
Abstract
Myofibroblastic tumors are rare lesions which can affect any part of the body. Although benign, their mass effect causes symptoms that can become life-threatening. Supraglottic laryngeal involvement is extremely rare, with only 4 cases described in the English literature. Because the pathophysiology is unknown and the incidence is so low, there is no standardized therapeutic management, although for laryngeal tumors surgery has traditionally been the preferred initial option. Another less common option is intravenous and oral corticosteroid therapy, but this is usually reserved for myofibroblastic tumors in other head and neck sites that are more difficult to access surgically, or patients who cannot undergo surgery. These lesions have a very high tendency to recur, and morbidity rates are therefore also high. We present a case of supraglottic myofibroblastic tumor in which we elected high-dose corticosteroid therapy as the only form of treatment. With this new therapeutic approach, we avoided the undesirable effects of the usual type of surgery. At the 12-month follow-up, the patient is in complete remission.
Introduction
Inflammatory myofibroblastic tumors (IMTs), also known as inflammatory pseudotumours, plasma cell granulomas, plasma cell pseudotumors, and pseudosarcomatous tumors, are lesions characterized by a proliferation of fibroblasts and myofibroblasts with abundant inflammatory infiltrates. Although benign in nature, they can exhibit locally aggressive behavior. It is rare for these tumors to be found in the larynx; in all the English scientific literature, only 40 cases have been reported. They can present a challenge to pathologists, as they are difficult to diagnose and the etiology and pathophysiology remain