
Abstract
Inflammatory myofibroblastic tumor (IMT) of the larynx is a rare benign lesion that commonly occurs in the soft tissues. We present the first case with systemic manifestations of laryngeal IMT that was associated with hypochromic, microcytic-type anemia and thrombocytosis.
Introduction
Inflammatory myofibroblastic tumor (IMT) is a rare benign childhood tumor that more commonly occurs in the soft tissues and viscera. The lung is the most common site. 1,2 The etiology and pathogenesis of IMT is still unknown. Grossly the tumor is solid, well circumscribed, and noncapsulated. Weight loss, pain, malaise, nonspecific abdominal symptoms, fever, anemia, thrombocytosis, and elevated erythrocyte sedimentation rate (ESR) have been reported to be related to IMT. 2 The laryngeal presentation of IMT is very rare. 2,3 In the current literature, the reported systemic manifestations of laryngeal IMT were weight loss and elevated ESR in only one case. 4 We present the first case with laryngeal IMT that was associated with hypochromic, microcytic-type anemia and thrombocytosis. The anemia was cured 4 months after the excision of the lesion.
Case Presentation
We report the case of a 29-year-old woman, with microcytic-type anemia and thrombocytosis, who presented to our clinic with the complaint of hoarseness for a duration of 2 months after a sore throat. The risk factors for hoarseness such as vocal abuse, talking and singing loudly, and smoking were not present in her history. There was no dyspnea or dysphagia. There was not any family history of laryngeal diseases. Laryngeal endoscopy revealed a giant polypoid mass, originating from the left arytenoid cartilage that occupied most of the glottis (Figure 1). Her vocal cord movements were normal. On physical examination, her body temperature was 36.5°C and she was pale. Thoracic and abdominal examinations were normal.

Preoperative view shows the lesion in the supraglottic region.
Complete blood count revealed the following results: hemoglobin 10.5 g/dL, hematocrit 32.3%, red sphere count 4.56 × 106/mm3, mean corpuscular volume (MCV) 71 fL, mean cell hemoglobin (MCH) 23 pg, mean cell hemoglobin concentration (MCHC) 32.5 g/dL, platelet count was 464 × 103/m3. Peripheral smear examination under microscopy has shown significant hypochromia and microcytosis. Serum iron level was 21.2 μg/dL (60-180 μg/dL), serum iron-binding capacity was 458.6 μg/dL (155-355 μg/dL), and the ferritin was 3.66 ng/mL (13-150 ng/mL). Serologic and immunological tests were normal.
The patient was intubated with video laryngoscope. The lesion was removed totally with laryngeal microsurgery. The surgical removal was successful and the patient’s vocal symptoms recovered excellently (Figure 2). Pathology revealed an IMT; tumor was composed of elongated myofibroblasts in the collagenous background with lymphocytes and plasma cells, and immunohistochemical staining demonstrated the spindle cells positive for vimentin and smooth muscle actin; it was negative for pan-cytokeratin and the epithelial membrane antigen (Figure 3).

Postoperative view shows the completely removed pathology without recurrence.
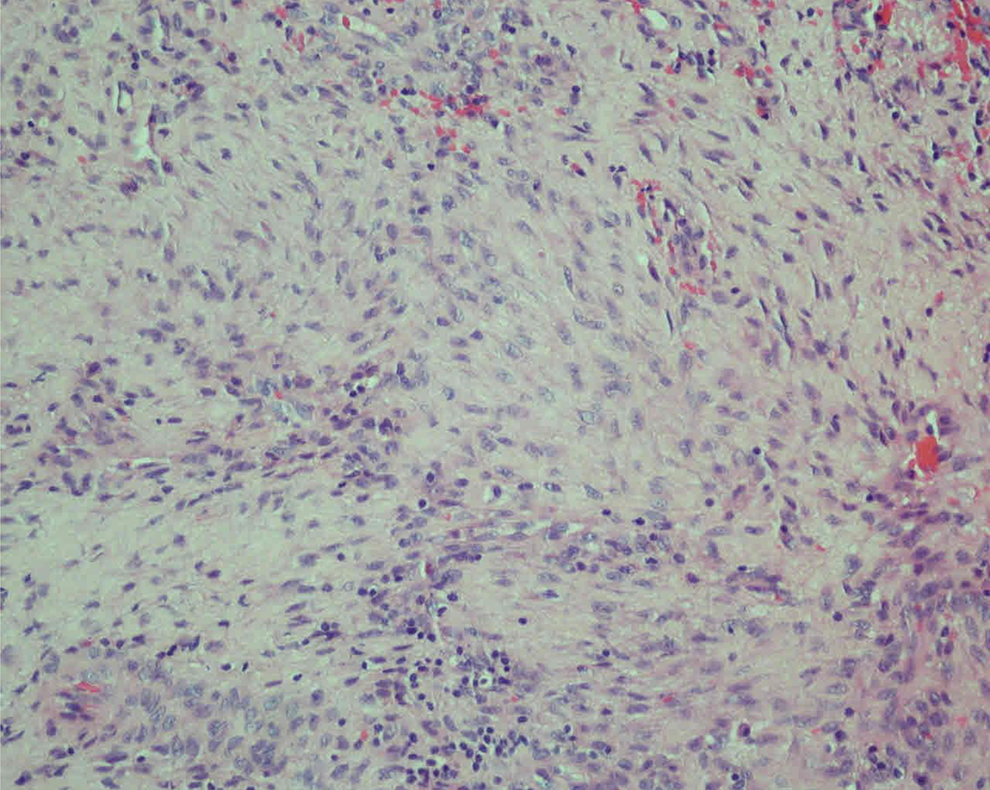
Positivity for smooth muscle vimentin and actin, cytoplasmic staining (smooth muscle actin, ×400).
