
Abstract

Keywords
Significance statement
Congenital EAC atresia with coexistent congenital cholesteatoma is a rare clinical entity among diseases of the temporal bone. The diagnosis and management of such conditions are extremely challenging. Surgeons should be extremely cautious regarding the possibility of facial nerve anomalies in such cases. A precise preoperative radiological imaging with HRCT temporal bone and MRI is essential for both the planning of the surgery and the prevention of complications in such situations.
Case report
A 14-year-old young male patient came to the otolaryngology department with bilateral progressive hearing loss since childhood. He was comfortable having a telephone conversation; however, it was difficult for him to understand conversations in a noisy environment. He also complained of intermittent episodes of pain in his left ear. He denied any symptoms of headache, tinnitus, vertigo or facial asymmetry. Examination of the ears revealed a Marx grade 1 microtia and bilateral external auditory canal (EAC) atresia. A bilaterally preauricular sinus was seen at the root of the helix (Figure 1A). TM could not be visualized due to atresia of the EAC. Bilaterally, facial nerve functions were normal with no mastoid tenderness. The tuning fork test elicited bilateral Rinne negative and Webers was lateralised to the left ear. His audiogram showed bilateral severe degree conductive hearing loss (right 63.8 dbHL and left 68.5 dbHL) (Figure 1B). The high-resolution computed tomogram (HRCT) of the temporal bone showed soft tissue opacification in the middle ear and the mastoid on the left side. HRCT also showed features of bilateral microtia, severe stenosis of the EAC and dysplastic ossicles (Figure 1C and D). Diffusion-weighted sequence of magnetic resonance imaging (MRI) of the brain confirmed the diagnosis of cholesteatoma in the middle ear and mastoid. Bilaterally, inner ear anatomy, 7th and 8th complexes were also normal on both sides on MRI (Figure 1E and F). Echocardiography, chest radiography, and ultrasound of the neck and abdomen