
Abstract
Ectopic pituitary adenoma is a condition characterized by the presence of an adenoma originating from extra-sellar pituitary cell residue from the migration of Rathke’s pouch. First described in 1909, ectopic pituitary adenoma is a very rare, largely unknown condition with a challenging diagnosis, that requires proving the absence of communication between the extra-sellar mass and the normal pituitary gland (or any of the intra-sellar contents). Here, we describe the case of a 38-year-old female who presented with symptomatic hyperprolactinemia in whom magnetic resonance imaging revealed a space-occupying mass in the sphenoid sinus with an empty sella turcica. Clinical information coupled with magnetic resonance imaging findings raised suspicion for the diagnosis, which was later confirmed through surgery (showing the absence of a breach in the sellar floor dura), and histology. Given the rarity of such cases, management is not standardized; however, most patients reported in the literature, as in our case, have undergone surgical treatment. This case report aims to provide an additional example to the existing literature on this rare condition, especially when it is associated with an empty sella turcica.
Introduction
Ectopic pituitary adenomas (EPAs) are defined as pituitary adenomas located outside the sella turcica, originating from remnants of Rathke’s pouch, and lacking any connection to the normal pituitary gland or its intra-sellar components.1,2 This characteristic distinguishes them from the much more common invasive pituitary adenomas that extend into the sphenoid sinus (SS). 1 EPAs are rare, with fewer than a hundred cases reported in the literature. Their association with an empty sella turcica is even rarer.1,3 The most frequent location is within the SS, accounting for approximately 40%–60% of cases in various series. 1 While clinical presentation, laboratory tests, and imaging can raise suspicion for the diagnosis, a definitive diagnosis can only be established through histopathology.1,3
Case report
A 38-year-old woman experiencing secondary amenorrhea and galactorrhea for the past 11 months visited the hospital. The patient underwent a general and gynecological physical examination finding nothing particular except for bilateral and multi-pore galactorrhea. The examination was followed by a pelvic and breast ultrasound, which returned normal results.
A comprehensive battery of biological tests was also conducted, revealing an elevation in prolactin levels at 320 ng/ml. Standard blood tests and the remaining hormonal panel showed no abnormalities.
Subsequently, a Magnetic resonance imaging (MRI) was requested to rule out a pituitary adenoma. It revealed a space-occupying mass involving the SS with an iso-signal on T1 and a slight hypersignal on T2-weighted sequence (compared to white matter) (Figure 1). The mass did not invade the walls of the SS nor the sella tucica floor; however, it was causing obstruction of the SS ostium with mucus retention (Figure 2). Additionally, the MRI showed an intact pituitary stalk which traverse a cerebrospinal fluid filled sella (infundibulum sign) with no pituitary gland visualized. Dynamic contrast-enhanced sequences were performed, demonstrating a normal enhancement of the pituitary stalk with the absence of intra-sellar pituitary parenchyma. The ectopic adenoma exhibited a low enhancement, with no visualization of the normal pituitary parenchyma around it. This observation aligns with the classical characteristics of macroadenomas, where the pituitary parenchyma is excessively stretched and thinned to the point of being imperceptible. (Figures 3 and 4).