Discussion
Inflammatory myofibroblastic tumors are rare benign tumors and histologically featured by myofibroblastic and fibroblastic spindle cells accompanied by an inflammatory infiltrate including plasma cells and lymphocytes. They are also known as histiocytoma, plasma cell granuloma, plasma cell histiocytoma complex, inflammatory fibrosarcoma, and benign myofibroblastoma. Since 1994, the definition “inflammatory myofibroblastic tumor (IMT)” has been used to describe this lesions. 5 Although benign in nature, they tend to be locally aggressive for local invasion and recurrences. 6 The local recurrences are notified in roundly 25% of cases. 2 These lesions are frequently found in the lungs, but similar lesions have been reported in virtually any tissue or organ of the body such as the genitourinary tract, gastrointestinal tract, the breast, salivary glands, sinonasal tract, orbit, and the central nervous system. 2,6,7 Systemic manifestations, for example, fever, anemia, polyclonal hyperglobulinemia, thrombocytosis, or elevated ESR have been reported in relation with IMTs. 2 Coffin et al 2 reported 84 extrapulmonary cases of IMT and 31 cases had anemia and 5 had thrombocytosis. These signs and symptoms, which usually disappear after surgery of the mass and return with recurrent disease, suggest a link to the development of IMT with an altered immune response. 2,3
The laryngeal IMT was first described in 1992. 8 To date, only 50 to 60 cases of IMT have been reported in the larynx. Guilemany et al described the first and only case in the larynx with systemic manifestations with a 6-month history of weight loss (20 kg), no constant fever, and an increased ESR of 46 mm/h. They reported that he recovered his normal body weight and ESR after surgery. 4 We also reported the first case with hypochromia, microcytic-type anemia (hemoglobin 10.5 g/dL) and thrombocytosis (platelet count 464 × 103/mm3) at laryngeal IMT. Our patient recovered her normal complete blood count 4 months after surgery.
The etiology and pathogenesis of laryngeal IMT is still unknown. Many theories have been proposed, and these include trauma, infections, immunological host response, smoking, neoplasm, and immunological factors. Three cases with direct laryngeal trauma have been reported in the literature. Traumatic intubation in 2 patients and external neck trauma during traffic accident with airbag inflation in the other patient. 8,9 However, trauma is difficult to prove as an etiology because there are only a few cases. Voice abuse, excessive coughing, smoking, and acid reflux are also subclinical traumatic stimuli.
These factors are usually associated with wound healing which includes the presence of myofibroblasts. 5,10 The neoplastic theory has been suggested because of recurrence, regional metastases, extensive local invasion, and malignant transformation (anaplastic lymphoma kinase 1 [ALK 1] receptor locus on chromosome 2p23, reported in up to 50% of IMTs). 11,12 In the case of laryngeal IMT, the fusion partner gene of ALK was first reported by Yorita et al. 13
The most common sites involved in the larynx are the true vocal cords followed by subglottis and rarely supraglottis. 14,15 In our case, IMT was detected in the supraglottic region (left arytenoid). The complaints usually depend on the site involved. In our case and other case series, voice change is the most common presentation, followed by stridor, dyspnea, shortness of breath, and globus sensation. 14,15
The treatment of this disease is best achieved by microlaryngoscopy (with or without laser) and complete excision with safe margins (with or without steroid therapy). 14 -16 Immunohistochemical staining is necessary for the diagnosis of these tumors. The typical immunostaining pattern is reactivity for vimentin with muscle-specific actin and smooth muscle actin.
Conclusions
While IMTs of the other organs and tissues have been associated with many systemic findings, the laryngeal IMTs have been reported to be associated only with weight loss and elevated ESR. This case is the first case that is associated with anemia and thrombocytosis. Anemia and thrombocytosis recovered after the excision of the tumor without any specific treatment for the anemia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.