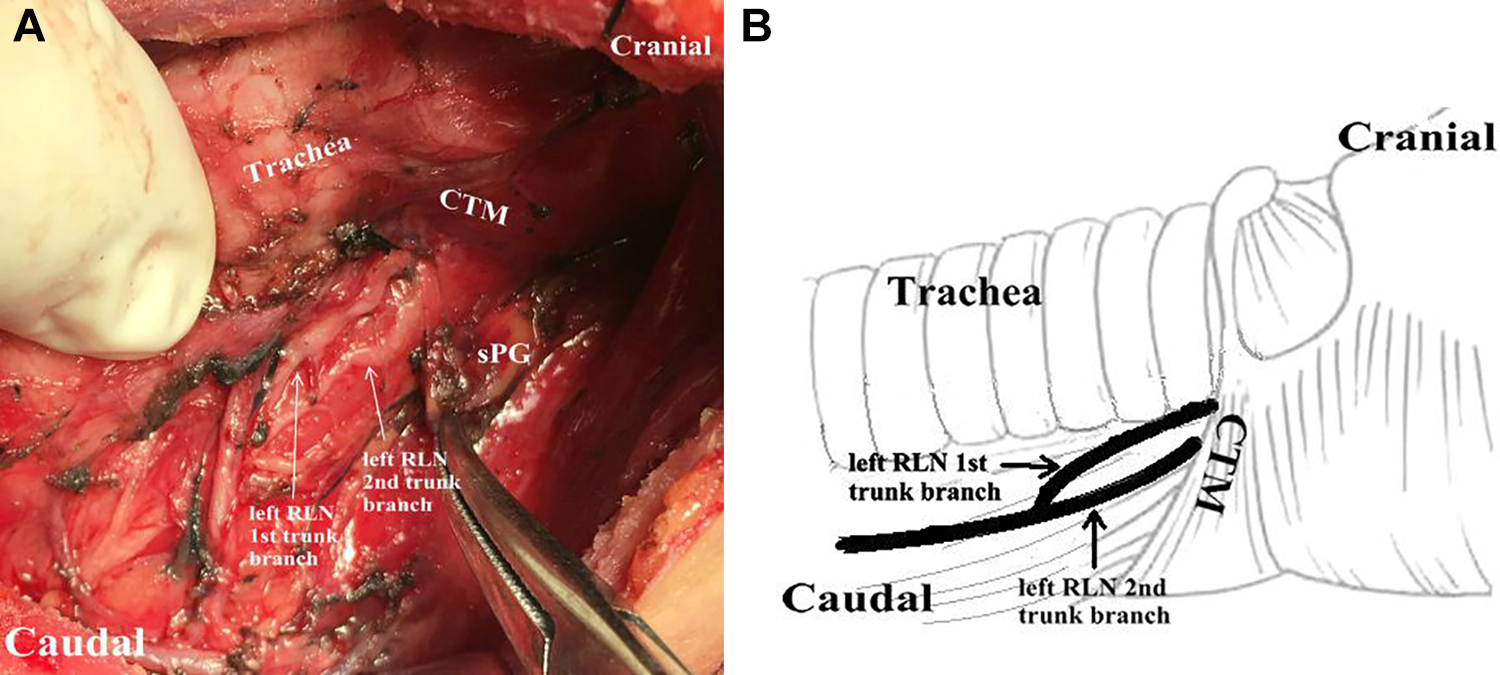
Type II RLN was characterized by 2 upward nerve branch into the larynx entry. The identification and exposure of Type II nerve usually begins at the lower pole of the gland by inferior approach. RLN indicates recurrent laryngeal nerve.
