
Abstract
Our aim was to investigate the relationship between facial canal dehiscence (FCD) and surgical findings and procedures in patients with cholesteatoma. A total of 186 patients (118 males, 39.2 ± 15 years) who underwent surgery for advanced cholesteatoma between 2013 and 2018 were included in the study. The relationship between FCD and surgical findings was investigated via the surgical registries. The prevalence of FCD was 36.6% (68/186). The prevalence of FCD was 44%, and 13.2% for the patients who underwent canal wall down mastoidectomy (62/141) and canal wall up mastoidectomy (6/45), respectively (P < .001). Facial canal dehiscence was detected in 73.9% of the 23 patients who had a lateral semicircular canal (LSCC) defect (P < .001), in 61.9% of 21 patients who had a tegmen tympani defect, and in 58.1% of the 31 patients who had erosion on the posterior wall of the external auditory canal (EAC; P < .05). The prevalence of FCD was 3.1% in patients with isolated incus erosion, 59.1% in patients with erosion of malleus and incus, 60.7% in patients with erosion of stapes suprastructure and incus, and 43.2% in patients with whole ossicular chain deformation (P < .001). The defects on LSCC, EAC, tegmen tympani, and malleus and incus might be cautionary findings for the presence of FCD during cholesteatoma surgery.
Introduction
Cholesteatoma is the condition characterized by keratinized stratified squamous epithelium in the middle ear and/or neighboring cavities, which should not be present normally. Although it is a benign lesion, it may exhibit erosive behavior. 1 Therefore, it causes destruction on anatomical structures in the middle ear and mastoid region. The exact mechanism of mentioned damage is not yet known; however, the most commonly accepted theories include increased pressure and possible enzymatic erosion. 2 The integrity of the bone structure over the facial nerve is the barrier that protects the nerve from destructive effects of cholesteatoma and possible iatrogenic damages. The presence of cholesteatoma is shown to be the main cause for most patients with facial paralysis due to chronic otitis media (COM). 3 Facial paralysis may also occur as an iatrogenic complication during surgery, and it has higher incidence during cholesteatoma surgery than other ear surgeries. 4
There are several studies on facial nerve canal dehiscence (FCD) and COM in the literature. 4 –6 However, a heterogeneity is found in these literature in terms of cholesteatoma spread and cholesteatoma presence. Also, limited data are found in the literature about the relationship between FCD and other damaged anatomical structures in cases with cholesteatoma. Therefore, the aim of this study was to evaluate the possible relationship between FCD and other damaged anatomical structures in patients with advanced cholesteatoma.
Materials and Methods
This was a retrospective study of patients with cholesteatoma advanced both to middle ear and to mastoid bone according to the intraoperative findings. One hundred eighty-six patients who underwent surgery for advanced cholesteatoma between January 2013 and November 2018 were included in the study. For patients who had a history of repetitive surgeries, only the data of the first operation performed in our clinic were used. The information regarding age, gender, operation side, and surgical information was recorded. Although all the patients had computed tomography (CT) scan before surgery, the data about the presence of FCD, the integrity of the posterior wall of the external auditory canal (EAC), lateral semicircular canal (LSCC), and each of the structures forming the ossicular chain were investigated from the surgical records. All the surgical records were written according to the intraoperative findings. The presence of the FCD was determined according to the microscopic evaluation and the palpation of the facial canal. The surgeries were classified as canal wall up (CWU) and canal wall down (CWD) mastoidectomy in accordance with preservation of the posterior wall of EAC. Patients were grouped as children (<18 years) and adults (>18 years). The location of the dehiscence was determined as tympanic region or mastoid region, or both. Ossicular damages were classified as incus defect, incus and malleus defect, suprastructure of incus and stapes, and total ossicular defect.
Statistical Analysis
SPSS 21.0 (IBM, Corp., Armonk, NY) software was used for statistical evaluation. Chi-square test and independent samples t test were used to determine whether there was a statistically significant difference between the groups. Value of P < .05 was accepted as statistically significant.
Results
One hundred eighty-six patients (68 females and 118 males) were included in the study. The ratio of males to females was 1:7. The mean age of the patients was 39.2 ± 15 years. Facial canal dehiscence was clearly identified in 68 (36.6%) patients, and the most common location was the tympanic segment (61 from 68 patients, 89.7%). There was no significant difference in FCD presence according to gender and age groups (Table 1).
