
Abstract
Background:
Paranasal sinus mucoceles, by virtue of extension into the orbit or cranial vault, can lead to significant ocular, nasal, or neural complications. There is limited comprehensive data on the presentation, management, and outcomes of cases with intraorbital or intracranial extension. A thorough analysis is essential to enhance clinical practices and improve patient outcomes.
Objective:
This retrospective case series investigates the clinical presentations, radiological features, and surgical outcomes of 10 patients with paranasal sinus mucoceles exhibiting intraorbital or intracranial extensions.
Methods:
Ten diagnosed cases of paranasal sinus mucoceles with intraorbital or intracranial extensions, as identified on CT or MRI imaging, were selected and retrieved from the electronic database of an academic-affiliated hospital from July 2013 to December 2023. Data were analyzed using descriptive statistics with IBM SPSS version 23.0 software.
Results:
The study revealed a mean patient age of 65 years, with females (60%) affected more than males (40%). The ethmoidal and frontal sinuses were predominantly involved, with varied clinical symptoms ranging from periorbital pain to visual disturbances. Radiologically, CT and MRI scans depicted extensive sinus involvement, often with intraorbital (50%), intracranial (20%), or combined (30%) extensions. Surgical interventions, primarily endoscopic sinus surgery, resulted in favorable outcomes, including symptom resolution, minimal complications, and no recurrence.
Conclusion:
This case series emphasizes the importance of thorough preoperative evaluation, individualized surgical approaches, and vigilant postoperative care in managing mucoceles with orbital and cranial involvement. Further research with larger cohorts and extended follow-up periods is essential to refine treatment strategies and enhance patient outcomes for this complex pathology.
Introduction
Paranasal sinus mucoceles are benign pseudocysts that contain mucus or clear fluid, resulting from chronic mucus overproduction. This leads to gradual enlargement of the lesion, which displaces the surrounding tissues and erodes the bony walls of the sinus cavity.1,2 They can also be caused by the obliteration of the sinus ostium, which may be hereditary or acquired due to allergies, trauma, wounds, inflammation, or infection.1,3,4
Although paranasal sinus mucoceles are non-neoplastic inflammatory lesions, they can pose significant problems in critical orbital and cranial structures. They commonly originate in the frontal and ethmoid sinuses but may extend into surrounding spaces, posing risks to the orbit and nervous system if left untreated.2,4,5 The erosion of the lamina papyracea or sinus floors can lead to complications such as visual impairments, proptosis, and pain, while severe cases may result in intracranial penetration, risking compression of the frontal lobe and potential neurological deficits.2,3,5,6 Mucoceles of the paranasal sinuses are typically managed by maxillofacial or otorhinolaryngological surgeons. While intraorbital or intracranial extension is uncommon, comprehensive case series are scarce in the existing literature, which primarily consists of single case reports.1,7 -13
This study aims to address these gaps by enhancing the understanding of the clinical, radiological, and management aspects of mucoceles that extend into the orbit and cranial vault. By presenting additional cases, we seek to contribute valuable insights into the implications of mucoceles on surrounding structures and the multidisciplinary strategies employed for their treatment.
Methods
Study Design and Setting
This retrospective case series reviewed electronic clinical records of patients surgically treated for paranasal sinus mucoceles at our institution from July 1, 2013, to June 30, 2024. The study, approved by the Institutional Research Ethics Board (2024-10396), included patients aged 18 years and older with diagnosed mucoceles exhibiting intracranial or intraorbital extension who underwent endoscopic sinus surgery (ESS). Exclusions were made for inadequate documentation, lack of follow-up, or prior resections at other institutions. Data collected included demographics, comorbidities, presenting illness, lesion site and extension, imaging findings, surgical procedures, and postoperative outcomes. Information was retrieved from electronic medical records and clinician notes.
Statistical Analysis
Descriptive statistics summarized patient characteristics and symptoms reported during preoperative and postoperative follow-ups, using IBM SPSS version 23.0 for all analyses.
