
Abstract

A 25-year-old man visited our department with a growing tumor over left-sided external auditory canal (EAC) for several years. On physical examination, a firm, painless, and hyperpigmented nodule about 5 mm was located on the cartilaginous part EAC (Figure 1). High-resolution computed tomography of the temporal bone demonstrated a 7 mm × 5 mm × 3 mm nodule in the anterosuperior over outside the left EAC (Figure 2). The tumor was excised completely under local anesthesia, and the pathologic results showed pictures compatible with dermatofibroma (Figure 3). Immunohistochemical staining with CD34, S-100 protein, and smooth muscle actin was negative.

On physical examinations, a firm, painless, and hyperpigmented nodule about 0.5 cm on the cartilaginous part of external ear canal (arrow).
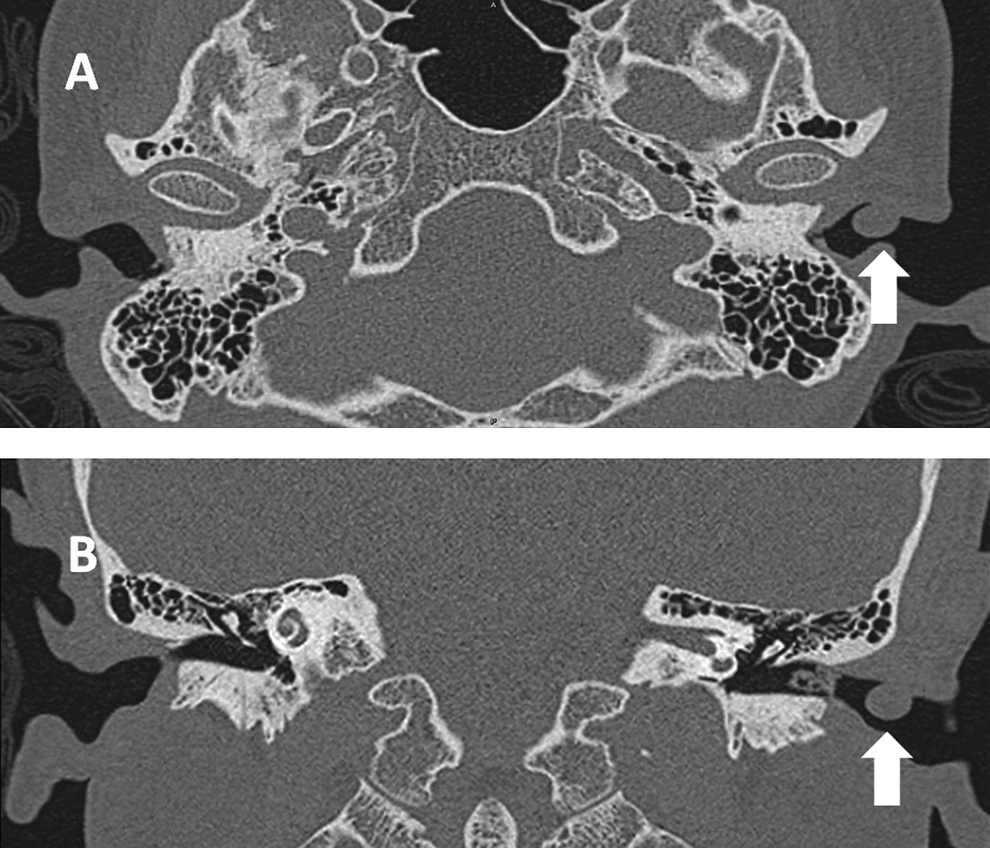
Axial view (A) and coronal view (B) of HRCT of the temporal bone demonstrated a 7 mm × 5 mm × 3 mm nodule in the left external auditory canal (arrows). HRCT indicates high-resolution computed tomography.