The Relationship of the Investigated Parameters With Facial Canal Dehiscence.
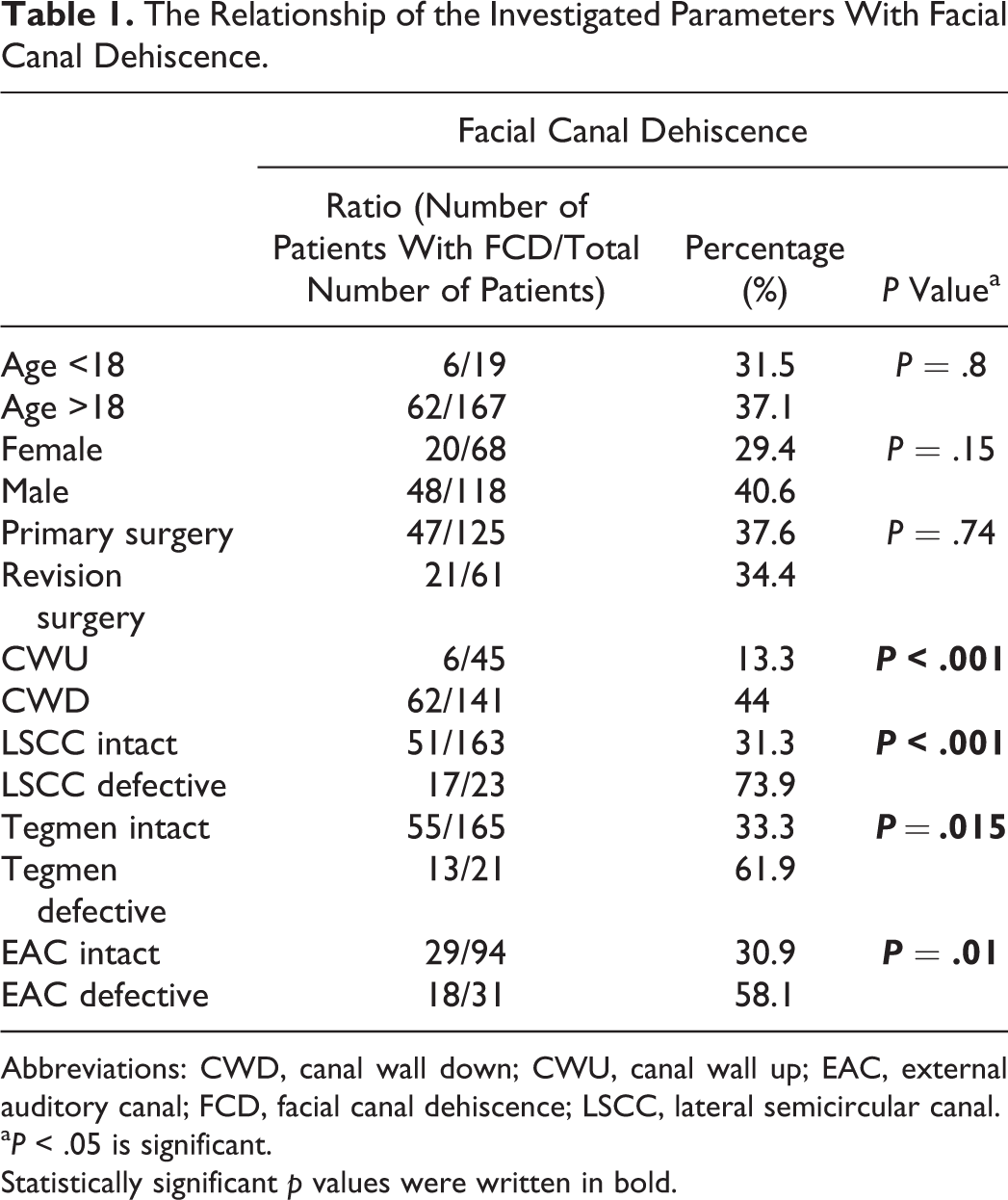
Abbreviations: CWD, canal wall down; CWU, canal wall up; EAC, external auditory canal; FCD, facial canal dehiscence; LSCC, lateral semicircular canal.
a P < .05 is significant.
