
Abstract
Lymphangioma (LM) is a rare but benign tumor derived from lymphatic malformation, which is extremely rare in the auditory canal or middle ear cavity. We presented a case of acquired lymphangioma of the external auditory canal combined with cholesteatoma in the middle ear cavity. To our best knowledge, this is the first case of combined lesions of lymphangioma and cholesteatoma in English literature.
Introduction
Lymphangioma (LM) is a rare but benign tumor resulting from lymphatic malformation, and the symptoms depend on the mass effect. On the other hand, cholesteatoma is a non-malignant but destructive epithelial lesion that may cause erosion of the adjacent bony structures and various complications. The treatment options for these two diseases are different. For lymphangioma, function-sparing management is adopted, while a complete resection is the main therapy choice of cholesteatoma. Therefore, if a patient had these two diseases simultaneously, it may cause a dilemma in the treatment. Here, we presented a young female having an external auditory canal lymphangioma concurrently with a middle ear cholesteatoma.
Case Presentation
This 27-year-old female, who denied any systemic disease, came to our ENT clinic for the first time with the chief complaint of left hearing loss with bloody discharge for one year. She also complained of left aural fullness with block sensation, but she denied tinnitus, otalgia, vertigo, facial numbness or palsy, or recent body weight change. She ever visited a local medical doctor for help, and a mass lesion in the left external auditory canal (EAC) was suspected. In our out-patient clinic, ENT local finding revealed a reddish tumor in her left EAC with nearly total obliteration of the left eardrum. High-resolution CT of the temporal bone was arranged, which showed a soft tissue density lesion in the EAC and middle ear cavity of Prussak’s space with bone erosion of the left incudostapedial joint and dislocation of the left incudomalleolar joint. Tympanic membrane was involved, and the lesion spread to the tympanic cavity and posterolateral through aditus ad antrum into mastoid antrum. We prescribed ofloxacin eardrop first and suggested further examinations. However, the patient got pregnant, so she postponed the survey and treatment for about one year.