unknown. Although there is still no definitive therapeutic management for IMT, surgery has been the therapeutic option of choice in laryngeal tumors, with corticosteroid therapy reserved for tumors affecting other areas. We present a case of a supraglottic tumor, which is extremely rare, with only 4 cases found in the literature. We used corticosteroids as our only therapeutic approach, with complete remission of the lesion at 12 months.
Case Report
Case 1
This was a 50-year-old healthy male who, one month earlier, had begun to experience dyspnea and the sensation of a foreign body in his pharynx. Endoscopy revealed a round, bilobed lesion in the midline at the base of the epiglottis. The mobility of the larynx was maintained. Computed tomography showed thickening of the base of the epiglottis with moderate enhancement occupying the pre-epiglottic fat, with the radiological appearance being nonspecific (Figure 1). A biopsy of the lesion was taken. Histopathology reported a proliferation of fusiform cells on a myxoid stroma with abundant mixed inflammatory cells composed mainly of lymphocytes and plasmids, accompanied by neutrophils and eosinophils. The fusiform cells had fairly regular elongated nuclei, no pleomorphism, with occasional figures of not-atypical mitosis and were distributed in a fascicular pattern. The immunohistochemical profile expressed was positive for vimentin and for smooth muscle actin, but negative for cytokeratin AE1/3, S100, desmin, myogenin, CD34, and anaplastic lymphoma kinase (ALK). Fewer than 20 immunoglobulin G4 (IgG4)-positive plasma cells were found per high-magnification field (×400), with an IgG4+/IgG+ ratio of approximately 10%. The covering was nonkeratinized squamous epithelium, with pseudoepitheliomatous hyperplasia. No dysplasia was identified. These findings led us to the diagnosis of IMT (Figure 2).
