
Abstract
As a variant of recurrent inferior laryngeal nerve (RILN), the nonrecurrent inferior laryngeal nerve (NRILN) is closely related to the occurrence of abnormal subclavian artery (ASA). The nonrecurrent inferior laryngeal nerve has been found in patients without arterial abnormalities, which is seen in the coexistence of NRILN and RILN, but it is easily confused with sympathetic-inferior laryngeal anastomosis branch (SILAB). We encountered 2 right NRILN patients without ASA during thyroid surgery. This article summarizes the characteristics of these cases and proposes methods to distinguish the coexistence of NRILN and RILN from SILAB. So far, 11 articles have reported 16 cases of NRILN without arterial abnormalities. In patients without artery abnormality, the vagus nerve could send out a descending branch NRILN at the bifurcation of the carotid artery and enter the larynx after anastomosis with RILN. Adequate dissection of the carotid sheath may avoid confusion with SILAB, and neural monitoring is also expected to provide a reference for the identification.
Keywords
Introduction
As one of the anatomic abnormalities of the recurrent inferior laryngeal nerve (RILN), the nonrecurrent inferior laryngeal nerve (NRILN) is derived from the vagus nerve and is responsible for innervating the movement of laryngeal muscles and sensation of the laryngeal mucosa below the rima glottides. Once injured, NRILN can seriously affect the quality of life for patients. Due to the special anatomical position of NRILN, the injury rate of NRILN was found to be 8 times higher compared to that of RILN. 1 According to literature statistics, the total incidence of NRILN is .28%–.52%. 2 The incidence of right NRILN was .3%–1.6% and left was 15 cases (6 cases with arterial abnormalities,3-7 4 cases without arterial abnormalities,8-10 and the rest did not mention arterial condition11,12). The nonrecurrent inferior laryngeal nerve is usually accompanied by arterial abnormalities, and preoperative prediction can effectively avoid NRILN injuries. 13 But we encountered 2 cases of NRILN without arterial abnormalities during the operation. This type of NRILN is easy to be confused with sympathetic-inferior laryngeal anastomosis branch (SILAB), 14 which may cause accidental injuries if not identified in time. Cases without arterial abnormalities have not been systematically summarized and discussed, and it is necessary to conduct a comprehensive analysis of the articles providing intraoperative pictures and patterns. The experience summed up can further deepen surgeons' understanding of NRILN.