Statistically significant p values were written in bold.
Relation of Facial Canal Dehiscence and Surgical Procedures
Canal wall down mastoidectomy was performed in 141 (75.4%) patients, whereas CWU mastoidectomy was performed in 45 (24.6%) patients. Facial canal dehiscence was detected in 62 (44%) patients who underwent CWD mastoidectomy and in 6 (13.3%) patients who underwent CWU mastoidectomy (P < .001).
Of 186 patients, 125 underwent operation for primary and 61 had revision surgery. Facial canal dehiscence was observed in 47 (37.6%) of the 125 primary surgery cases and in 21 (34.4%) of the 61 revision surgery cases (P = .74; Table 1). Considering ossicular chain reconstruction, only 5 (7.4%) of the 68 patients with FCD underwent ossicular chain reconstruction, while 25 (21.2%) of the 118 patients without FCD underwent ossicular chain reconstruction (P = .013; Table 2).
The Relationship of Facial Canal Dehiscence and Ossicular Chain Reconstruction.
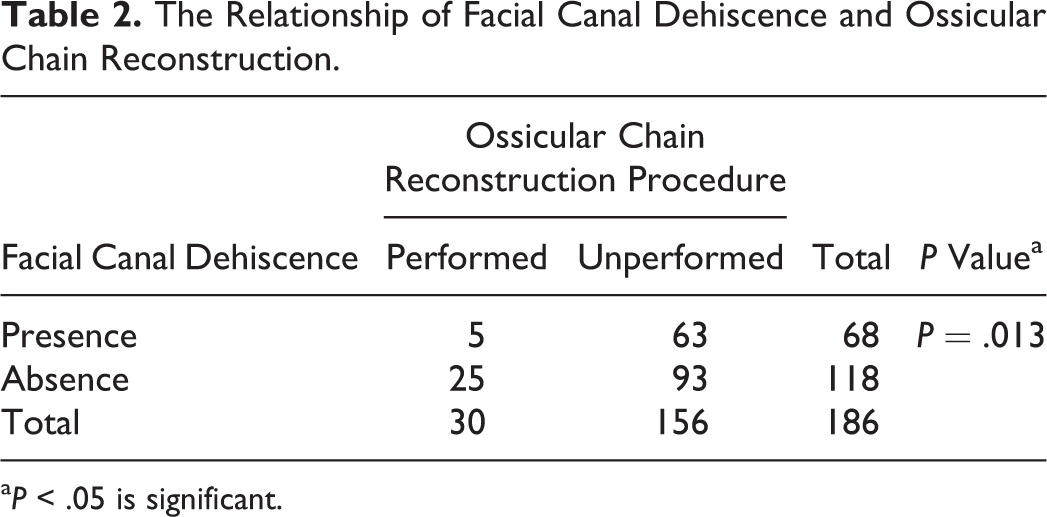
a P < .05 is significant.
Relation of Facial Canal Dehiscence and Surgical Findings
Lateral semicircular canal fistula was detected in 23 (12.4%) patients. Facial canal dehiscence was observed in 51 (31.3%) of the 163 patients without LSCC fistula and in 17 (73.9%) of the 23 patients with LSCC fistula (P < .001; Table 1).
In total, 21 (11.3%) patients had tegmen tympany defect. Facial canal dehiscence was observed in 55 (33.3%) of the 165 patients without tegmen tympany defect and in 13 (61.9%) of the 21 patients with a tegmen tympani defect (P = .015; Table 1).
Thirty-one (31/125, 24.8%) patients had erosion on posterior wall of EAC. Facial canal dehiscence was observed in 18 (18/31, 58.1%) of these patients. Facial canal dehiscence was found in 29 (30.9%) of the 94 patients who had no erosion on the posterior wall of EAC (P = .01; Table 1).
The incus was the most eroded (84.9%) ossicle, followed by malleus (67.2%) and stapes (61.3%). The prevalence of FCD was observed as 8.7%, 3.1%, 59.1%, 60.7%, and 43.2% for the patients with intact ossicular chain, with isolated incus erosion, with a defect of malleus and incus, with the erosion of suprastructure of stapes and incus, and with total erosion of ossicular chain, respectively (P < .001; Table 3).