revealed no additional congenital anomalies, ruling out syndromic causes. The diagnosis of left congenital cholesteatoma with preexistent congenital ear anomaly was made. (A) Clinical image showing grade 1 microtia with a preauricular sinus and EAC atresia. (B) Pure tone audiogram showing bilateral conductive hearing loss. (C, D) HRCT temporal bone (C) axial view (D) coronal view showing bilateral EAC atresia (red arrow), dysplastic ossicles with dehiscent floor in the middle ear (yellow arrow) and (E, F) MRI brain (E) T2 weighted and (F) DWI drive sequence axial view showing hyperintensity in the middle ear and mastoid (green arrow). EAC: External Auditory Canal; MRI: magnetic resonance imaging; HRCT: high-resolution computed tomogram.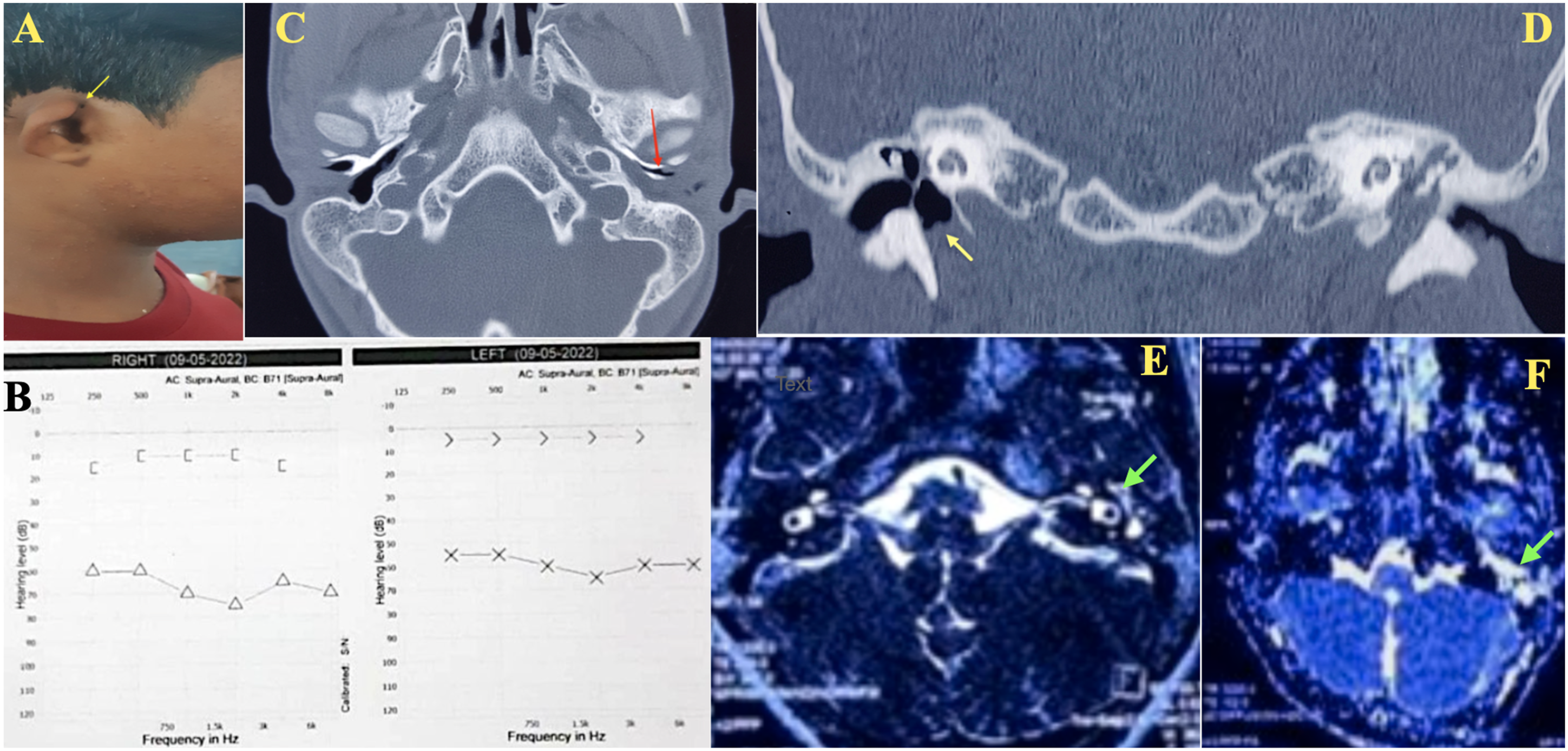
Surgical management
He underwent modified radical mastoidectomy in the left with type 4 tympanoplasty with preauricular sinus excision and meatoplasty under general anaesthesia. Intraoperatively, the entire course of the facial nerve appeared to be dehiscent (Figure 2). The ossicles were dysplastic with malleus attached to the anterior wall of the EAC. Only the stapes footplate was present. An accessory canal was seen communicating with the neck muscles in the infratemporal fossa just posterior to the bony atretic EAC (Figure 2). The cholesteatoma sac, which was seen in the middle ear and mastoid, was excised in total and sent for histopathological examination (HPE). The defect in the floor of the EAC was reconstructed with cartilage, perichondrium, and temporal fascia graft. Haemostasis was obtained and the wound was closed in layers. Postoperatively, the patient had temporary grade 2 House Brackman facial nerve palsy that recovered to normal within a week. HPE findings confirmed the diagnosis of cholesteatoma. (A, B) Intraoperative findings showing chordatympani nerve (CT), accessory extra canal between mastoid and atretic external auditory canal with dehiscent tympanic and mastoid segment of the facial nerve (FN).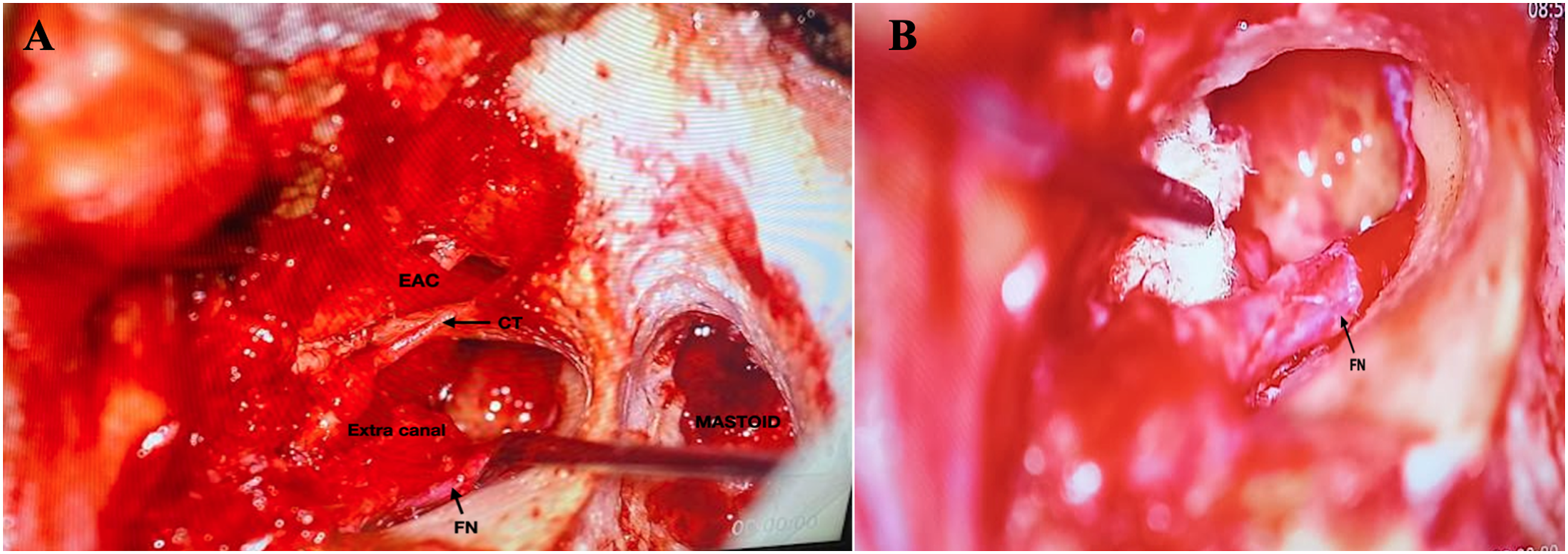
Discussion