Case Report
Case 1
A 51-year-old Chinese woman had a mass neoplasm in her right neck for 4 months. There was no hoarseness and dysphagia. During the operation, a transverse neuro-like structure was seen below the isthmus of the right thyroid. The carotid sheath was thoroughly dissected for the purpose of ascertaining the neural origin. The result was that NRILN originated from the vagus nerve anastomosed with RILN and entered the throat behind the cricothyroid joint (Figures 1A–1C). Intraoperative freezing showed atypical hyperplasia of follicular epithelium. There was no hoarseness after surgery. Chest computed tomography (CT) considered it as the normal right subclavian artery (Figure 1D). (A–B) Surgical and imaging information of patient 1. Surgical picture of patient 1; CCA, common carotid artery; NRILN, nonrecurrent laryngeal nerve; CB, communicating branch; RILN, recurrent laryngeal nerve; Arrow: entrance of RILN to throat; and E, esophagus. (C) The pattern diagram of patient 1. (D) Postoperative chest CT of patient 1 showed normal right subclavian artery and brachiocephalic trunk. (E) Surgical picture of patient 2; CCA, common carotid artery; NRILN, nonrecurrent laryngeal nerve; ITA, and inferior thyroid artery. (F) Patient 2 showed normal right subclavian artery by cervical angiography and three-dimensional reconstruction after operation.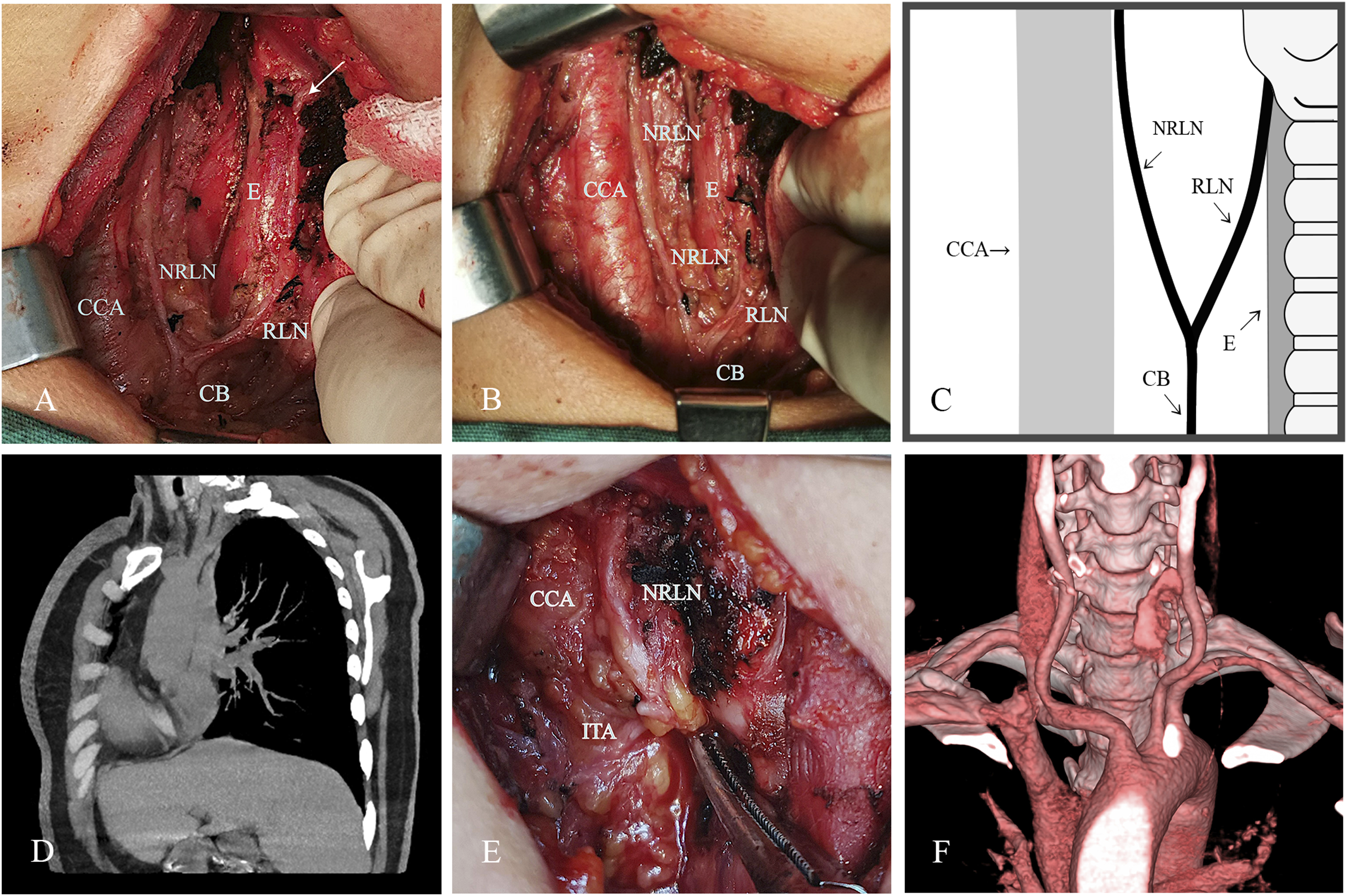
Case 2
A 50-year-old Chinese woman found a mass on her right neck during physical examination 5 weeks ago. Ultrasound-guided puncture was performed in another hospital, and the pathological diagnosis was papillary carcinoma. There was no hoarseness and dysphagia. The nonrecurrent inferior laryngeal nerve was detected at the superior level of the right thyroid (Figure 1E). There was no hoarseness after surgery. The normal right subclavian artery was shown by cervical angiography and three-dimensional reconstruction (Figure 1F).