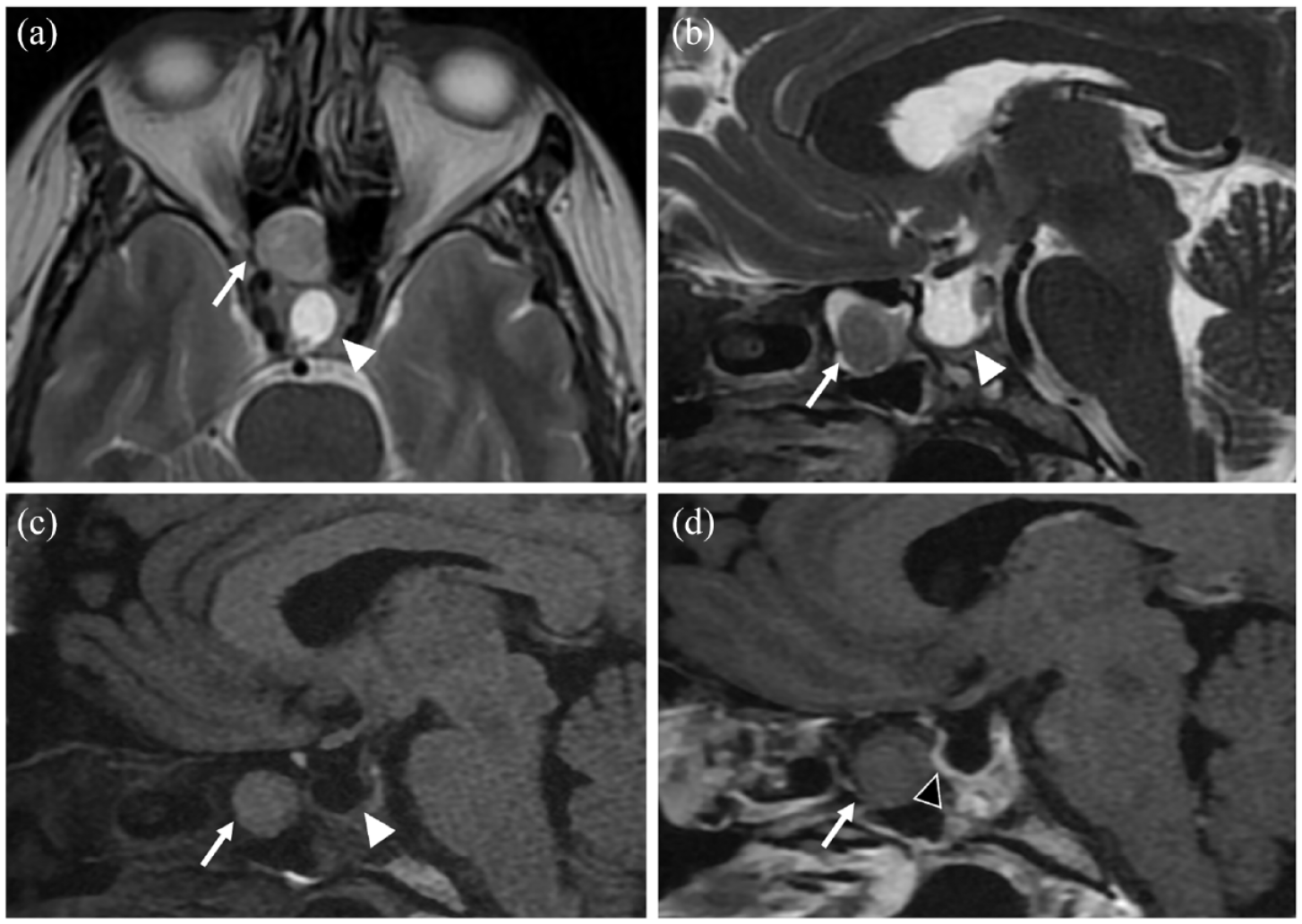
Axial T2-weighted image (a) and sagittal T2 (b), T1 FLAIR (Fluid-attenuated inversion recovery) (c) and T1 Fat-Sat GD+ (d) images with a focus on the sellar and sphenoid sinus (SS) regions. Visualization of a space-occupying mass in the right SS (arrow), the sella turcica is empty, only filled with cerebrospinal fluid (White arrowhead) ((a)–(c)). The injected sequence (d) shows a very mild enhancement of the mass, and does not visualize any sella turcica floor defect (Black arrowhead), which was confirmed during the surgical procedure.

Coronal T2-weigted image showing the pituitary adenoma (arrow) obstructing the sphenoid sinus ostium obstruction with mucous retention around the mass (arrow heads).

Coronal T2-weigted (a) and T1 Fat-Sat GD+ (b) images showing the pituitary stalk diving in the CSF filled sella, realizing the “infundibulum sign.”

Coronal Dynamic contrast-enhanced (DCE) sequences passing through the sella turcica (Column A) revealed the normal enhancement of the pituitary stalk and the absence of normal pituitary parenchyma inside the sella turcica. Additionally, slices passing through the ectopic adenoma (Column B) displayed a mild and persistent enhancement of the mass, without the presence of normal pituitary parenchyma around it.
Based on these findings, the diagnosis of EPA with an empty sella turcica was established.
Despite receiving medical treatment, the patient’s symptoms did not improve, she subsequently underwent surgical treatment via the transsphenoidal approach, the surgeon reported an intact sellar dura. The histopathological and immunohistochemical examination were in favor of a prolactinoma (Figure 5).

Image showing the histological appearance of specimens taken from this patient. It reveals the presence of diffusely growing adenoma cells with eosinophilic or chromophobe cytoplasm.
On follow-up consultations, the patient reported an immediate cessation of galactorrhea after the surgery, and a resumption of a normal menstrual cycle 3 months later.
Discussion
Pituitary adenomas are one of the most frequent intracranial neoplasms accounting for 10%–25% of cases, in contrast, EPAs are exceedingly rare (approximately 0.5% of all pituitary adenoma cases). 1 First described by Erdheim in 1909, EPA refers to the extra-sellar development of pituitary adenoma, the pituitary gland can either be normal or absent, in this case it is referred to as EPA with an empty sella turcica. The location of the lesion can vary, typically occurring outside the blood-brain barrier, it may be either intra- or extra-cranial.1,2
During the eighth week of gestation, the primitive pituitary gland divides into two parts, the pharyngeal and distal portion. The distal part forms Rathke’s pouch, which subsequently migrates upward to develop into the intra-sellar pituitary gland. The pharyngeal part usually persists as a small accessory gland embedded in the pharyngeal mucosa, devoid of endocrine activity. 2 In the case of an EPA, three scenarios can be described:
Extra-cranial EPA originates from the pharyngeal pituitary or from remnants of pituitary tissue retained within the craniopharyngeal canal during Rathke’s pouch migration. It can be found at varying heights along this migratory path. The most common location is the SS, but it can also be found in the nasal cavities or septum, nasopharynx, or within the sphenoid or petrous bone.