Congenital EAC atresia is a rare condition with an incidence of 1 in 10 000 to 20 000 live births. Bilateral occurrence is more common than unilateral. 1 Schucknet 2 and other reported literature mention that 4 to 7% of cases of congenital EAC atresia also have congenital cholesteatoma, making it one of the rare diseases of the temporal bone. 2 -4 The diagnosis of congenital cholesteatoma with canal atresia is very challenging. Imaging with DWI brain magnetic resonance imaging and temporal bone HRCT is helpful in confirming the diagnosis of cholesteatoma. EAC develops embryologically from invagination of the ectoderm of the first pharyngeal pouch. Failure to recanalize the EAC at the 28th week of gestation leads to congenital EAC atresia. 2
Congenital cholesteatoma is a rare diseased condition arising primarily from the epithelial cells originating from ectodermal origin in the petrous temporal bone. When canal atresia is associated with cholesteatoma, patients present late with complications such as facial nerve palsy or hearing loss. Congenital dehiscence of the facial nerve tympanic segment is the most common facial nerve abnormality seen among congenital external ear abnormalities. For hearing rehabilitation in children with congenital external ear anomalies, bone anchoring hearing aids are the available treatment option. In this case, a surgical intervention was planned due to the presence of a congenital cholesteatoma.
Conclusions
In conclusion, even though both of the aforementioned conditions can occur on their own, the presence of both together is uncommon and requires a high level of suspicion, supported by HRCT and MRI images, to confirm the diagnosis. In such scenarios, the surgeon should be extremely cautious regarding the possibility of facial nerve anomalies, and thus a precise preoperative radiological evaluation is essential for both the planning of the surgery and to prevent complications.
Footnotes
Acknowledgements
The authors thank the faculty, the patient and the attendants for accepting the publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from the patient.