Discussion
Right NRILN is frequently accompanied by abnormal subclavian artery (ASA), and preoperative examination of the abnormal artery may indicate NRILN. 15 The current prediction of NRILN mainly relies on image examinations, such as ultrasound and CT. It should be emphasized that ASA is a non-routine examination item, and 80% of radiologists will not specifically describe it in the reports even if it exists. 16 Moreover, NRILN without ASA also exists; thus, careful dissection and prudent operation in the course of surgery is the key point. The damage rate of NRILN has dropped significantly in recent years, but it is still far higher than that of RILN (NRILN = 14.3% vs. RILN = 1.75%). 1 For surgeons whose operation fields involve RILN, getting a good command of the anatomical characteristics of NRILN can effectively reduce injury. NRILN appears in surgeries of thyroid, parathyroid, esophagus, 4 cervical vertebra, 9 and carotid endarterectomy 10 ; it is suggested that the RILN should be systematically identified.
Here, we described 2 NRILN patients without arterial abnormalities. Literature review was also conducted by searching with terms nonrecurrent laryngeal nerve, non-recurrent laryngeal nerve, nonrecurrent inferior laryngeal nerve, non-recurrent inferior laryngeal nerve, anatomical variation, arteria lusoria, and sympathetic-inferior laryngeal anastomotic branch in MEDLINE, Web of Science, Cochrane, Google Scholar, Pubmed, and ScienceDirect without publication year limitation. The reference sections of the articles found were searched for additional reports. The references of all articles were searched to find articles missed in the database search. In case of multiple publications from the same authors or institutions, only the latest and largest series were considered, in order to avoid the duplication of cases. A total of 296 articles were included, of which 71 were excluded via titles and abstracts. Finally, 11 of 225 articles were included after reading the full text (Figure 2). Flowchart of study search and inclusion.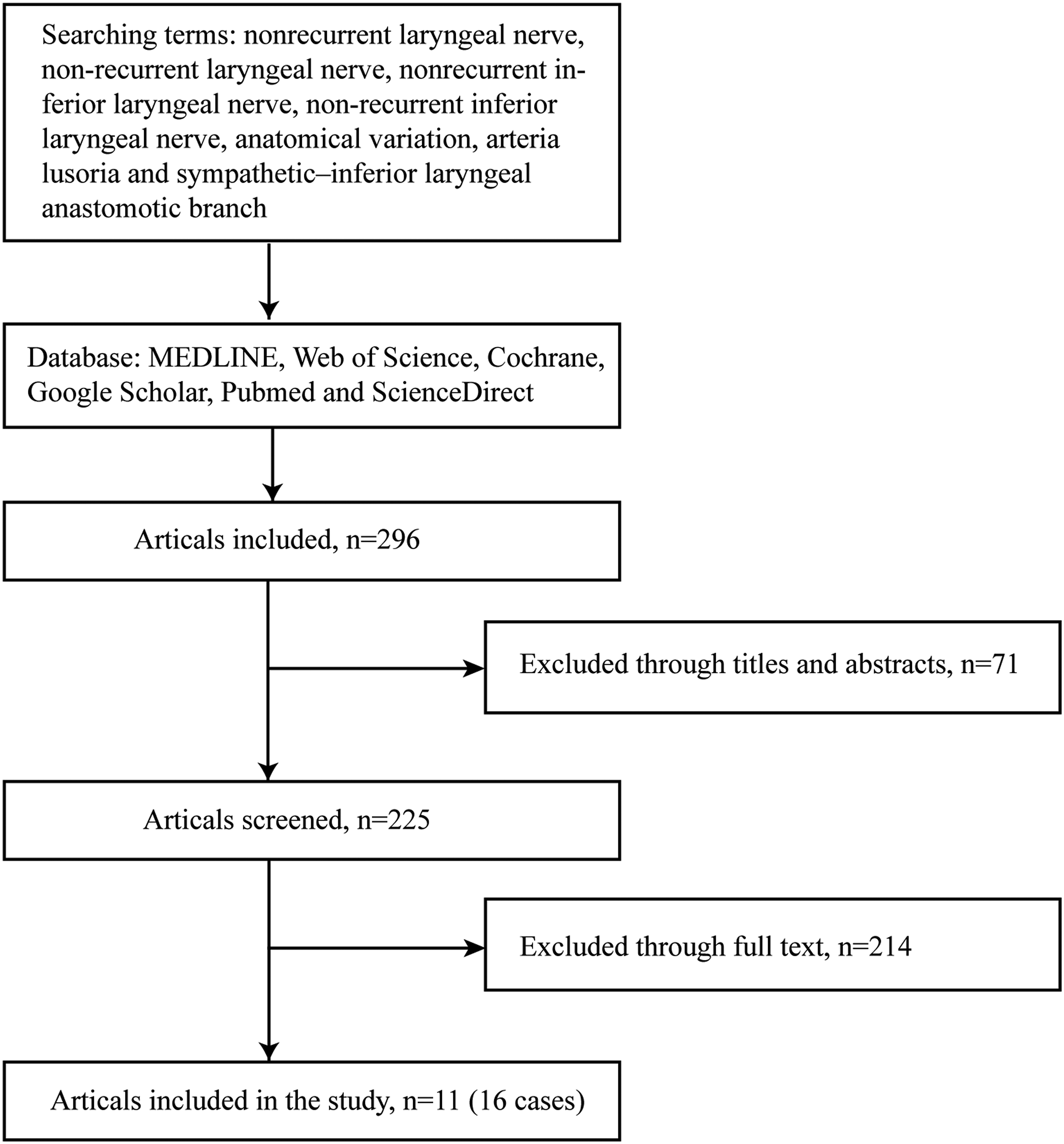
Cases of Nonrecurrent Inferior Laryngeal Nerve Without Arterial Abnormalities.
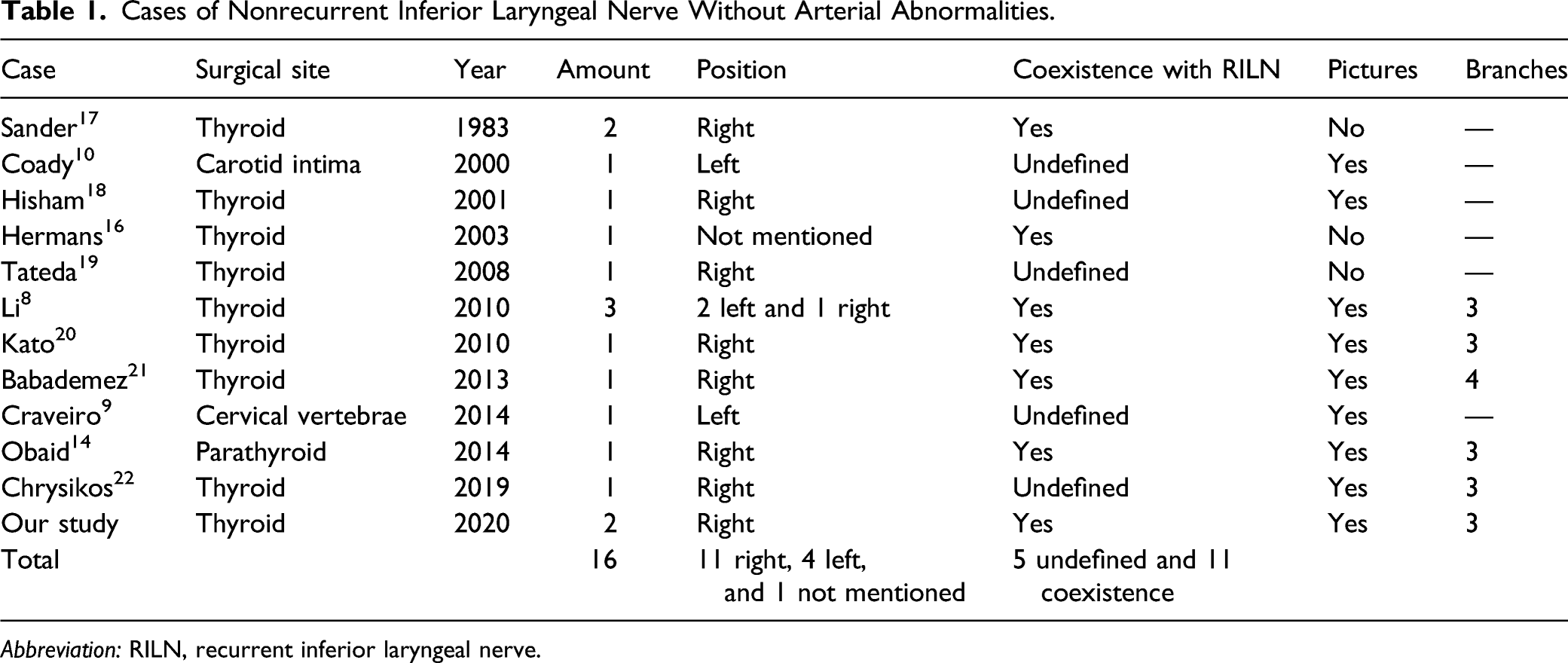
Abbreviation: RILN, recurrent inferior laryngeal nerve.