Patients and Results
Patient Demographics
After applying the exclusion criteria, a total of 10 diagnosed patients with paranasal sinus mucoceles, who underwent ESS performed by the same surgeon, were included for final analysis. The mean age was 65.80 ± 17.42 years (range = 42–95 years). Females (60%) were more affected than males (40%) in younger age groups, while an equal distribution was observed in older age groups (Figure 1). The patients exhibited diverse past medical histories and comorbidities, including conditions such as right maxillary sarcoma with prior cholecystectomy, anemia with chronic rhinosinusitis, atrial fibrillation, type 2 diabetes, and obesity. Other significant conditions included Graves' disease with ophthalmopathy, hypertension, congestive heart failure, asthma, post-herpetic neuralgia, and a history of multiple surgeries for various cancers and neurological conditions. Table 1 presents a summary of the past medical histories of the included patients.
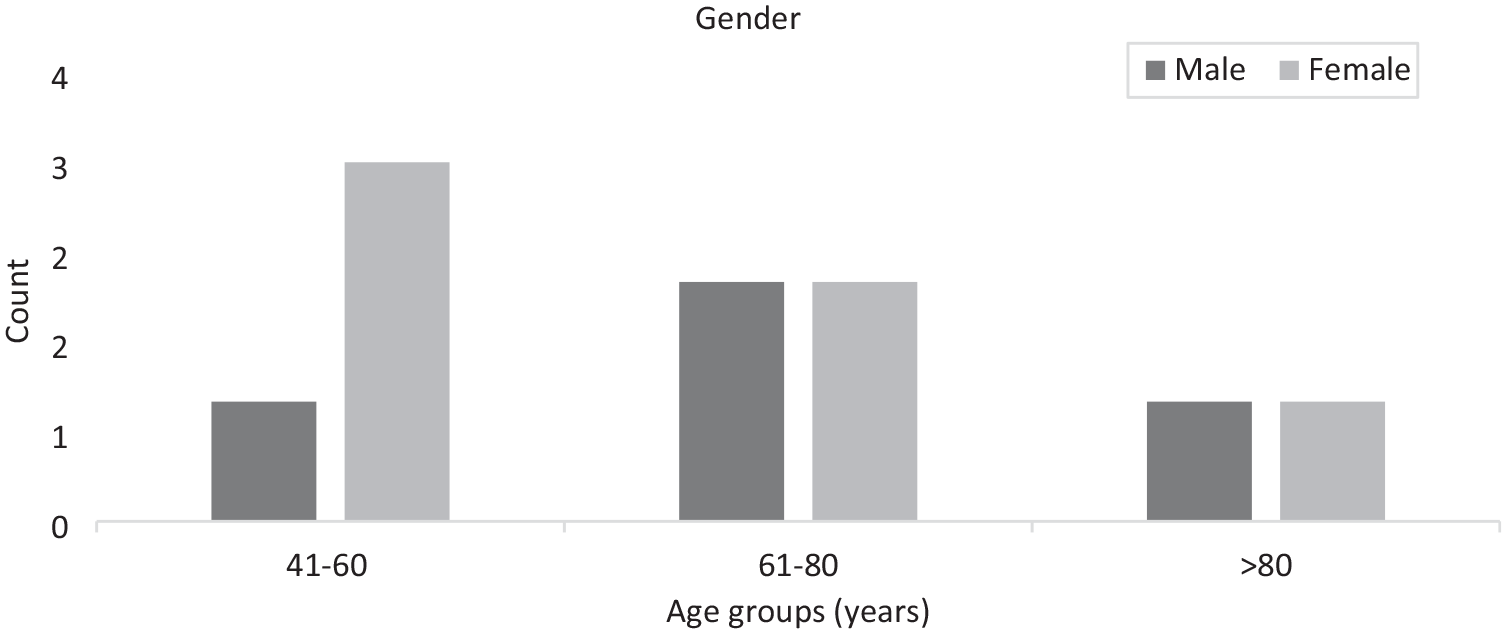
Gender distribution among different age groups.
Past Medical History.

Clinical Examination Observations
The primary complaints in patients with paranasal sinus mucoceles exhibiting intraorbital or intracranial extension were categorized into ophthalmological, rhinological, and neurological symptoms. Common findings included orbital swelling, vision changes, pain, nasal obstruction, and hyposmia (Table 2). Some patients presented with palpable frontal masses and minimal mucosal inflammation, while others showed normal mucosa without nasal polyps. Notable symptoms included proptosis and eye fullness, with 1 case involving ipsilateral nasal polyps.