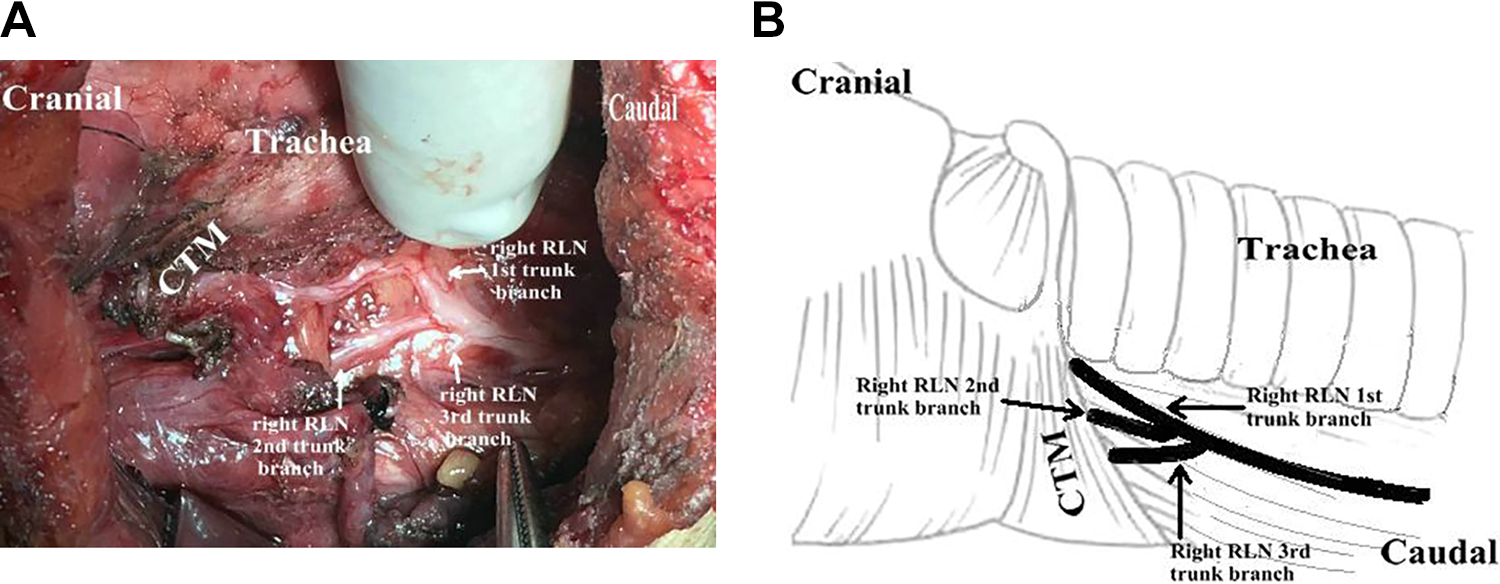
Type III RLN was characterized by 3 upward RLN branches into the larynx. The identification and exposure of Type III nerve usually begins at the lower pole of the gland by standard inferior approach. RLN indicates recurrent laryngeal nerve.
Type IV RLN was characterized by the entry of combining downward branch of vagus nerve and upward branch of recurrent laryngeal nerve into the larynx. Type II nerve usually was found by standard lateral approach. RLN indicates recurrent laryngeal nerve.
Type V RLN was characterized by bi-branches combining downward branch of vagus nerve and upward branch of recurrent laryngeal nerve into the larynx. Type V nerve usually was found by standard lateral approach. RLN indicates recurrent laryngeal nerve.