Embryology
The main cause of NRILN injury is the accompanying inferior thyroid artery (ITA), which will easily lead to mistaken ligation of NRILN. Thus, the anatomical relationship between NRILN and ITA became the basis of NRILN classification. The right NRILN typing proposed by Toniato has been widely used (Figure 3).
23
It should be noted that there is no clear boundary between type I and II a; the results of classification may be different due to intraoperative traction. Formation of NRILN is relevant to abnormal embryonic development. ASA (also known as the “lusoria” artery) evolves from the right fourth aortic arch and the cephalic dorsal aorta. When the above-mentioned arterial arch is abnormally developed, RILN lacking arterial restraint forms NRILN (Figure 3). Left NRILN occurs in ductus arteriosus deletion, right aortic arch, and visceral transposition, but these fatal variants render it a rare occurrence.
5
Up to now, there is no reasonable embryological explanation for NRILN without arterial abnormality. Classification of nonrecurrent inferior laryngeal nerve . Type I nonrecurrent inferior laryngeal nerve originated from the VN (vagus nerve) at the superior level of the thyroid and entered the larynx horizontally. Type II a nonrecurrent inferior laryngeal nerve entered the larynx above or parallel to the inferior thyroid artery. Type II b nonrecurrent inferior laryngeal nerve runs under the inferior thyroid artery or passes through between branches of the inferior thyroid artery.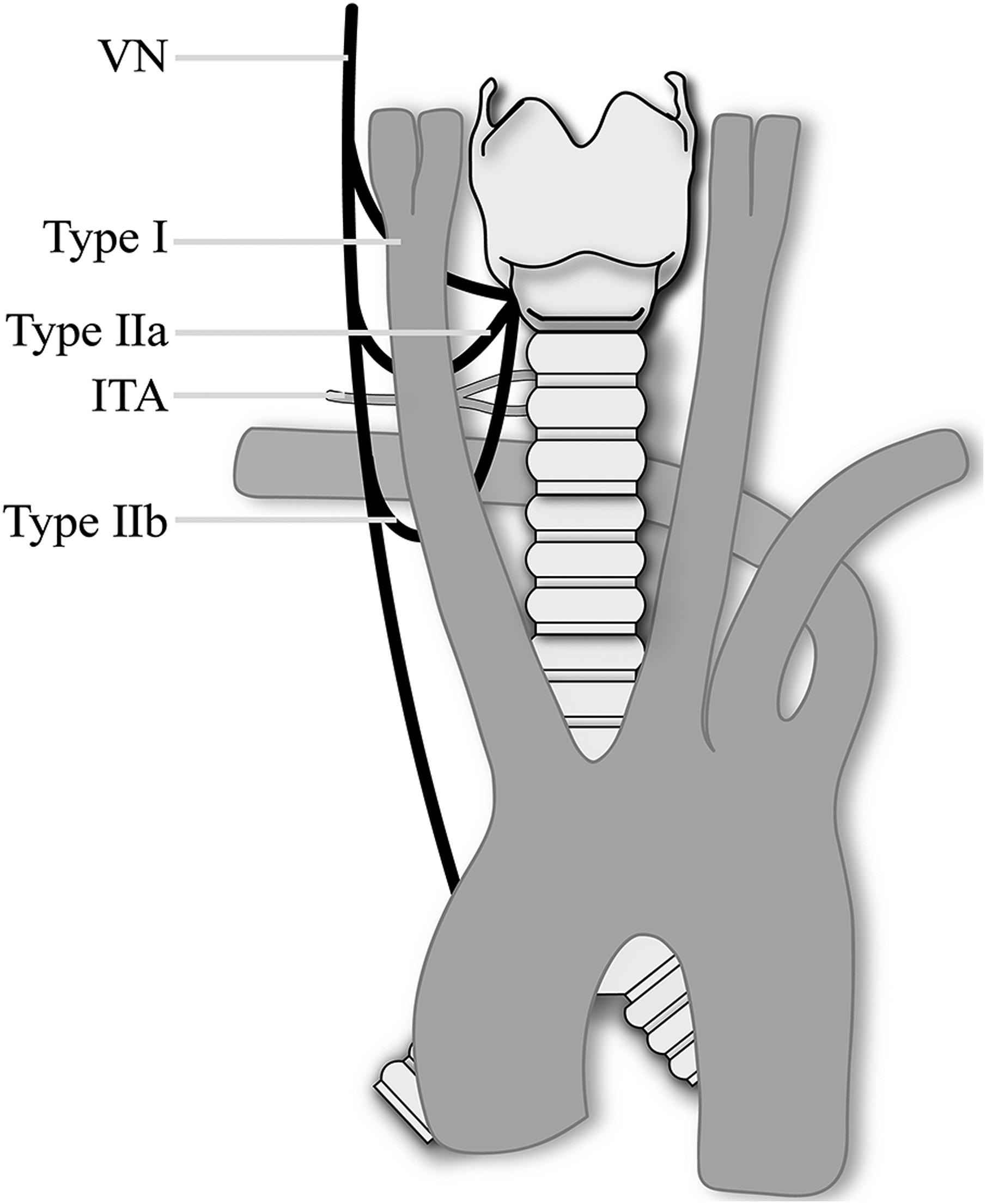
SILAB: An Explanation
Identification of Sympathetic-Inferior Laryngeal Anastomotic Branch and Nonrecurrent Inferior Laryngeal Nerve. 24
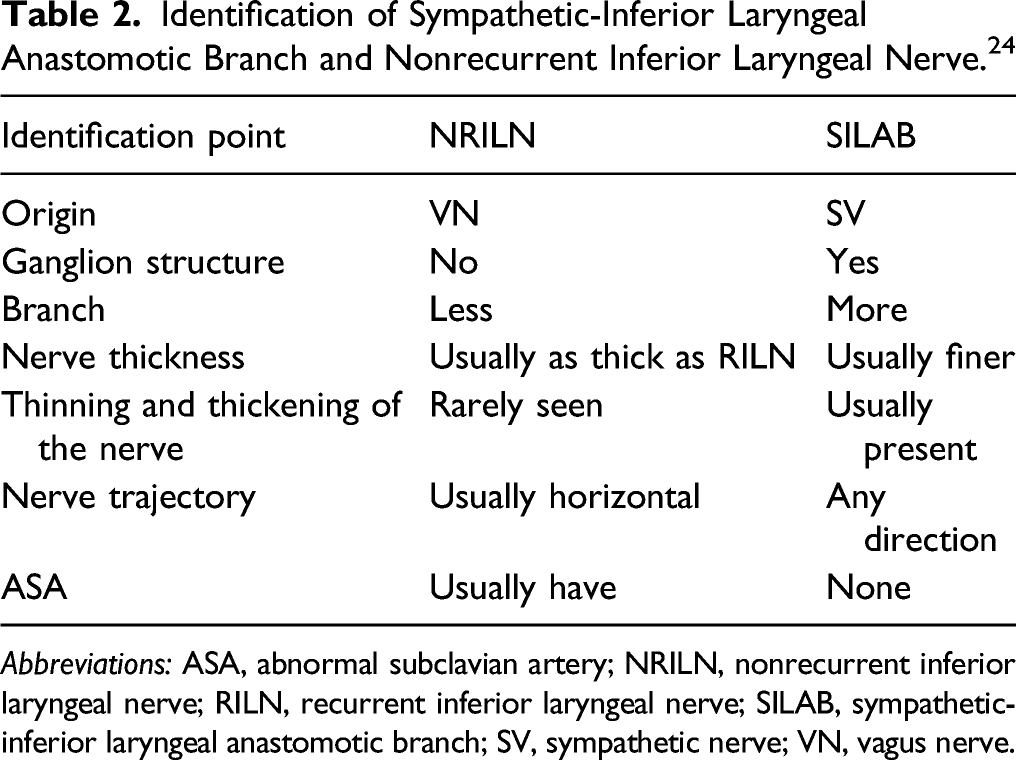
Abbreviations: ASA, abnormal subclavian artery; NRILN, nonrecurrent inferior laryngeal nerve; RILN, recurrent inferior laryngeal nerve; SILAB, sympathetic-inferior laryngeal anastomotic branch; SV, sympathetic nerve; VN, vagus nerve.
