
Abstract
We investigated whether cholesteatoma is associated with sensorineural hearing loss (SNHL) and the effects of a lateral semicircular canal (LSCC) fistula, destruction of stapes, localization of cholesteatoma, and air–bone gap (ABG) size on SNHL. The charts of 159 patients who had received surgery for unilateral cholesteatoma were examined retrospectively. In all patients, air conduction and bone conduction (BC) thresholds in both ears were measured at 500, 1000, 2000, and 4000 Hz. Differences in BC thresholds between ears with cholesteatoma and contralateral ears were calculated. Demographics, localization of cholesteatoma, presence of LSCC fistula, condition of stapes, and ABG size on the affected ear were evaluated. There were significantly greater BC thresholds in ears with cholesteatoma than in normal ears for each frequency. Comparing the average BC differences at the different cholesteatoma locations, there were significant differences between the tympanic cavity + all mastoid cell group and attic, attic + antrum, and tympanic cavity + antrum groups. The BC differences at 4000 Hz were significantly high in patients with LSCC fistula. There were no significant relationships between the condition of the stapes and BC differences at any frequencies. There were significant correlations between average ABG and BC threshold differences at all frequencies. A significant relationship was found between cholesteatoma and SNHL. Patients with advanced cholesteatoma had significantly higher levels of SNHL. The BC threshold differences increased with increases in the ABG.
Keywords
Introduction
Cholesteatoma is the accumulation of keratinizing stratified squamous epithelium in the middle ear or other pneumatized areas of the temporal bone. Of the various types of hearing loss, typically conductive hearing loss is accompanied by cholesteatoma, and it is typically associated with ossicular chain erosion or impairment of normal ossicular mobility. 1 However, sensorineural hearing loss (SNHL) may also occur. Paparella et al 2 suggested that inflammatory cell and mediator penetration of the otic capsule through the round window membrane is associated with cochlear dysfunction. Similarly, SNHL may be due to penetration of toxic agents through the round window membrane, disease-related destruction of the bony framework, or increases in the functional mass of the ossicular chain, resulting in changes in the resonant frequency and increased bone conduction (BC) thresholds, similar to the Carhart effect. 3 -6 The association between chronic otitis media (COM) and SNHL has been studied by many researchers. 1,7 -16 Some have reported statistically significant SNHL on the side of the COM, compared to intact ears, 1,7 -14 whereas others have not. 15,16 Although some studies have differentiated COM with and without cholesteatoma, 7,9 -15 few have evaluated SNHL in patients with cholesteatoma, 1,8 and the relationship between SNHL and cholesteatoma is not yet clearly understood. 1,8,14 We assessed whether cholesteatoma is associated with SNHL and investigated the effects of a lateral semicircular canal (LSCC) fistula, destruction of stapes, localization of cholesteatoma, and air–bone gap (ABG) size on SNHL.
Patients and Methods
Patients who had been operated on for unilateral COM in the otolaryngology clinic of a tertiary care center between July 2007 and July 2017 and had cholesteatoma during surgery were included in the study. Patient files were reviewed retrospectively. All patients who were included in the study had histopathologically confirmed cholesteatoma. Patients with unilateral COM without cholesteatoma, bilateral COM with cholesteatoma, bilateral adhesive otitis media and/or retraction pockets, congenital cholesteatoma, history of head trauma, noise exposure, use of ototoxic drugs, familial hearing loss, or previous ear surgery were excluded.
Based on patient files, age, sex, the side of the operated ear, and other findings were determined. The data were examined in terms of the LSCC fistula, the localization and incidence of cholesteatoma, and the condition of the stapes. The localization of cholesteatoma was classified as attic, attic + antrum, attic + meso-hypotympanum (tympanic cavity), tympanic cavity + antrum, and tympanic cavity + all mastoid cells. The condition of the stapes was classified as intact or defective. Audiometric data were collected from patients’ preoperative audiometric evaluation. To eliminate effects of environmental, occupational, and age-related factors on hearing status, healthy contralateral ears were taken as controls.