Signs and Symptoms.

Distribution of Affected Sinuses
Among the ten patients, sinus involvement varied significantly, with frontal (50%), ethmoid (40%), and sphenoid (10%) sinuses being the most frequently affected. These cases required extensive surgical interventions due to intraorbital and intracranial extensions, including frontal mucoceles extending into the orbit and anterior cranial fossa, and ethmoid mucoceles causing proptosis and orbital cellulitis.
Imaging Findings
Radiological assessments revealed that 5 (50%) patients had intraorbital extensions, 2 (20%) had intracranial extensions, and 3 (30%) had both. Computed tomography (CT) scans consistently showed mass growth, orbital plate invasion, globe displacement, and bone erosion.
Pre and post-operative radiological images of 3 paranasal sinuses mucoceles are shown in Figures 2 to 4.
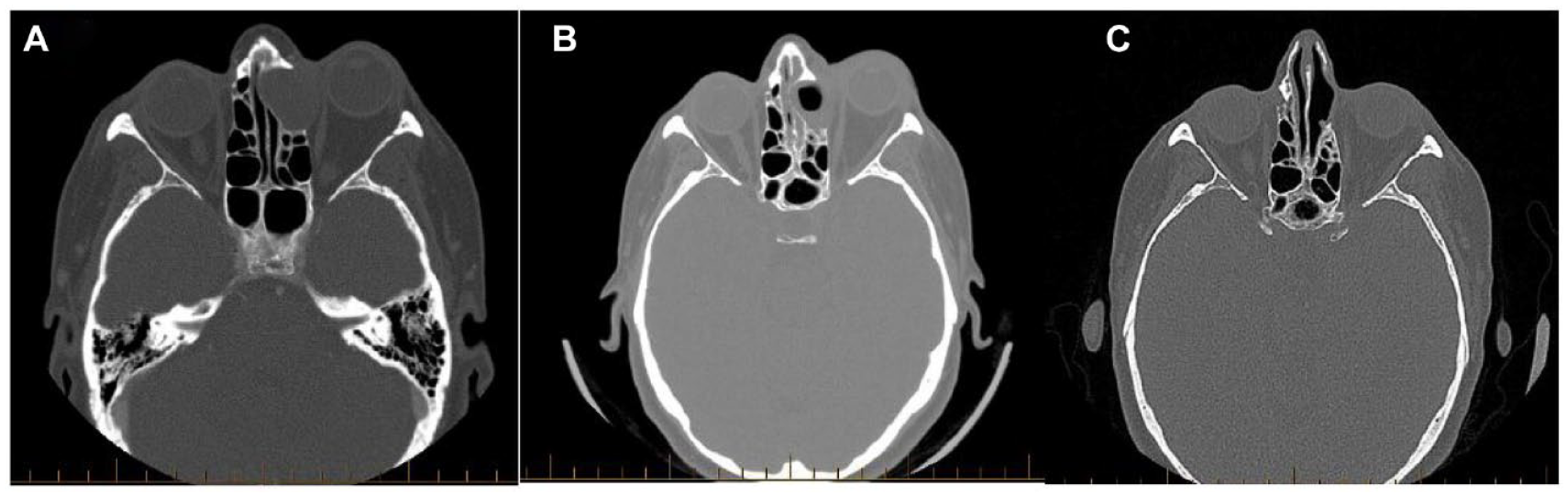
(A-C) Frontal mucocele with orbital extension. (A) Pre-operative CT Sinuses scan demonstrates a large mass in the left frontal sinus, eroding the sinus walls and causing proptosis of the left globe. There is notable expansion into the anterior ethmoid air cells without significant enhancement. (B) Post-operative CT shows residual soft tissue at the surgical site, with persistent proptosis and inflammation in the left orbit. No significant compression of the optic nerve is noted. (C) MRI findings reveal a drained mucocele with air content and inflammatory tissue. The lesion still protrudes into the left orbit, indicating mild to moderate proptosis but no acute inflammatory changes in the orbit.