Intracranial EPA arises from retained glandular tissue remnants during Rathke’s pouch migration within the cranial cavity. Common locations include supra-sellar, para-sellar, or within the clivus.
EPA with an empty sella turcica is a particular case thought to result from the complete or near-complete retention of precursor pituitary tissue outside the sella turcica.
Clinical symptoms depend on the tumor’s endocrine status, location, and size. For EPAs in the SS, aside from secretory forms, they can be asymptomatic or may manifest with mild signs such as headaches, rhinorrhea, nasal obstruction, or even epistaxis. 3
In various series, 30%–90% of EPAs are non-secreting, while those that do secrete hormones, can produce the same hormones as the normal pituitary gland and thus can be the source of various types of secreting adenomas. The most common secretory form is Adrenocorticotropic hormone (ACTH) secreting adenomas, accounting for over 50% of EPA cases, followed by prolactinomas, endocrine-inactive adenomas, and GH-secreting adenomas.2–4
The MRI studies usually reveal a space-occupying mass, typically round or with a shape conditioned by its bony relationships, well-defined, with iso- or hypointensity on T1, and iso- or hyperintensity on T2-weighted sequence. Enhancement is typically mild and can be either homogeneous or heterogeneous. The bony adjacent structures may present some degree of remodeling—thinning, bulging, erosion, or even osteosclerosis. Importantly, no communication should be evident with the pituitary gland. MRI also enables the examination of the sella turcica content. Computed tomography (CT) scan is useful for assessing the sella turcica floor and for surgical planning.2,5,6
As explained earlier, the type of migration anomaly determines the type of EPA encountered. Extra-sellar forms involving the SS are by far the most frequent (approximately 50%–60% of cases), followed by EPAs in the septum or nasal cavity, intra-petrous EPAs, and intracranial supra-sellar or clival EPAs.
Differential diagnosis includes other SS masses, such as chordomas, chondromas, chondrosarcomas, craniopharyngiomas, mucoceles, fungal balls, and nasopharyngeal tumors. The absence of calcifications on CT is an important feature that can help exclude the first four differential diagnoses, while the appearance on T2 and enhancement patterns can differentiate EPA from mucoceles and fungal balls. EPAs should also be differentiated from invasive adenomas with sellar floor defects, that remain continuous with the gland.2,3
Medical treatment is typically considered as the first-line approach. For prolactinomas, bromocriptine can sometimes alleviate symptoms and reduce tumor volume. In cases of persistently elevated prolactin levels, ongoing symptoms, intolerance to medical treatment, or chiasmal compression, surgery is proposed. Surgical intervention represents the only curative treatment and is typically carried out through an endonasal approach. It also allows for the assessment of the sellar floor, an intact sellar dura being a crucial element in confirming the ectopic nature of the adenoma.2,6,7
In the case of an isolated EPA, surgical treatment is typically radical, and patients generally do not require hormonal replacement therapy post-surgery. However, this scenario differs when the EPA is associated with an empty sella turcica. In such cases, lifelong replacement therapy is mandatory, as the normal secreting pituitary parenchyma is usually resected along with the adenoma during surgery.1,6,7
Conclusion
EPAs are a rare subset within the spectrum of pituitary neoplasms. Their unique presentation outside the sella turcica, coupled with diverse clinical manifestations and hormonal profiles, challenges conventional diagnostic and therapeutic paradigms. The association with an empty sella turcica is rare but evocative and can guide toward the diagnosis. The management of EPAs often involves a combination of medical and surgical interventions, with the latter proving essential in cases of persistent symptoms or hormonal imbalance.
Footnotes
Acknowledgements
The authors thank his professors and colleagues who helped in the completion of this work.
Author contributions
B.I. Contributed to conception or design, acquisition, analysis, and interpretation, drafted the article, critically revised the article, and agrees to be accountable for all aspects of work ensuring integrity and accuracy; B.K. Contributed to conception or design, acquisition, analysis, and interpretation, drafted the article, and agrees to be accountable for all aspects of work ensuring integrity and accuracy; K.S. Contributed to conception or design, acquisition, analysis, and interpretation, drafted the article, and agrees to be accountable for all aspects of work ensuring integrity and accuracy; L.F.Z. Critically revised the article, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy; J.L. Authorized the author to use the case, critically revised the article, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy; E.A. O. Critically revised the article, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.