The collected data included air conduction (AC) and BC thresholds in each ear at frequencies of 500, 1000, 2000, and 4000 Hz. Differences in BC thresholds between ears with cholesteatoma and healthy ears were calculated. The average BC (BC-A) in each ear was calculated for each patient at 500, 1000, 2000, and 4000 Hz, and the difference in BC-A between the ear with cholesteatoma and the healthy ear was calculated. Discrimination scores were noted for diseased and healthy ears. The ABG was calculated as the difference between the AC and BC thresholds at 500, 1000, and 2000 Hz for diseased ears. Informed consent was not obtained from patients because the study was retrospective, and the data were obtained from patient files. The hospital’s Research Ethics Committee approved this study (protocol number 2017/228).
Statistical analyses were performed using MedCalc Statistical Software version 12.7.7 (MedCalc Software bvba, Ostend, Belgium). To compare BC thresholds, we used the Wilcoxon test. We used the Kruskal-Wallis test to compare the BC differences among the audiometric frequencies and localizations of the cholesteatoma and BC-A differences. To determine the relationship between BC differences and the condition of the stapes and LSCC fistula, we used the Mann-Whitney U test. To correlate ABG with the BC differences, we used the Spearman rho test. A P < .05 was considered statistically significant.
Results
In total, 159 patients were eligible for this study. There were 89 (55.9%) males and 70 (44.02%) females with a mean age of 32.3 years (8-66 years). Overall, 98 (61.6%) had surgery on their right ear and 61 (38.3%) had surgery on their left ear. Table 1 shows paired mean BC thresholds for diseased and healthy ears across all frequencies (500, 1000, 2000, and 4000 Hz). There were greater BC thresholds in ears with cholesteatoma than in normal ears at each frequency. All of the differences were statistically significant (Wilcoxon P < .001). However, there was no significant difference in BC between ears with/without cholesteatoma at any frequency (Kruskal-Wallis P = .211). Mean BC differences were 10.9, 10.7, 11.8, and 12.9 dB at 500, 1000, 2000, and 4000 Hz, respectively. The presence of cholesteatoma was associated with lower discrimination scores compared to contralateral ears (Wilcoxon P < .001). The cholesteatoma was located in the attic in 9 (5.6%) patients, in the attic + antrum in 8 (5%) patients, in the attic + meso-hypotympanum (tympanic cavity) in 13 (8.1%) patients, in the tympanic cavity + antrum in 83 (52.2%) patients, and in the tympanic cavity + all mastoid cells in 46 (28.9%) patients. The mean BC-A differences were 5.8, 7.1, 11.5, 10.9, and 15.8 dB for attic, attic + antrum, tympanic cavity, tympanic cavity + antrum, and tympanic cavity + all mastoid cells, respectively. The BC-A differences significantly differed at the different cholesteatoma locations (Kruskal-Wallis P = .027; Table 2). However, post hoc binary analyses, which were performed to analyze this difference, revealed that there were significant differences between the tympanic cavity + all mastoid cell group and attic group (Mann-Whitney U P = .005), tympanic cavity + all mastoid cell group and attic + antrum group (Mann-Whitney U P = .027), and tympanic cavity + all mastoid cell group and tympanic cavity + antrum group (Mann-Whitney U P = .013). No significant differences were evident among the other groups (Mann-Whitney U P > .05 with Bonferroni correction).