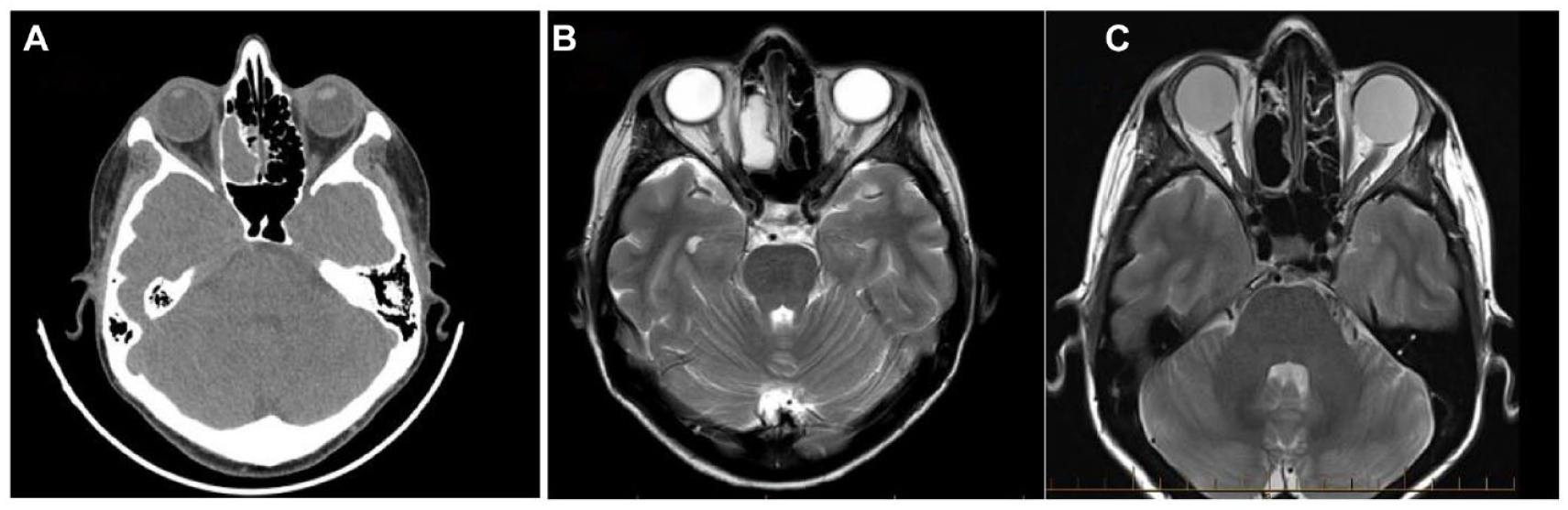
(A-C) Right ethmoidal mucocele. (A) Preoperative CT scan reveals a mass in the right ethmoidal air cells with smooth outlines, causing disruption of septations but no significant bony erosion. (B) Pre-operative MRI shows an expansile lesion in the right ethmoidal air cells with characteristic signal intensities, indicating a likely mucocele. (C) Post-operative MRI demonstrates resection of the ethmoid mucocele with minor residual mucosal inflammation in the ethmoids and no intracranial extension or orbital abnormalities.
