
Abstract
Abstract
Introduction:
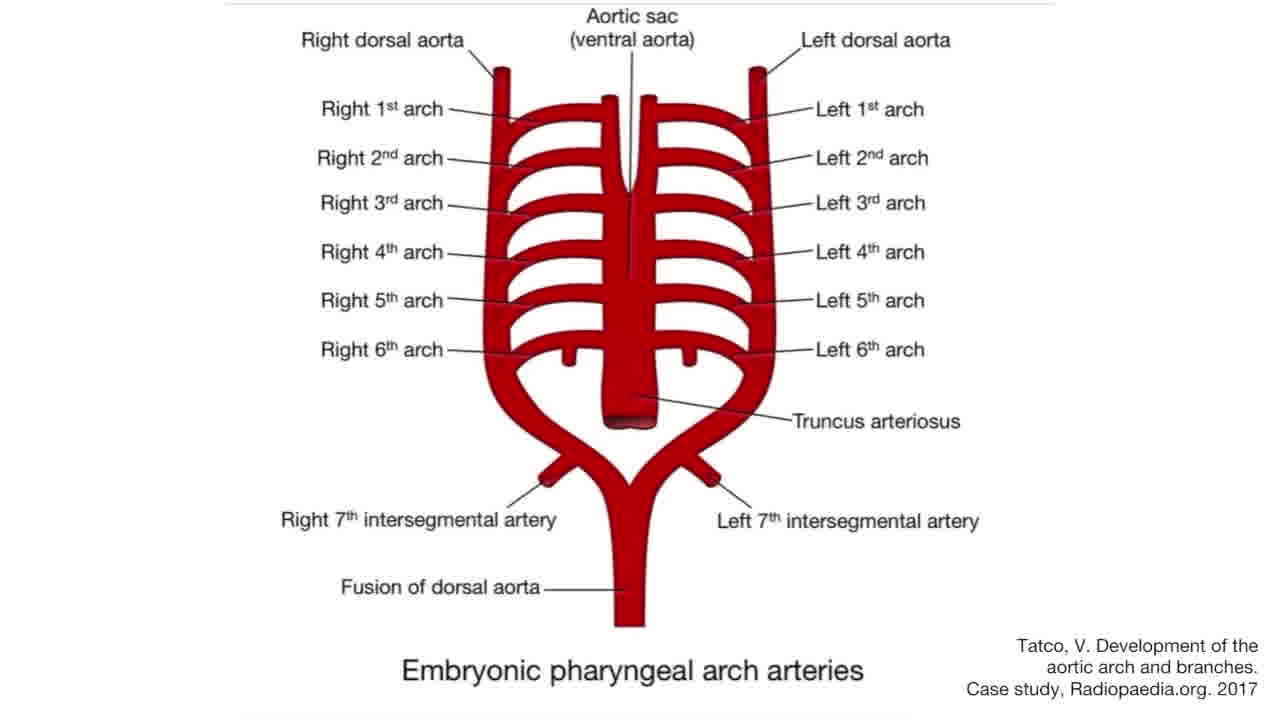
A nonrecurrent laryngeal nerve (NRLN) is a rare anatomical variant that arises because of the aberrant development of the fourth branchial arch vessels.1,3 The anomaly may be predicted based on preoperative cross-sectional imaging demonstrating aberrant positioning of the right subclavian artery posterior to the esophagus, termed an arteria lusoria. 4 We present two patients undergoing thyroidectomy, for whom preoperative imaging indicated an arteria lusoria and suggested the presence of an NRLN.
Materials and Methods:
Intraoperative videos were compiled from two procedures where NRLNs were identified, and videos were edited using Adobe Premiere Pro. Patient data were obtained from the electronic medical record. A literature review was conducted to facilitate preparation of introduction and conclusion.