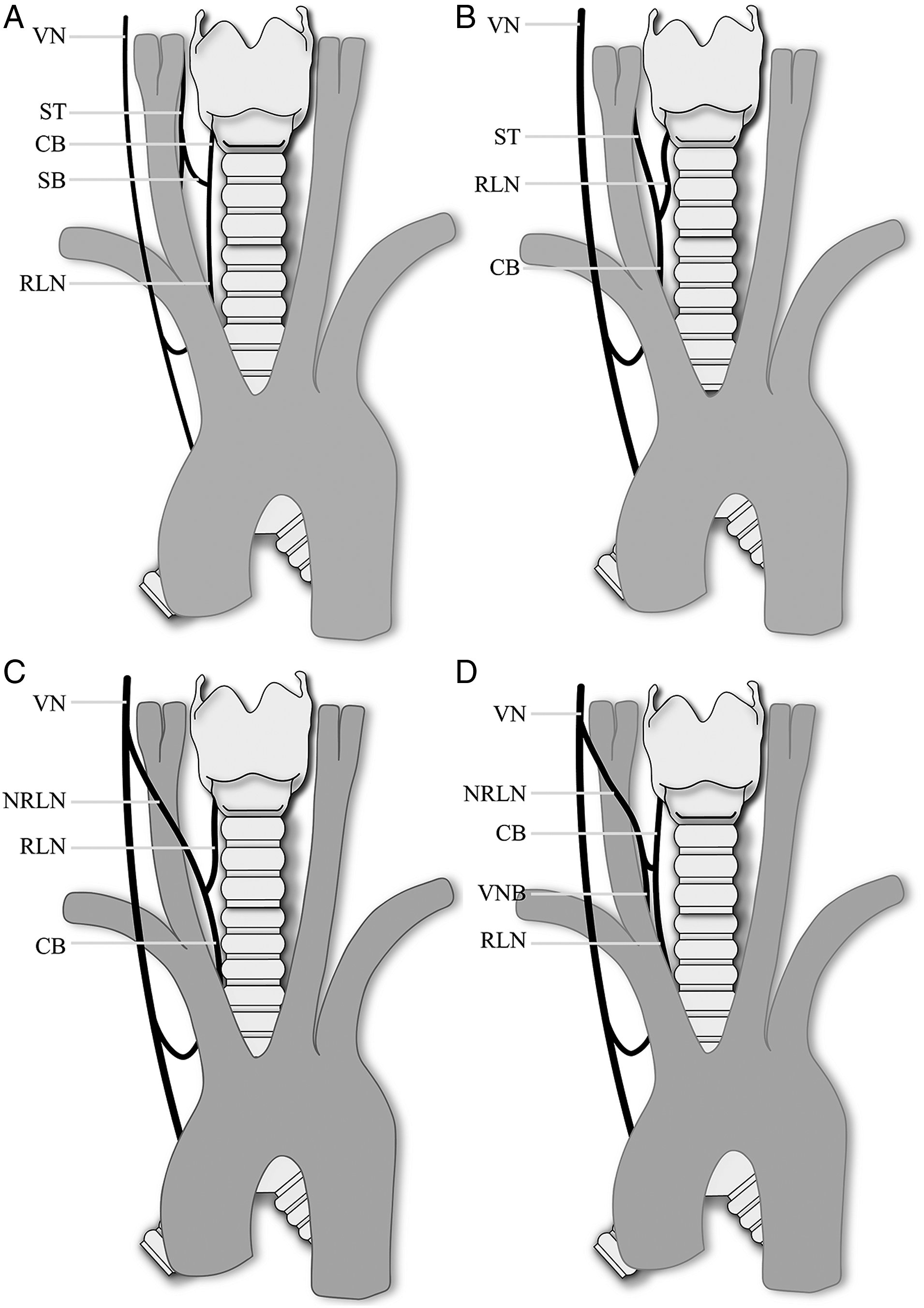
Explanations of nonrecurrent inferior laryngeal nerve without arterial abnormalities. (A) sympathetic-inferior laryngeal anastomosis branch, 4 nerves need to be defined; VN, vagus nerve; ST, sympathetic trunk; CB, communicating branch; and SB, sympathetic branch. (B) sympathetic-inferior laryngeal anastomosis branch, 3 nerves need to be defined. (C) Coexistence of nonrecurrent inferior laryngeal nerve and recurrent inferior laryngeal nerve, 3 nerves need to be defined. (D) Coexistence of nonrecurrent inferior laryngeal nerve and recurrent inferior laryngeal nerve, 4 nerves need to be defined; VNB, vagus nerve branch.