Comparison of Bone Conduction Thresholds Between Ears With Cholesteatoma and Contralateral Ears at Different Frequencies.a
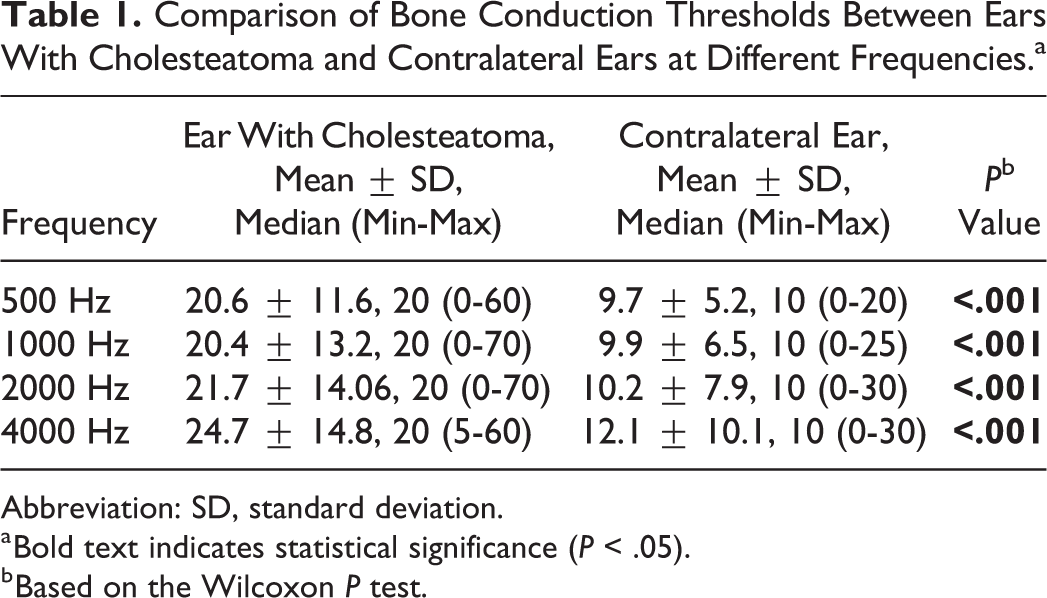
Abbreviation: SD, standard deviation.
a Bold text indicates statistical significance (P < .05).
b Based on the Wilcoxon P test.
Relationship Between Average Bone Conduction Difference and Localization of Cholesteatoma.a

Abbreviations: BC-A difference: average bone conduction difference at 500, 1000, 2000, and 4000 Hz; SD, standard deviation.
a Bold text indicates statistical significance (P < .05).
b Based on Kruskal-Wallis tests.
The stapes was damaged (partially or completely) in 97 (61%) patients. There were no significant relationships between the condition of the stapes and BC differences at any frequencies (Mann-Whitney U P = .289 500 Hz, P = .750 1000 Hz, P = .799 2000 Hz, P = .737 4000 Hz).
The LSCC fistulas were detected in 12 (7.5%) patients. When we grouped the patients according to the presence of LSCC dehiscence, the difference between BC values was significant at 4000 Hz (Mann-Whitney U P = .019). No significant difference in BC values was evident at 500, 1000, or 2000 Hz (Mann-Whitney U P > .05). Among the 12 patients, 7 had cholesteatoma localized in the tympanic cavity + antrum, 4 in the tympanic cavity + all mastoid cells, and 1 in the attic + antrum. Of 12 patients, 11 also had a stapes defect. There was a correlation between the ABG average and BC differences at all frequencies (Spearman rho P < .001).
Discussion
Cholesteatoma is an aggressive disease. 14 Although some studies have suggested an association between cholesteatoma and SNHL, there is still a lack of consensus. Eisenman and Parisier 1 suggested that BC thresholds might be increased at high frequencies due to inflammatory mediators passing through the oval window membrane, and they reported greater differences at 4000 Hz than at 500, 1000, or 2000 Hz in 145 patients with unilateral COM. Rosito et al 8 reported greater BC differences between cholesteatoma ears and contralateral normal ears at 2000 and 3000 Hz than at 500 Hz. Levine et al 7 studied 161 patients with unilateral COM and reported that the most affected frequencies were 2000 and 3000 Hz. They also reported statistically significant differences in discrimination scores between diseased and normal ears. In our study, we found significantly greater BC thresholds in ears with cholesteatoma than in normal contralateral ears for each frequency. Although we found greater BC differences at 4000 Hz, there were no significant differences between frequencies. Similar to Levine et al, 7 we found lower discrimination scores in cholesteatoma ears than in normal contralateral ears.