Results:
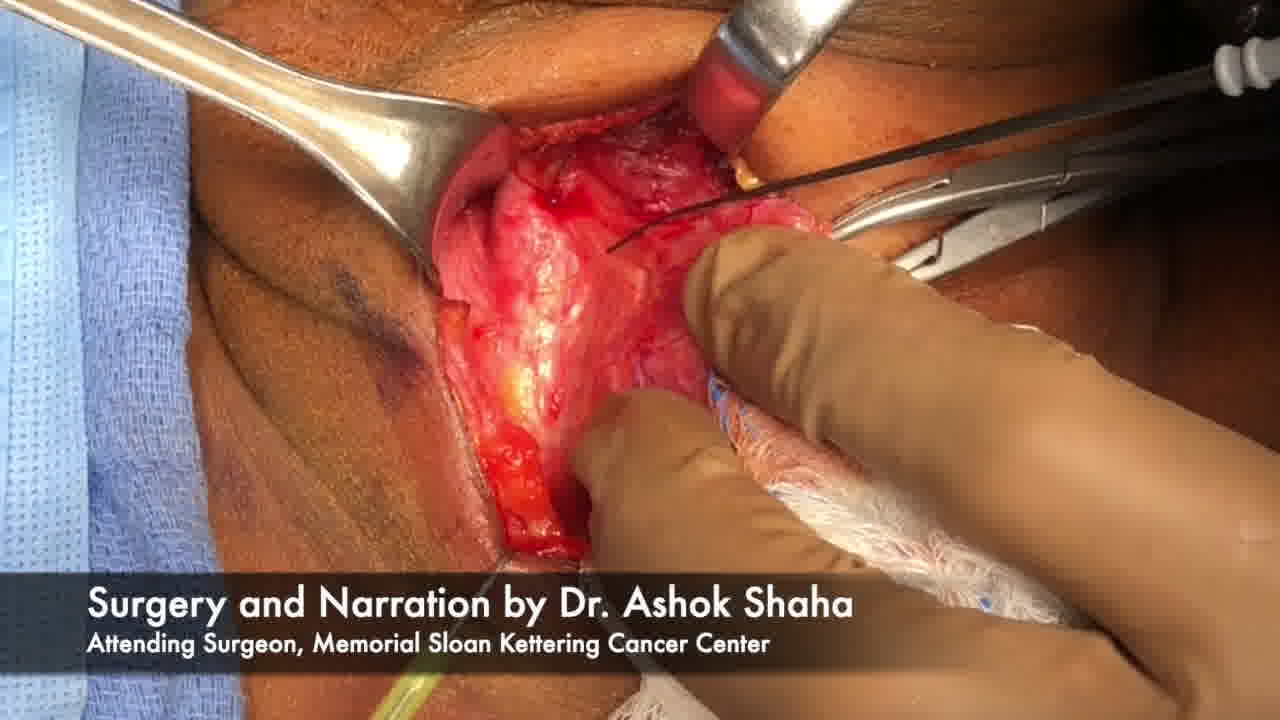
We first describe a 64-year-old woman who presented with a palpable thyroid nodule, noted on ultrasonography to represent a 2.2 cm nodule involving the right thyroid lobe and isthmus, and found to represent papillary thyroid carcinoma by fine-needle aspiration. A preoperative dedicated thyroid CT scan further demonstrated the papillary thyroid carcinoma, but also revealed an aberrant right subclavian artery with a slightly ectatic, or dilated, origin. This finding raised suspicion for an NRLN. The patient underwent total thyroidectomy, which was free of complications. Second, we report an 85-year-old woman with right-sided cervical nodularity, who was found to have a Bethesda IV right thyroid nodule with cervical metastasis to a right level V lymph node. As in the first case, preoperative CT imaging revealed an aberrant right subclavian artery. The patient safely underwent a total thyroidectomy and right neck dissection without any complications. In both cases, we highlight the relevant NRLN anatomy and demonstrate the process of intraoperative nerve monitoring and stimulation of the vagus nerve above and below the bifurcation of the NRLN.
Conclusion:
The NRLN is a rare anatomical variation that places patients at increased risk of recurrent laryngeal nerve injury. Although the use of intraoperative nerve monitoring has been debated in the past, we recommend this adjunct to meticulous surgical technique in the setting where a preoperative diagnosis of potential NRLN has been made. Understanding the cause of this anatomical variation and how to recognize it intraoperatively are essential for the safe practice of thyroid surgery.
Source of Work:
Memorial Sloan Kettering Cancer Center.
The authors declare no conflicts of interest
.
Runtime of video: 7 mins 37 secs
Keywords
Get full access to this article
View all access options for this article.