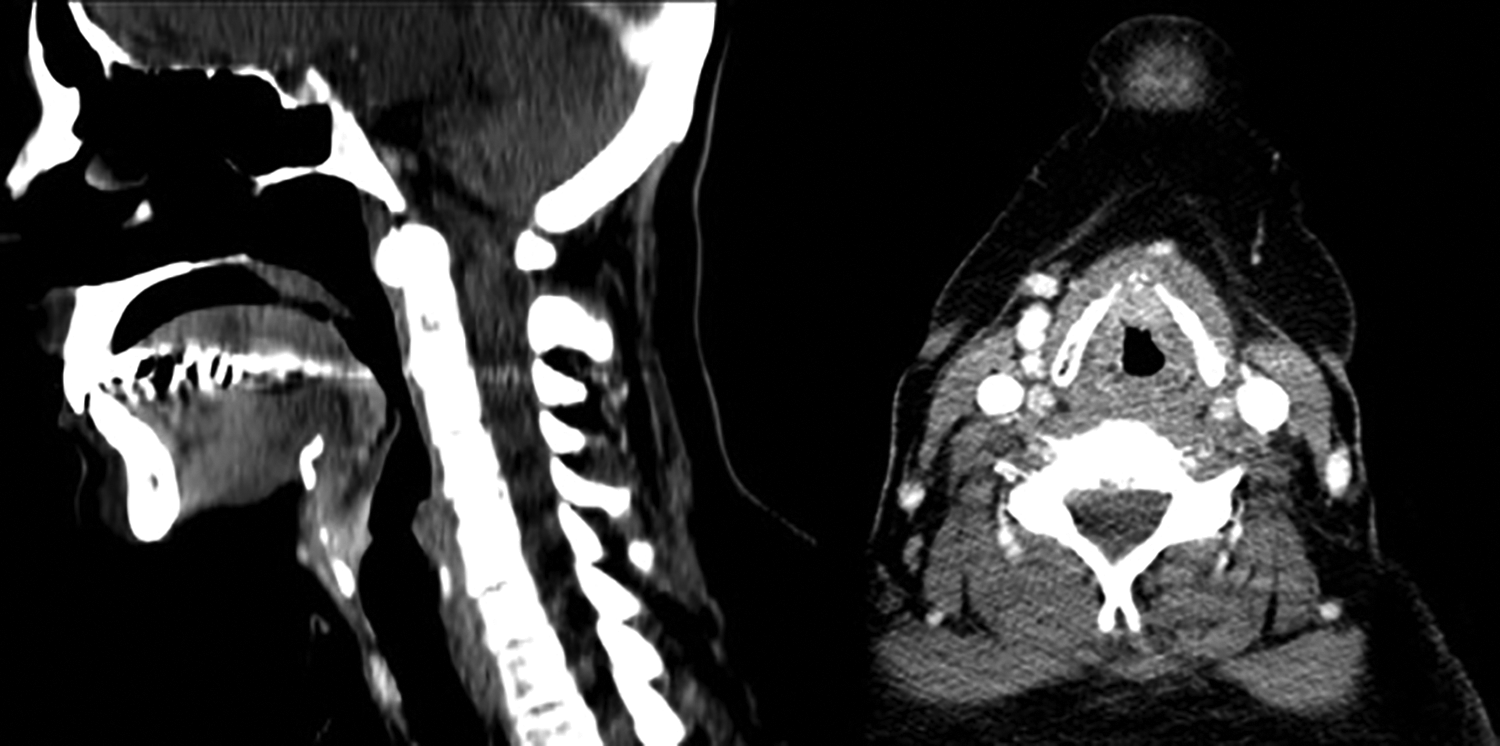
Two images are shown of the patient’s computed tomography (CT) before treatment. We see thickening of the base of the epiglottis with moderate enhancement, without defined masses, occupying the pre-epiglottic fat, all of which has a nonspecific radiological appearance.
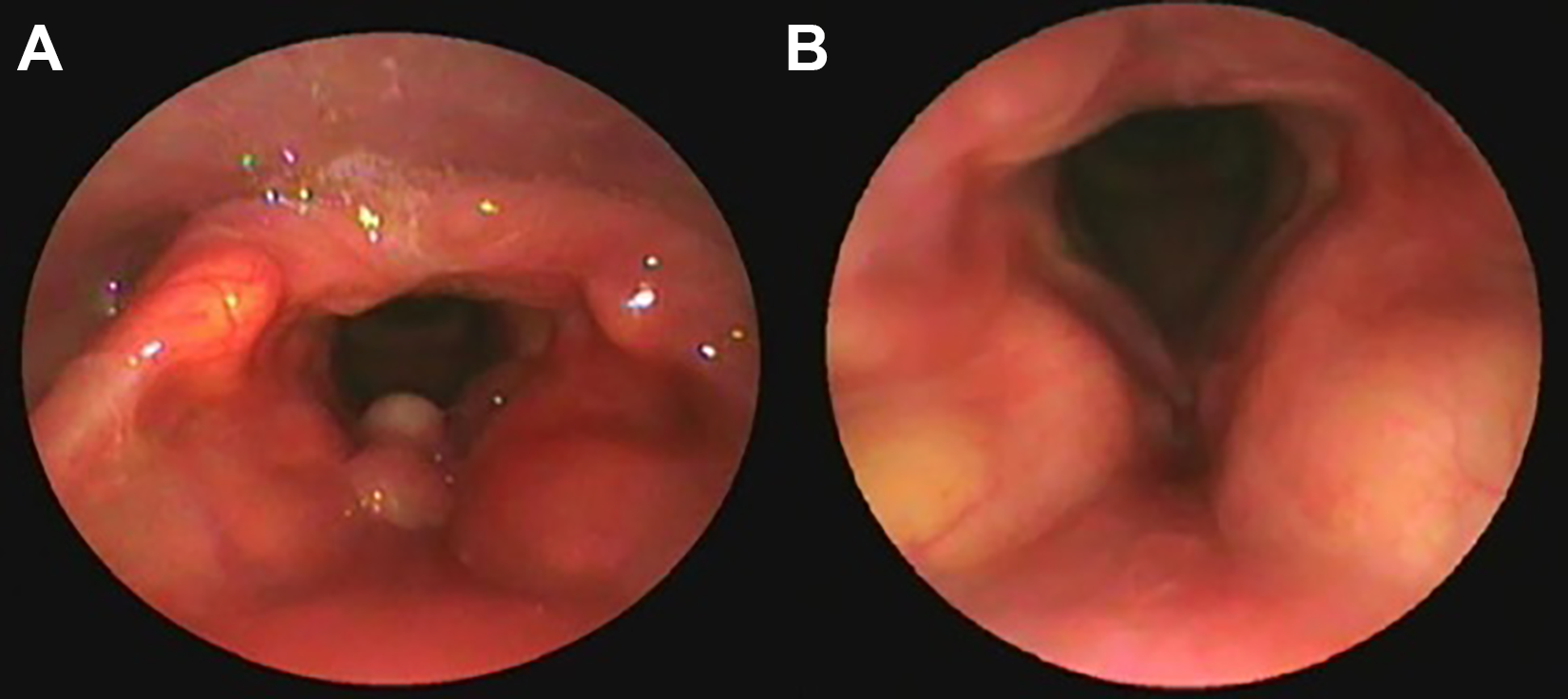
On the left is the endoscopic image of the patient’s larynx before starting treatment with corticosteroids. The bilobed lesion at the base of the epiglottis is evident. The image on the right shows the patient’s larynx 12 months after receiving the treatment.
The patient was treated with methylprednisolone at 1 mg/kg/d for 10 days, and great clinical improvement was found. Although the symptoms improved, the lesion had not completely disappeared and was therefore scheduled for laser excision. A second course of corticosteroid therapy was administered for another 10 days at 1 mg/kg/d before surgery. On the day of surgery, the lesion had completely resolved, so the procedure was canceled. At the 12-month follow-up, the lesion remains in complete remission (Figure 3).
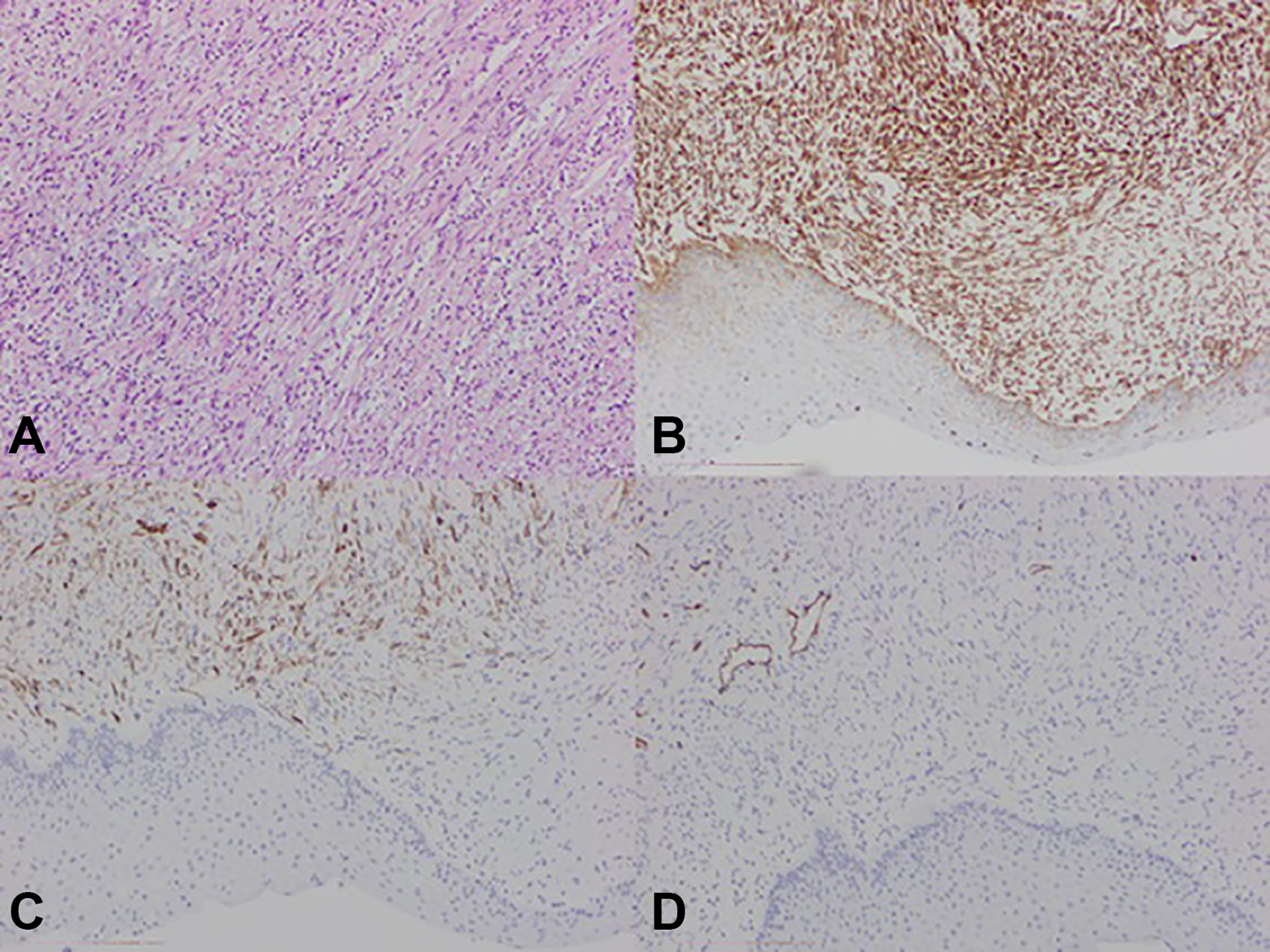
A) Fusiform cells and mixed inflammatory infiltrate with lymphocytes, plasma, eosinophils and neutrophils, in a loose stroma, with oedematous areas. B) Fusiform cells positive for vimentin. C) Positivity for smooth-muscle actin. D) Negative for CD34.
Discussion
Inflammatory myofibroblastic tumor is a rare tumor which can develop in any part in the body. The organs most commonly affected are the lungs and the gastrointestinal tract. Only 40 cases in total have been reported in the larynx. The most common laryngeal site is the glottis, and it is very rare to find IMT in the supraglottis, as in our case. 1,2