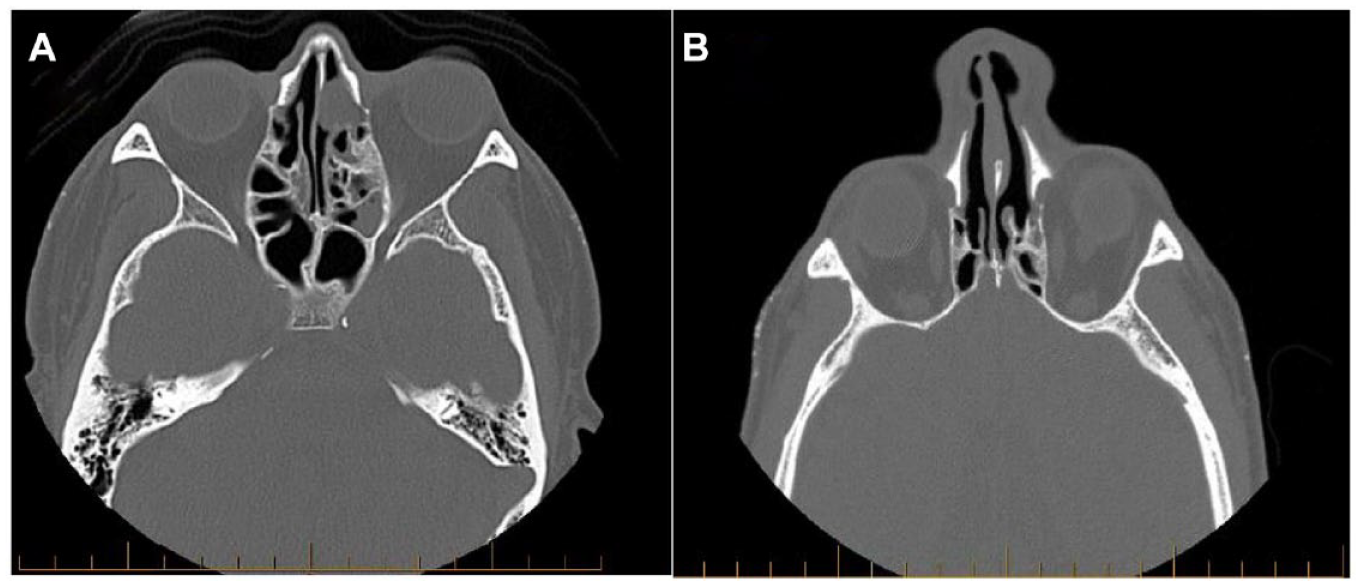
(A and B) Left frontoethmoidal mucocele. (A) Preoperative CT scan indicates a slow-growing lesion from the left anterior ethmoidal air cells expanding into the left frontal sinus and eroding the roof of the orbit, with possible muscle. (B) Post-operative CT findings reveal minor mucosal thickening and chronic changes in the left frontal sinus post-resection of the mucocele, with no signs of recurrence or significant disease in the paranasal sinuses.
Notably, maxillary sinus floor was absent in Case 1 due to prior surgery for right maxillary sarcoma, while Case 9 indicated a mass expansion in right frontal sinus, suspected to be metastatic neuroendocrine carcinoma, from the right upper lobe of the lung (Table 3).
Diagnostic Imaging Findings.

Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; PET, positron emission tomography.
Surgical Approaches and Outcomes
All ten patients underwent surgery for paranasal sinus mucoceles, with approaches tailored to the extent of intraorbital and intracranial involvement. The primary objectives were symptom alleviation, preservation of eyesight, and prevention of complications. Eight patients (80%) had unilateral functional endoscopic sinus surgery (FESS), while 2 (20%) underwent bilateral FESS (Table 4).
Surgical Approach.
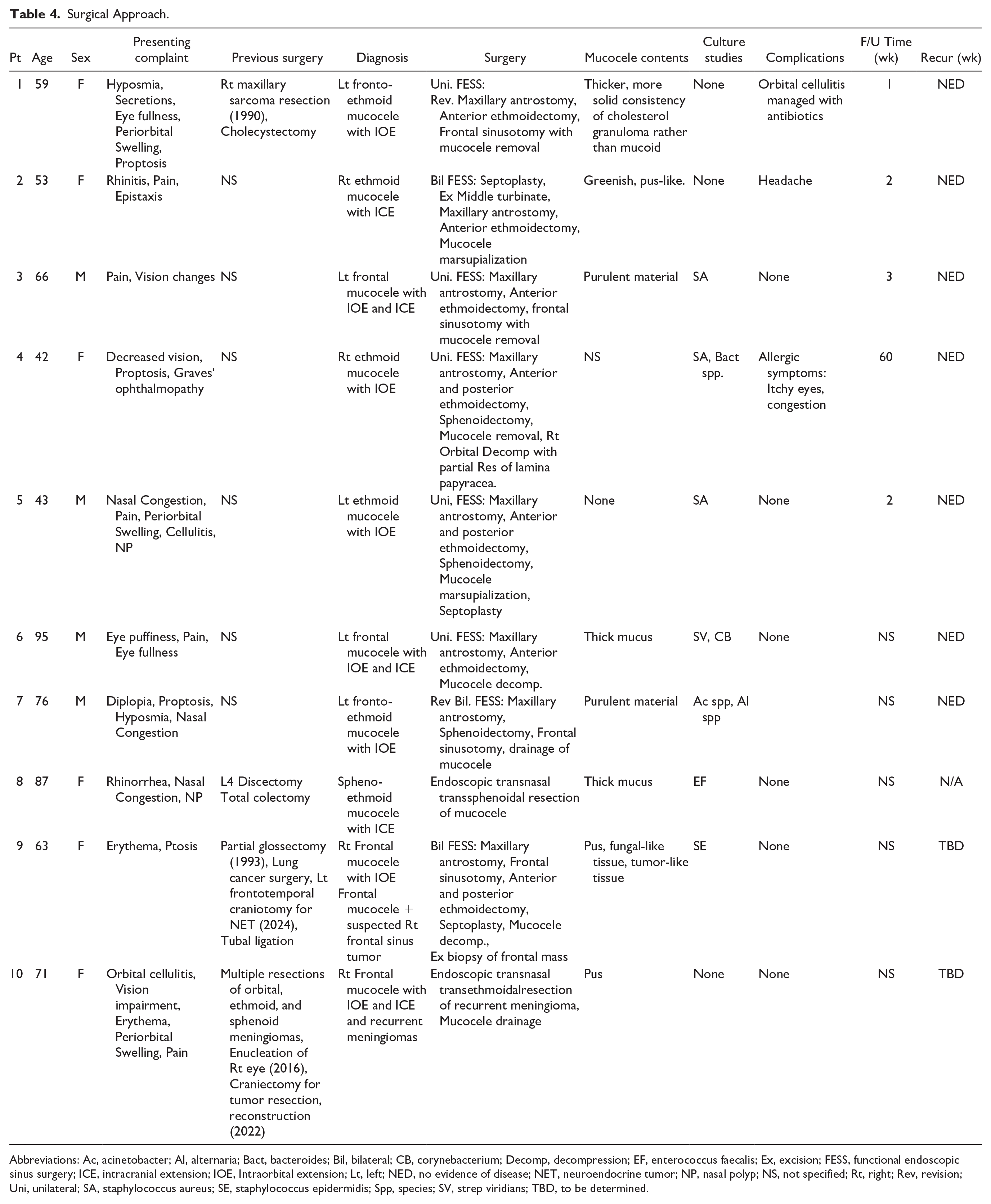
Abbreviations: Ac, acinetobacter; Al, alternaria; Bact, bacteroides; Bil, bilateral; CB, corynebacterium; Decomp, decompression; EF, enterococcus faecalis; Ex, excision; FESS, functional endoscopic sinus surgery; ICE, intracranial extension; IOE, Intraorbital