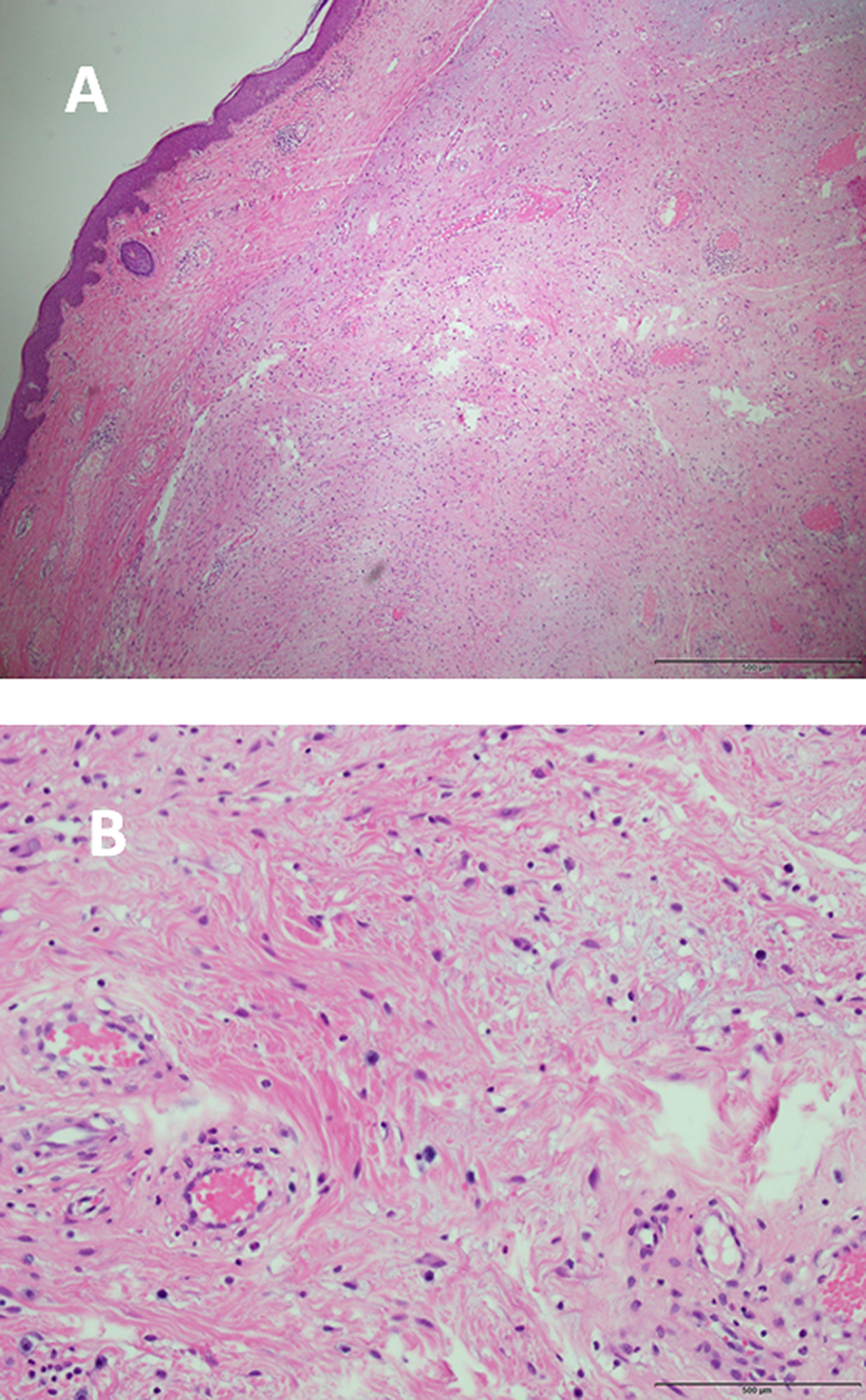
A, The tumor was completely removed (H&E, 40e magnification). B, Microscopically, the specimen showed entrapment of collagen and the storiform growth pattern of spindle-shaped and polygonal histiocytoid tumor cells with myxoid change of the soft tissue (H&E, 200e magnification). H&E indicates hematoxylin and eosin.
Dermatofibroma, also known as benign fibrous histiocytoma, is a common benign tumor, typically found on extremities with prevalence at middle age and female predominance. 1 The etiology of dermatofibroma is not clear, but most of them are associated with previous skin trauma, irritation, or insect bite. 2 The tumor is rarely reported on head and neck region, and only few cases have been reported in the EAC. 3 The differential diagnosis includes nonspecific nodular lesions, melanocytic nevus, epidermal cyst, fibroma, keloid, angioma, and some of malignancy such as dermatofibrosarcoma protuberans. 3,4 Dermatofibroma presents as slow-growing, painless, and hard nodule or papule associated with low rate of recurrence after local excision. However, some case series indicated that the tumor located at uncommon sites such as the face or ear has more aggressive behavior including increased nuclei mitotic rate, deeper extension of soft tissue, and cellular atypia than those at common sites. 2,3 Tumor metastasis was rarely reported, and immunohistochemical staining especially with negative CD34 may help physicians to distinguish dermatofibroma from dermatofibrosarcoma protuberans if tumors present with untypical histology or clinical manifestation. 3 Although dermatofibroma is usually considered to have good prognosis, wide excision is necessary especially when the tumor involved the head and neck region or recurrence. 2,3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-C108-037 to H.C. Chen).