
Abstract
A 51-year-old woman with headache was referred to our hospital. She had a history of endonasal pituitary surgery 22 years prior and hypertension 10 years prior. The endonasal transsphenoidal pituitary approach was performed via microscopic transseptal approach. Nasal endoscopy revealed whitish cystic wall protruded from the right sphenoid sinus. Functional endoscopic sinus surgery was performed under general anesthesia. After incision of the right sphenoid ostium, yellowish mucoid discharge in the right sphenoid sinus was pushed out from the sphenoid sinus. Histopathology confirmed fungal ball in the sphenoid sinus, which is consistent with aspergillosis sinus. The presence of fungal ball and mucocele are rarely reported, but mucocele and fungal ball found after pituitary surgery are the first and therefore unique in this case.
A 51-year-old woman with headache was referred to our hospital. She had a history of endonasal pituitary surgery 22 years earlier and hypertension 10 years earlier. An endonasal transsphenoidal pituitary approach was performed via a microscopic transseptal approach. Nasal endoscopy revealed a whitish cystic wall protruding from the right sphenoid sinus (Figure 1A). Coronal computed tomography (CT) demonstrated total opacification of soft tissue in the right sphenoid sinus (Figure 1B). Magnetic resonance imaging (MRI) showed that a marked hypodense signal on T1- and T2-weighted images was surrounded by a high signal on those images (Figure 1C and D). We initially diagnosed a mucocele in the right sphenoid sinus.
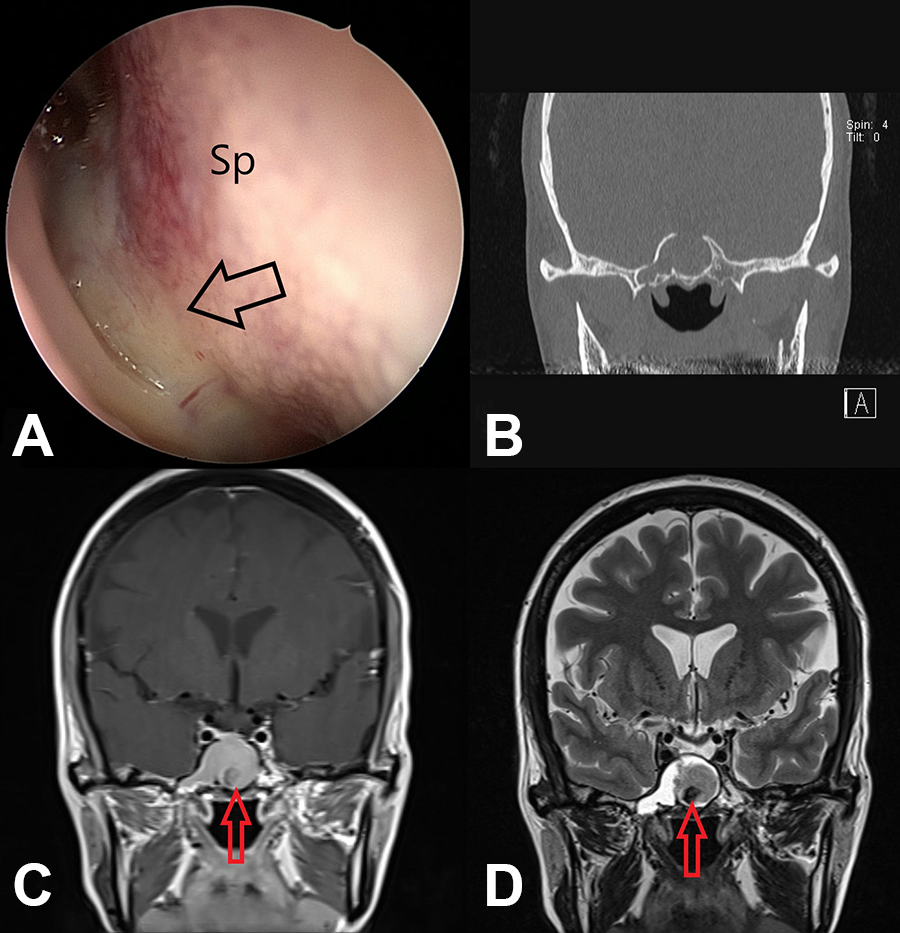
(A) Nasal endoscopy revealed a whitish cystic wall protruding from the right sphenoid sinus (black open arrow). (B) Coronal computed tomography (CT) demonstrated total opacification of soft tissue in the right sphenoid sinus. (C, D) Magnetic resonance imaging (MRI) showed that a marked hypodense signal (red open arrows) on T1- and T2-weighted images (WI) is surrounded by a high signal on those images.
Functional endoscopic sinus surgery was performed under general anesthesia. After incision of the right sphenoid ostium, a yellowish mucoid discharge exuded from the right sphenoid sinus (Figure 2A). After suction of the mucoid content, clay-like material was detected in the sphenoid sinus and was removed with saline irrigation (Figure 2B). Histopathology confirmed a fungal ball in the sphenoid sinus, which is consistent with aspergillosis.
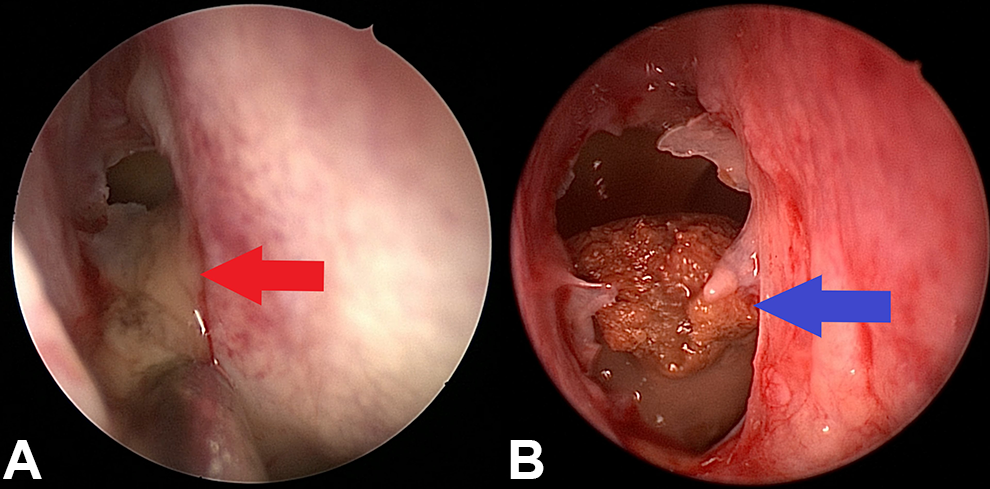
(A) Yellowish mucoid discharge exuded from the right sphenoid sinus. (B) After suction of the mucoid content, clay-like material was detected in the sphenoid sinus and was removed with saline irrigation.
The pathophysiology of fungus ball has not been precisely clarified at the present time, but one of the most likely causes is damage to sinus ventilation. 1 A mucocele is also known to be caused by an obstructed ostium. Diagnosis of a mucocele on preoperative CT and MRI is quite straightforward. Protein concentration in the mucocele can affect the signal intensity on T1- and T2-weighted images. A high protein content may increase the signal intensity on T1-weighted images and decrease the signal intensity on T2-weighted images. 2 In this case, we detected a mucocele with a superimposed fungal infection in the sphenoid sinus. The presence of a fungal ball and mucocele together is rarely reported; this is the first reported occurrence of a mucocele and fungal ball found after pituitary surgery. 2,3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by the Fund of Biomedical Research Institute, Chonbuk National University Hospital.