extension; Lt, left; NED, no evidence of disease; NET, neuroendocrine tumor; NP, nasal polyp; NS, not specified; Rt, right; Rev, revision; Uni, unilateral; SA, staphylococcus aureus; SE, staphylococcus epidermidis; Spp, species; SV, strep viridians; TBD, to be determined.
Four patients had fronto-ethmoidal mucoceles and initially received unilateral FESS. Two of these had no mucoceles present during the initial surgery, but revision sinus surgery was done to address newly developed mucoceles following the initial sinus surgery over time and not due to any recurrences of mucocele. Intraoperative findings revealed varying mucous compositions. Microbiological analysis showed diverse results, with some cases exhibiting no microbial growth and others identifying specific bacteria like Staphylococcus aureus.
Recurrence was defined as the reappearance of mucoceles at the same anatomical location, confirmed by clinical symptoms or radiological evidence after the initial surgery during the follow-up period. Postoperative follow-ups were initially conducted weekly and subsequently spaced out over longer intervals (typically at 1 week, 3 months, and 6 months post-surgery, though these intervals varied by case). Postoperative outcomes were generally excellent, with symptoms resolved in all cases and no immediate complications reported. Follow-up was conducted for only 5 patients, 3 of whom complained of headache, itchy eyes, or orbital cellulitis, which were successfully managed with oral antibiotics. Two patients were recently diagnosed with paranasal sinus mucoceles and are under ongoing follow-up.