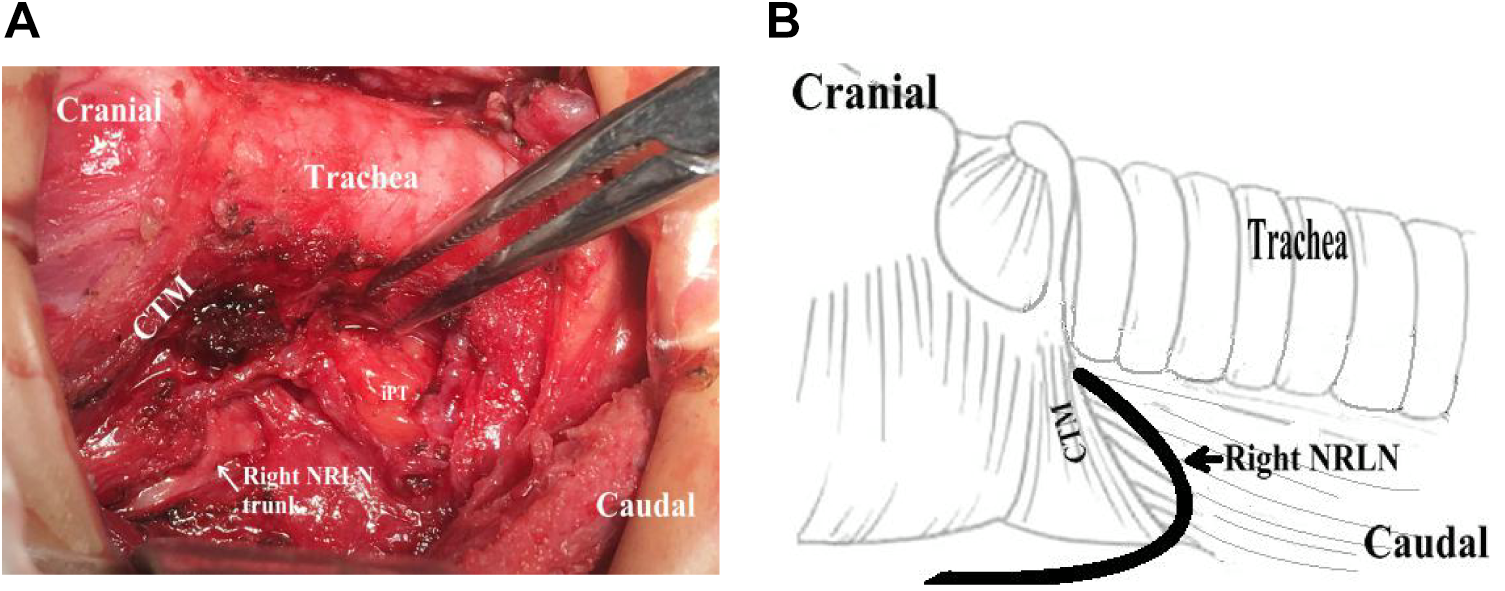
The feature of Type VI was that the nerve trunk passed from the vagus nerve behind the upper pole of gland into the larynx entry, also namely the nonrecurrent laryngeal nerve (NRLN).
Anatomical variations in left and right RLNs in patients were recorded. The incidence rates of bifurcation in the unilateral side or the bilateral side were determined. Bifurcation characteristics of nerves were compared between the right and left sides. The anatomical details of the patients were documented. Also every special variation was recorded photographically. Postoperative course and complications of each patient were also noted.
Statistical Analysis
Statistical analysis of clinic data was conducted on SPSS 23.0. All quantitative data were expressed as N (%), and the count data in anatomical variations of RLN on the right and left sides were compared via χ2 test. Significant difference for comparison was considered at P < .05.
Results
There were 294 patients included in this study (Table 1). The tested population in this prospective study consisted of 49 men and 245 women, with a median age of 49 years (range: 13-85 years). A total of 482 laryngeal nerve dissections, including 234 on the left side and 248 on the right side, were performed with unilateral exposure in 91 patients and bilateral exposure in 203 patients (Table 2). Six types of RLN variations were met in the patients and outlined in Table 2. Generally, 482 RLNs exhibited anatomical variation, with 234 (48.5%) dissections on the left side and 248 (51.5%) dissections on the right side, with no significant difference in laterality (P > .05). These variations were classified according to the original direction of RLNs and the bifurcation number of RLN into larynx entry. Type I was featured by a single superior RLN branch into larynx entry (Figure 1) and was observed on the left side (159 patients, 68.0%) and on the right side (170 patients, 68.6%). Type II was characterized by 2 diverging superior RLN branches into larynx entry (Figure 2), with 60 cases on the left side (25.4%) and 63 cases on the right side (25.6%). Type III was featured by the superior entry of 3 diverging branches of RLN into the larynx (Figure 3), with more observed on the left side than on the right side (6.4% vs 4.4%, P > .05). Type IV was defined as single entry of combining inferior branch of vagus nerve and superior branch of RLN into the larynx (Figure 4) and was found only on 1 right-side case. Type V was featured by 2 independent branches into the larynx entry after combining inferior branch of vagus nerve and superior branch of RLN (Figure 5) and was observed only on 1 right-side case. In Type VI, namely NRLN, the single nerve trunk passed from the vagus nerve and directly entered the larynx (Figure 6). The Types IV, V, and VI variations were just observed and identified on the right side. No patient experienced hoarseness or dyspnea after thyroid surgery.