The symptoms of IMT depend on its location and are caused by its capacity for local invasion and mass effect. In the larynx, the main symptoms will be dysphonia, dysphagia, foreign body sensation, and dyspnea. 3,4 As our patient’s tumor was supraglottic, he had dysphagia and dyspnea, with dysphonia being less severe.
Inflammatory myofibroblastic tumor is a lesion mainly made up of myofibroblasts with a variable mix of chronic inflammatory cells and extracellular collagen. The terminology used for lesions with similar histopathological characteristics is confusing. 5 The term inflammatory pseudotumour has been used to cover a heterogeneous group of lesions that occurs in different organs, including the lung, liver, gastrointestinal tract, lymph node, or spleen, characterized histologically by a proliferation of fibroblasts and myofibroblasts with an inflammatory background. Other synonyms include postinflammatory tumor, plasma cell granuloma, and IMT. 2,6,7 The fundamental question about the pathogenesis of IMT is whether it is reactive or a true neoplasm. Because rearrangements and expression of the ALK gene have been found in 30% to 60% of IMT, it is now classified as a mesenchymal neoplasm rather than a reactive process. Inflammatory myofibroblastic tumor has intermediate biological potential, with a tendency to local recurrence but little risk of distant metastasis. 3,8 The tumor cells are very positive with vimentin, have a variable immunohistochemical reaction for myoid markers such as smooth muscle actin, muscle-specific actin, and desmin, and are positive for immunostaining with ALK in up to 60% of cases.