Coexistence of NRILN and RILN: Another Explanation
Notably, Iacobone presented a surgical image of SILAB which has no ganglion structure, no branches, is as thick as an RILN, and is of uniform thickness; this is more similar to the characteristics of NRILN (Figure 4B). Due to insufficient dissection, the coexistence of NRILN and RILN is also an explanation. Eleven cases of nerves without arterial abnormalities have been defined as the coexistence of NRILN and RILN (Table 1). Obaid described a case of the VN branch, which is located in the medial of the CCA, coexisting with RILN, 14 and there are 3 nerves that needed to be defined in the surgical field (Figure 4C). Babademez reported a case of anastomosis between NRILN and RILN which has 4 nerves that need to be defined in the surgical vision 21 (Figure 4D). To sum up, the coexistence of NRILN and RILN can be divided into 2 types, one is the coincidence of RILN with the vagus nerve trunk (Figure 4C), and the other is the vagus nerve branch (Figure 4D). More importantly, carotid endarterectomy and cervical vertebra surgery for patients without arterial abnormalities found that the vagus nerve could send out descending branches in the front of the carotid bifurcation,9,10 running inward and downward in the medial of the CCA. The medial vagus nerve prompt NRILN 27, this case provides a basis that the nerve originates from vagus, which is another strong evidence for the coexistence of NRILN and RILN. The carotid sheath of patient 1 was dissected until the top of the cricothyroid joint. The exposed nerves were thick, uniform in thickness, and had no branches and no ganglion (Figures 1A–1B). Therefore, the explanation of the coexistence of NRILN and RILN is reasonable, combining the evidence of carotid endarterectomy and cervical vertebra surgery.
Identification Methods
Anatomical studies propose that the nerve source should be adequately dissected if intraoperative identification of NRILN is difficult. 2 SILAB can be derived from sympathetic trunk (66.6%), middle cervical sympathetic ganglion (21%), superior cervical sympathetic ganglion (6.25%), and stellate ganglion (6.25%). 26 At least 12.5% of the SILAB require enlarging the surgical field to be clear if the sympathetic nerve is going to be thoroughly dissected, which may aggravate the collateral damage. According to our experience, dissection of the carotid sheath also contributes to the identification of NRILN and SILAB. It is recommended to fully expose the carotid sheath (especially the posterolateral and upper) to clarify the course of VN. Important as it is, rare cases have achieved that. VN is usually located on the medial side of the CCA in the presence of ASA and it could be located on the dorsal side of the CCA and internal jugular vein (IJV) (73%), only the dorsal side of the CCA (15%), only the dorsal side of the IJV (8%), or the ventral side of the CCA and IJV (4%) when the vessels are normal. 27 Surgeons should take those into account when dissecting the carotid sheath. Furthermore, VN stimulation may assist in identification of nerve. The latency threshold of NRILN during IONM is short, 5 but the research of IONM in the coexistence of NRILN and RILN has not been carried out yet. To sum up, surgeons should take advantage of all means to identify between NRILN and “false” NRILN, and try their best to avoid any damage to nerves.
Footnotes
Author Contributions
YL: manuscript drafting, picture editing, and manuscript submission. CHD: case surgeon and manuscript drafting. NL and PXW: data collection and manuscript revising. HZX: picture editing. SLF: manuscript revising. WZY: case surgeon and critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.