Discussion
In this prospective study, the anatomical variations in RLNs on living patients who underwent thyroid surgery were evaluated. The traditional course of RLNs is as follows: the left RLN separates from the vagus nerve hooking around the aortic arch and returns into the larynx in the TEG. In comparison, the right RLN originating from the vagus nerve travels below the subclavian artery before entering the larynx within the TEG. However, not every RLN follows the same above course. Many publications have described various arrangements of RLNs and techniques for identifying and protecting RLN during thyroid surgery.6,7 In the current study, 6 types of anatomic RLN variants were identified. This is in contrast to prior studies where type 1, 2, and 3 nerve 8 branching patterns were recognized but where the number of RLN branches into the larynx was not considered as part of the classification scheme. Our experience suggests that the RLNs were divided in 30.9% of thyroid patients into 2 or 3 branches entering the larynx on both sides, which was a little higher than the percent reported by Makay et al. 9 The NRLN (Type VI) was found only in 0.4% cases. Despite the low incidence, NRLN has been studied extensively to decrease the risk of vocal cord paralysis for its injured in operation. 10 In addition to these variants (type I-III, type VI) that were identified in Western and Middle Eastern populations, 11 we identified 2 other anatomical variants (type IV, type V) of RLN in Chinese thyroid patients. Of them, the common feature is the inferior branch of the vagus nerve be combining with the superior branch 6 of RLN into the larynx, which is identified in Chinese patients for the first time in the present study and reported previously by our group. In this study, the anatomical variation rate of the right RLN was higher than that in the left side, but insignificantly (P > .05), which may be due to the lack of enough patients. Terminal RLN divisions prior to laryngeal entry have been the most commonly cited RLN anatomical variants encountered during surgery; however, the novel findings of Type 5 and 6 RLN branching patterns are important as surgical morbidity could increase dramatically with the coexistence of 2 (downward and upward) main RLN divisions. The RLN arborizes prior to the larynx entry at the cricothyroid joint, and injury to a small branch may result in a voice change. This is because the anterior branch of RLN mostly contains motor fibers, while the posterior branch mainly plays the sensory role. 12 Miyauchi et al described inverse innervation of cricopharyngeal muscles by extralaryngeal branches of the RLN that influences voice changes following thyroid surgery. 13 Recurrent laryngeal nerve should be identified during dissection in every thyroid operation, as recommended by American Thyroid Association Guidelines in 2015. 3 Moreover, the surgeon should be familiar with anatomical variations of the RLN in order to make effort to protect every variation type. Once the RLN is identified in operation, it should be dissected inferiorly and superiorly to confirm whether or not the adjacent structure is actually an anatomical branch of the RLN. Our operative philosophy is to identify and protect the main trunk and any adjacent structure of RLN. Before dissection of RLN, we must clearly identify the anatomic landmarks of RLN, such as TEG, inferior thyroid artery (ITA), Berry’s ligament, the Zuckerkandl tubercle, and the entrance of larynx. In the traditional anatomical course of the RLN, the TEG is the only landmark that must be traversed by the nerve, but NRLN and the type II of RLN in our cases do not rely on this path. According to the relationship between the ITA and the RLN, 4 widely accepted segments of the RLN were classified, including the prearterial, arterial, postarterial, and prelaryngeal segments. 9 But type IV/V and type VI of RLN were not included in this incomplete classification. The thyroid gland is affixed by the Berry’s ligament to the trachea and larynx. Berlin reported RLNs embedded in the Berry’s ligament, 14 while we found the same result as Sasou et al, who reported no RLNs penetrated this ligament. 