The Relationship Between Ossicular Chain Defect and Facial Canal Dehiscence.
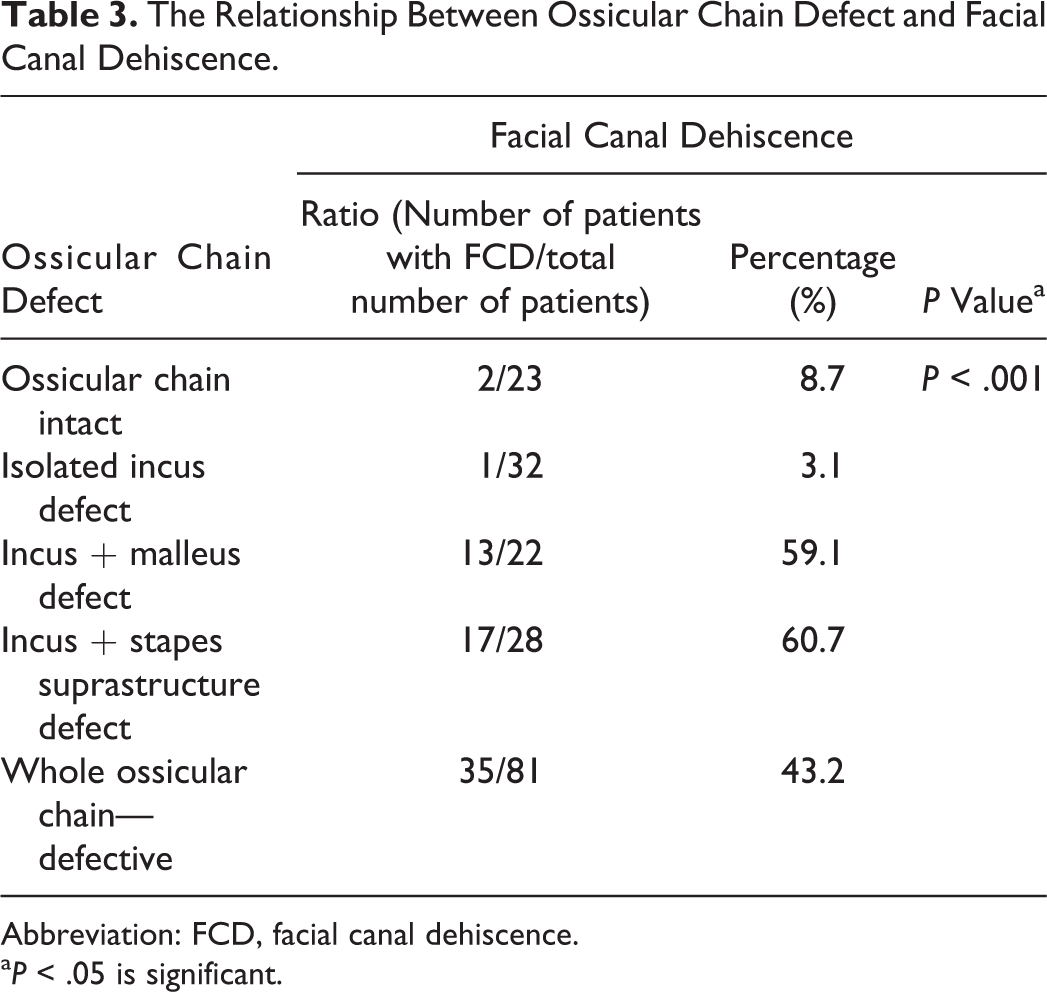
Abbreviation: FCD, facial canal dehiscence.
a P < .05 is significant.
Discussion
According to our study, we found that (1) FCD was found more common in patients with LSCC defect, (2) FCD was also found more common when noticed that EAC and tegmen tympany was destructed by cholesteatoma, (3) moreover, FCD was found more common especially in patients with the erosion of suprastructure of stapes and incus.