Discussion
Paranasal sinus mucoceles are benign, expansile, cystic lesions lined by mucoid-secreting respiratory epithelium. 14 The most widely accepted pathophysiological explanation for sinus mucoceles is the retention of mucus due to obstruction of sinus outlets, which can be caused by tumors, allergies, surgeries, nasal polyps, chronic inflammation, or trauma. 15 Paranasal sinus mucoceles exhibit slow growth patterns and can expand, infiltrating adjacent critical tissues like the orbit and skull base, leading to intracranial and intraorbital complications. 14
While mucoceles can affect individuals of all ages and genders, people between 40 and 70 years are most susceptible.2,16 Our study showed a predominance of females, with 40% of patients aged 40 to 60 years. The frontal and ethmoidal sinuses are most frequently affected, likely due to the long, convoluted drainage pathway of the frontal sinus, which is prone to occlusion.2,14,17
The location, size, and extent of infiltration into adjacent tissues contribute to the physical signs and symptoms of mucoceles. Expansion of the sinuses due to mucus buildup and pressure on neighboring tissues leads to ocular discomfort, proptosis, diplopia, periorbital edema, impaired visual acuity, and restrictions in ocular movement when the orbit is involved.2,14,18 Several patients in our study presented with these symptoms.
Mucoceles are diagnosed using clinical indicators, physical examination, and radiographic tests like CT scans and/or MRI, considered the most reliable modalities.6,14 CT scans typically show ovoid, well-defined, expansile lesions within the sinus cavity, with a density similar to brain tissue, while MRI findings include low T1 and high T2 signal intensities without gadolinium contrast enhancement.19,20 Our study patients underwent CT and/or MRI scans, revealing increased density, sinus expansion, orbital invasion, and sinus wall bone degradation, confirming the extensive and invasive nature of mucoceles, and underscoring the necessity for comprehensive assessment and intervention in such cases.
Observation is occasionally considered for smaller, asymptomatic mucoceles that do not infringing on critical structures. However, in the cases presented, all patients exhibited symptoms or anatomical involvement that warranted surgical intervention. The optimal treatment is surgical excision of obstructing partitions, with early intervention crucial in cases involving visual impairment. 21 Endoscopic sinus surgery is currently preferred due to its ability to reduce complications, minimize sinus injury, preserve sinus structure, avoid facial scarring, and enable endoscopic follow-up.2,14,22 In our study, FESS was employed to treat patients, with consistently positive postoperative outcomes, including symptom resolution and no recurrence during follow-up. Complications such as cerebrospinal fluid leakage, hemorrhage, ocular injury, retrobulbar hematoma, ocular abscess, and cellulitis may arise from nasal endoscopic surgery and should be promptly identified and managed. 2 One of our study participants developed orbital cellulitis post-surgery, leading to mild proptosis, which was treated with antibiotics. After discharge, the patient continued outpatient monitoring, and there was no recurrence of the condition. All of our mucoceles were managed quite effectively with wide marsupialization, and none had to resort to more invasive procedures such as modified Lothrop (Draf 3) or open surgery. Approaches like these are mostly taken for extensive bony involvement, inadequate access endoscopically, or intracranial complications (abscess or osteomyelitis). None of the aforementioned conditions were present in our patients.2,14,22
Finally, this case series illuminates the diverse clinical presentations, radiological features, and surgical outcomes of mucoceles with intraorbital and intracranial involvement. The varied anatomical complexities and associated challenges underscore the importance of thorough preoperative evaluation, meticulous surgical planning, and attentive postoperative monitoring to achieve favorable outcomes. Further research with larger cohorts and extended follow-up periods is warranted to refine treatment algorithms and enhance patient care in managing this complex disease entity.
Conclusion
Ten patients with paranasal sinus mucoceles exhibiting intraorbital or intracranial extensions, and presenting with ocular and nasal symptoms were treated endoscopically. Throughout follow-up, all patients experienced symptom improvement and were successfully treated without recurrence. However, 2 recent cases necessitate longer follow-up to assess recurrence status.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Committee Approval
This study was approved by the Institutional Research Ethics Board at the McGill University Health Centre (Approval Number: MP-37-2024-10396).