15 Nevertheless, some RLNs embedded in the thyroid gland tumor had been located in our surgery. During our surgical dissection, the Zuckerkandl tubercle was a useful landmark for identification and preservation of RLN, which supported the important relationship of the Zuckerkandl tubercle with the RLN. 16 To the RLN, the entrance to the larynx is a relative fixation point for exposing it during surgery. But the terminal branches of RLN to the laryngeal entry point are quite different in quantity. According to anatomical knowledge of these topographic findings, the iatrogenic nerve injury rarely occurs from a dissection close to the gland in thyroid surgery. We did not always rely on 1 approach for dissection of RLN in all operations. The approach was chosen according to the concrete condition of RLN in the surgery. We used a combining method and can find and preserve the NRLN and the inferior part of type IV to V RLN trunk in situ by using the superior approach. The type I to III of RLN and the superior part of type IV to V RLN trunk can be identified and preserved from connective tissues along the TEG by using the inferior approach. The bonding point of type IV to V RLN can be found in the back area of the middle thyroid vein by adopting the lateral approach. The residual course of the nerve was completely traced to the larynx entry point under the cricothyroid muscle. We dissect each part (inferior branch of vagus nerve, superior branch of RLN, or/and the bonding point of them) of RLNs until the larynx entry point under the cricothyroid muscle though this combining approach (superior/inferior/lateral approach). The combining dissection approach was proved as successful and safe for protection of the RLN with no permanent paresis. There are 2 other RLN dissecting methods, including the medial approach 17 and the retrograde medial approach, 18 which both have limitations. With the first one which uses the surface of the third tracheal ring near the Berry’s ligament as a landmark, the surgeons employ a blunt dissection to expose the course of RLN, which may raise the risk of bleeding. With the second method focusing on finding the Zuckerkandl tubercle after releasing the superior pole, the surgeons search for the RLN in the cricothyroid region, which is similar to the superior approach without dissecting the upward part of type II RLN stunk. The combining dissection approaches decrease the risk of complications, including hemorrhage, vocal paralysis, and hypocalcemia. There are some limitations in the present study. First, the ratio of female to male patients undergoing thyroid surgery was 5:1, so we did not much consider the correlation of anatomical variations with male patients, which should be explored in future studies. Second, not enough patients for type IV to VI RLN variations were involved. Third, information regarding the relationship of RLNs with the anatomic landmarks (eg, TEG, Berry ligament, ITA, and Zuckerkandl tubercle) was not identified clearly. Finally, iatrogenic RLN injuries associated with these anatomical variations were not evaluated. Future multi-institutional studies are needed to clarify whether the more frequent anatomical variations in RLN relate to the increasing rates of iatrogenic nerve in the larger sample size. We believe that more than 6 types of RLN variation will be identified in future studies. Despite these limitations, our study has elucidated the safe way of preventing RLN damage is to identify and dissect it rather than to stay away from it.
Conclusion
The anatomical variations of RLN are frequently encountered in thyroid patients. Large anatomical variability of RLN may increase the risk of vocal cord paralysis caused by RLN injury. The anatomic variation types, which are classified based on the original direction of RLN and the terminal branch number into the larynx, may simplify identification and preservation of every variation in RLN. Therefore, the classification of RLN increasing the awareness of thyroid surgeons may be helpful for identification and dissection of RLN with terminal branches for a safe thyroidectomy.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The ethical commission approval number (TH2016-1-10). C.Y. is the first Author.
Acknowledgments
The author would like to thank Prof Bin Song for sharing knowledge on recurrent laryngeal nerve dissection, available in the dissection skills discussed, and promoting this classification of RLN for years now.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.