The primary causes of FCD are congenital disorders, infection, and inflammatory diseases. In addition, ear surgeries and erosive lesions, such as cholesteatoma, have also been identified among its main causes. Moreover, it was reported that FCD can be observed not only in patients with ear disease but also in healthy individuals. 7 –10
According to the current literature, the prevalence of FCD was found between 8.9% - 21.1% and 18.4% - 37.2% in patients who underwent surgery for COM and cholesteatoma, respectively. 4,11 –15 In the present study, we included patients with advanced cholesteatoma and we found that the rate of FCD was 36.6%.
Facial paralysis is one of the most feared complications of ear surgeries and iatrogenic facial nerve injury was reported as 0.6% to 3.6% in the literature. 4 Computed tomography is one of the most commonly used method to evaluate the presence of FCD before surgery. However, there are studies showing that CT may be inadequate for providing information. 7 Therefore, cautionary surgical findings, which might be related to FCD, should be carefully evaluated to reduce the facial nerve injury during surgery. During the surgical procedure, the presence of defects on EAC, tegmen tympany, LSCC, and ossiculer chain was noticed before the cholesteatoma sac removed over the facial canal.
Facial canal dehiscence is most frequently observed in the tympanic segment. Baxter observed the rate of tympanic segment dehiscence as 91% among the temporal bones with FCD in their histopathologic study included 535 temporal bones. 10 The prevalence of tympanic segment dehiscence was found as 74% and 87.2% in patients with FCD, respectively. 9,4 We found that the rate of tympanic segment dehiscence was 89.7% in patients with FCD. As known, there was a close anatomical relationship between the facial canal and the cholesteatoma located in the tympanic region and tympanic segment is more susceptible to mechanical injury. 14
Facial Canal Dehiscence and Surgical Procedures
We performed mastoidectomy in all patients with cholesteatoma included in our study. Therefore, we grouped our patients according to CWU and CWD mastoidectomy techniques. The rate of patients who underwent CWD (75.4%) was higher than CWU due to the fact that majority of patients admitted to our clinic had advanced cholesteatoma. In our study, FCD was observed in 13.3% of patients who underwent CWU mastoidectomy and in 44% of patients who underwent CWD mastoidectomy.
In the study performed by Gülüstan et al, no significant difference was observed at the rate of FCD between CWD and CWU mastoidectomy applied groups. 6 However, we observed a statistically significant difference between these surgical procedures in terms of FCD presence. We thought that including patients with advanced cholesteatoma in our study was the result of this significant difference. Relevant with the literature, we did not observe any significant difference between primary surgery and revision surgery cases in terms of FCD. 4,11,14,15
In the present study, we observed that only 5 (7.4%) of the 68 patients with FCD underwent ossicular chain reconstruction, while 25 (21.2%) of the118 patients without FCD underwent ossicular chain reconstruction. We thought that placing a prosthesis or nonanatomic bone block might be avoided due to the close anatomical neighboring of tympanic segment of the facial nerve and the oval window. These data suggest that the presence of FCD might be an independent parameter that could indirectly affect postoperative hearing thresholds.
Facial Canal Dehiscence and Surgical Findings
In our study, there was also a strong statistical relation between LSCC fistula and FCD as compatible with the literature. 6,11,13,15 The evaluation of LSCC is easier than the facial canal on CT. Moreover, LSCC is easier to be pointed during surgery and it is an anatomic structure previously pointed in terms of the steps followed in the surgical procedure of mastoidectomy. Therefore, LSCC fistula is a very important indicator in terms of FCD.
Ossicular chain damage is also common in patients with cholesteatoma. 16,17 An intact ossicular chain was detected only in 23 patients and the prevalence of ossicular chain damage was determined as 87.6% in the present study. Also, the prevalence of malleus, incus, and stapes defects was 67.2%, 84.9%, and 61.3%, respectively.
There was no significant relation between FCD and isolated incus defect. However, the rate of FCD has increased considerably when the incus or stapes suprastructure was damaged together. Furthermore, the defect of malleus and incus together has found to be an important indicator of FCD in the present study.
Conclusions
A defect on the posterior wall of EAC, LSCC, or tegmen tympany might be important cautionary surgical findings for the FCD. In addition, incus defect with stapes suprastructure or incus defect with malleus was also an important indicator for FCD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.