The relationship between cholesteatoma and SNHL has been analyzed in previous studies, with controversial results. Some have found an association between the two, 1,10 -12 whereas others have not observed any difference between COM with or without cholesteatoma and the development of SNHL. 7,9,13,15 Although our study included only patients with cholesteatoma, we found that 31.5%, 34%, 39.7%, and 47.2% of the patients had differences greater than 10 dB at 500, 1000, 2000, and 4000 Hz, respectively, and that 15.6%, 13.1%, 11.9%, and 17.5% of the patients had differences greater than 20 dB. In the study by Levine et al, 7 45% of the patients had differences greater than 10 dB and 20% had differences greater than 20 dB at 2000 and 3000 Hz. In our study, 31.4% of the patients (n = 50) had BC thresholds of 25 dB or lower for at least one frequency in ears with cholesteatoma and had values of 15 dB or greater at all frequencies in contralateral ears. Based on these data, we concluded that one of 3 patients with cholesteatoma developed SNHL in our study, for an incidence rate of 31.4%.
Although we excluded patients with known ototoxic drug use, we could not exclude patients who used topical antibiotics. The use of ear drops is a common practice in patients with COM, and all of the patients made use of them, at some point, to control otorrhea. In fact, topical drops may rarely cause SNHL, and their ototoxic effects are still controversial. 17
To the best of our knowledge, no previous study has investigated the relationship between localization of cholesteatoma and SNHL. In our study, we found that BC differences were significantly higher in advanced cholesteatoma cases in which the tympanic cavity and all mastoid cells were affected by cholesteatoma. Cholesteatoma may cause mechanical obstruction of the round window, changing the resonance frequency of the middle ear and ossicular chain and elevating the BC thresholds with a Carhart-like effect. 3 -6 In addition, BC differences may be higher in cases of long disease duration because the round window membrane is exposed to toxins and inflammatory mediators released from the cholesteatoma matrix for a longer period of time. We believe that these 2 hypotheses may explain the high BC differences in advanced cholesteatoma cases, but in our opinion, further studies are needed on this subject.
Noordzij et al 15 studied 69 patients with unilateral COM and found no association between SNHL and ossicular chain erosion. Similarly, MacAndie and O’Reilly 13 reported that they did not find an association between ossicular chain erosion and SNHL. In our study, no significant relationship was found between the condition of the stapes and BC differences at any frequency.
In this study, an LSCC fistula was detected in 12 (7.5%) patients, who had significantly greater BC differences at 4000 Hz. These findings are in line with Rosito et al, 8 who reported 6% of patients with an LSCC fistula, and a significant association between SNHL and the presence of an LSCC fistula. Unlike our findings, Jesic et al 14 reported that they did not find a significant association between presence of an LSCC fistula and SNHL. In our opinion, an LSCC fistula is one of several mechanisms by which a cholesteatoma can damage the inner ear, and the association with SNHL needs to be investigated in a larger series of cases in future studies.
Luntz et al 11 studied 317 patients with unilateral COM and found no significant correlation between the ABG and BC thresholds in affected ears. Rosito et al 8 studied 115 unilateral cholesteatoma patients and reported that SNHL increased as the ABG increased in ears with cholesteatoma. Our study also supports this finding; as ABG increased in ears with cholesteatoma, the BC differences at each frequency also significantly increased. Because BC differences are also high in advanced cholesteatoma cases, high ABG values may be a warning for clinicians in terms of advanced cholesteatoma.
The main limitation of our study may be the lack of disease duration data. If we could establish the relationship between disease duration and SNHL, we could obtain more information about the course of the disease in terms of SNHL. Another limitation is that we studied patients with unilateral COM with cholesteatoma, and hearing levels were compared to normal contralateral ears. Our patients could be compared to patients with COM without cholesteatoma. However, it is difficult to create similar groups; therefore, we preferred patients’ healthy ears as controls.
Our results showed a statistically significant relationship between cholesteatoma and SNHL. Patients with advanced cholesteatoma had significantly higher levels of SNHL.
In patients with an LSCC fistula, SNHL was significantly higher at 4000 Hz. As the ABG increased in ears with cholesteatoma, the differences between BC thresholds increased significantly.
These findings reveal that patients should be told that patients with more advanced disease have worse SNHL. Therefore, cholesteatoma should be treated as soon as possible before it becomes more advanced. It is important for otorhinolaryngologists to tell patients about cholesteatoma surgery and the complications that may develop if cholesteatoma is left untreated. Our study clearly shows that SNHL is one of these complications. In addition, it may be helpful for otorhinolaryngologists to know that if BC is down at 4000 Hz and this could raise suspicion of an LSCC fistula.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.