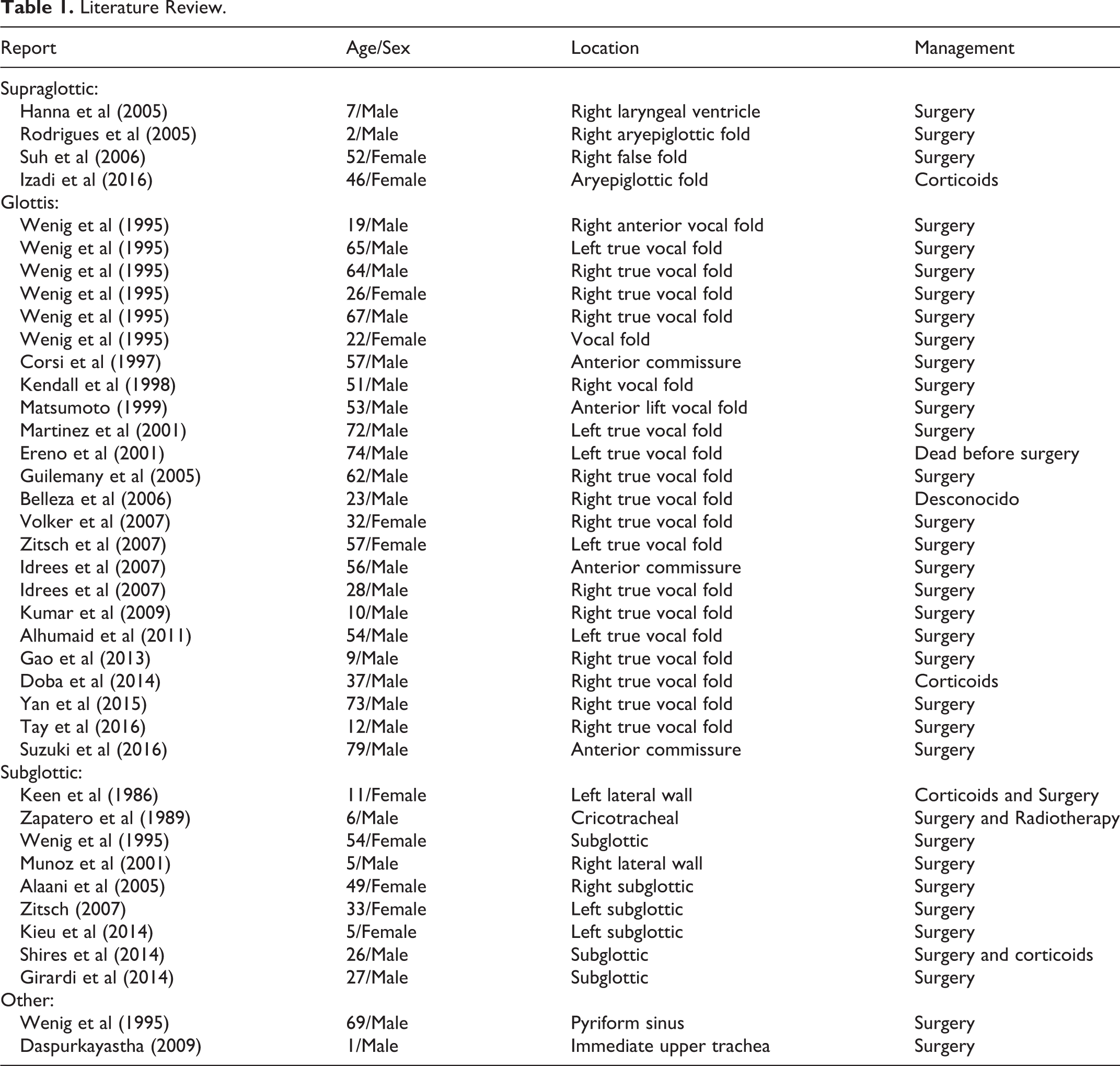
As shown in Table 1, the treatment of choice for this type of lesion is surgical excision. In the larynx, the most common type of surgery is laser cordectomy. The recurrence rate is quite high, with repeat surgery required in 50% to 60% of patients. In some cases, partial or even total laryngectomy is necessary. It is also common to have to perform a tracheotomy on these patients 1,8,9 (Table 1). In inflammatory pseudotumors in the larynx, corticosteroid therapy is generally reserved for difficult-to-access tumor sites, surgical recurrence, or patients with contraindications for surgery. However, corticosteroids have been used successfully for inflammatory pseudotumors in other head and neck regions such as the parapharyngeal space, orbit, face, and skull base. The success rate with corticosteroid treatment is around 80%, with a recurrence incidence of 40%. Due to the high recurrence and morbidity rates associated with surgery and the good response to corticosteroids, some authors prefer to use corticosteroids as initial therapy. 1,3,10 -14 In our case, we used methylprednisolone as first-line treatment instead of surgery. The lesion is in complete remission.
Literature Review.
The main limitation of our study was that we had a short follow-up time, since according to Humaid et al the recurrence period for these lesions is approximately 1 year. 1 In this regard, Kichenaradjou et al recommend longer follow-up periods due to the unpredictable behavior of these tumors. 12 However, the follow-up period we employed is in line with that published by the majority of the authors: Tay and Balakrishnan (12 months), 2 Yan and Hu (12 months), 6 Suzuki et al (14 months), 7 Do et al (6 months), 9 Kieu et al (12 months), 10 Girardi et al (14 months). 13
We have considerably reduced the comorbidity and suffering of these patients by applying these measures. We therefore believe that high-dose corticosteroid therapy should be considered as an initial treatment measure, reserving surgical management for cases in which steroids have failed, especially in such a delicate area as the larynx, where we are working with the patient’s airway and their ability to speak.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.