After delivery of a healthy full-term baby, she came back to our clinic one year later, complaining of persistent symptoms. An MRI of the temporal bone was arranged for further evaluation. The MRI demonstrated cloudiness of the left mastoid cells and a poorly enhanced lesion in the left orifice of EAC, about 1.1 × 0.7 × 0.7 cm, with high T1W and T2W signals (Figure 1A and B). Left EAC hemangioma was suspected, so we suggested surgery for tissue proof. The patient underwent endoscopic excision of the mass through a left trans-canal approach (Figure 1C and D). During the operation, we found about 90% perforation of the left eardrum and profuse granulation tissue in the middle ear cavity, including the antrum, epitympanum, mesotympanum, and hypotympanum region. The whole ossicular chain was surrounded by the granulation tissue with fixed ossicular motility. We removed the left EAC tumor with en bloc resection and took out the middle ear granulation while preserving the facial nerve and chorda tympani nerve. (A) A poorly enhanced lesion in the left orifice of the EAC, about 1.1 × 0.7 × 0.7 cm in size; (B) opacification of the left EAC with high T1W, T2W lesions; (C) the gross EAC tumor under the otoscopy during the operation; (D) the keratinized and granulated tissue in the middle ear cavity. Abbreviation: EAC, external auditory canal.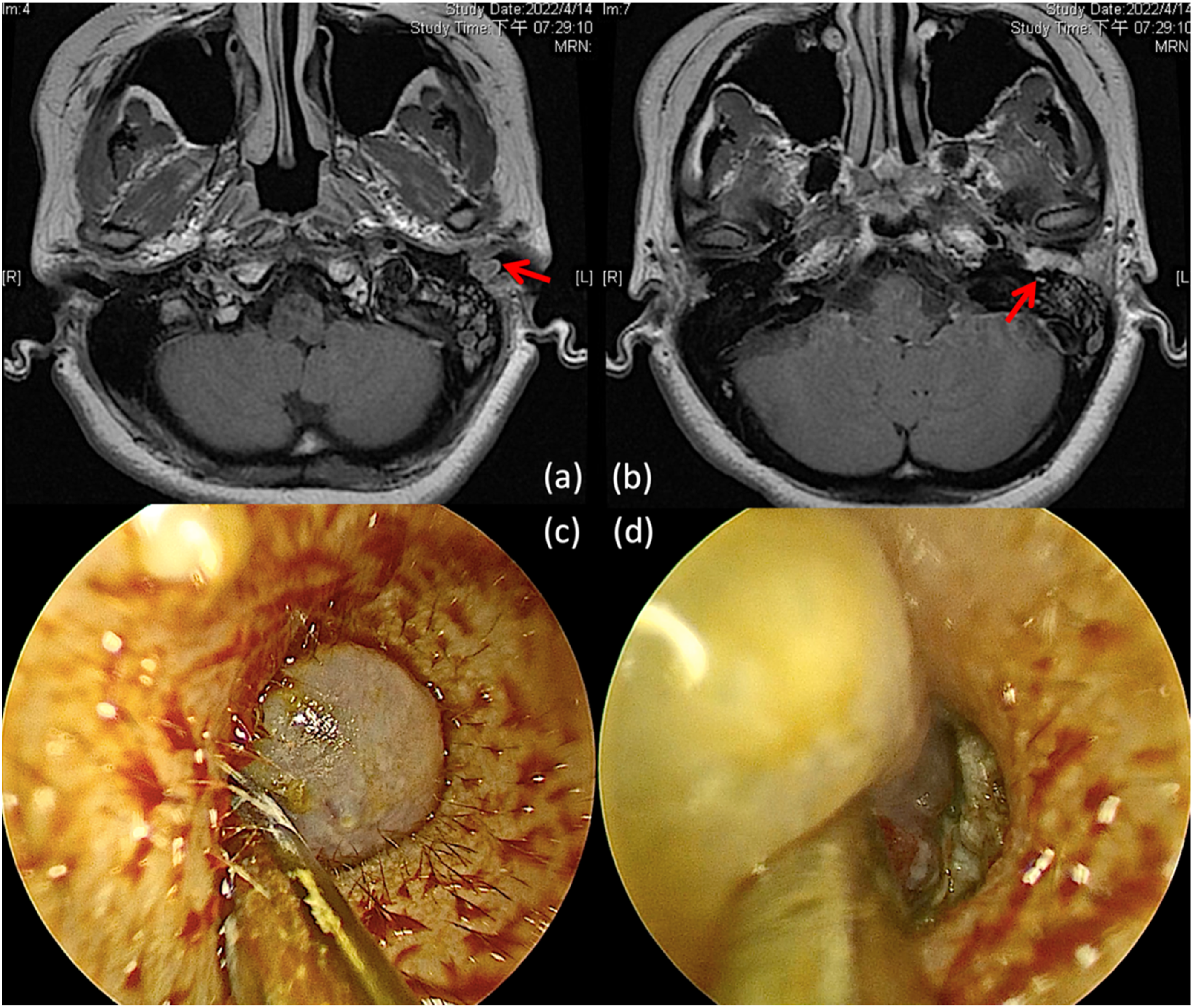
Pathological examination of the left EAC tumor revealed squamous epithelial tissue with dilated channels containing eosinophilic proteinaceous material in the underlying stroma. Immunohistological study showed positive CD31 and D2-40 staining in the flat lining cells of the channels, confirming their lymphatic nature (Figure 2A, C, and D). A diagnosis of lymphangioma circumscriptum was rendered. To our surprise, the specimen of the middle ear part showed a different result—cholesteatoma, based on the presence of fragments of keratinized stratified squamous epithelial tissue, keratin flakes, and fibrous tissue with inflammatory cell infiltration (Figure 2B). (A) Microscopically, the specimen of the external auditory canal tumor showed a stratified squamous epithelial tissue with dilated channels containing eosinophilic proteinaceous material in the underlying stroma. (B) The specimen of the middle ear lesion showed keratinized stratified squamous epithelial tissue, keratin flakes, and fibrous tissue with inflammatory cell infiltration. The lining cells of the dilated channels in (A) were positive for CD31 (C) and D2-40 (D).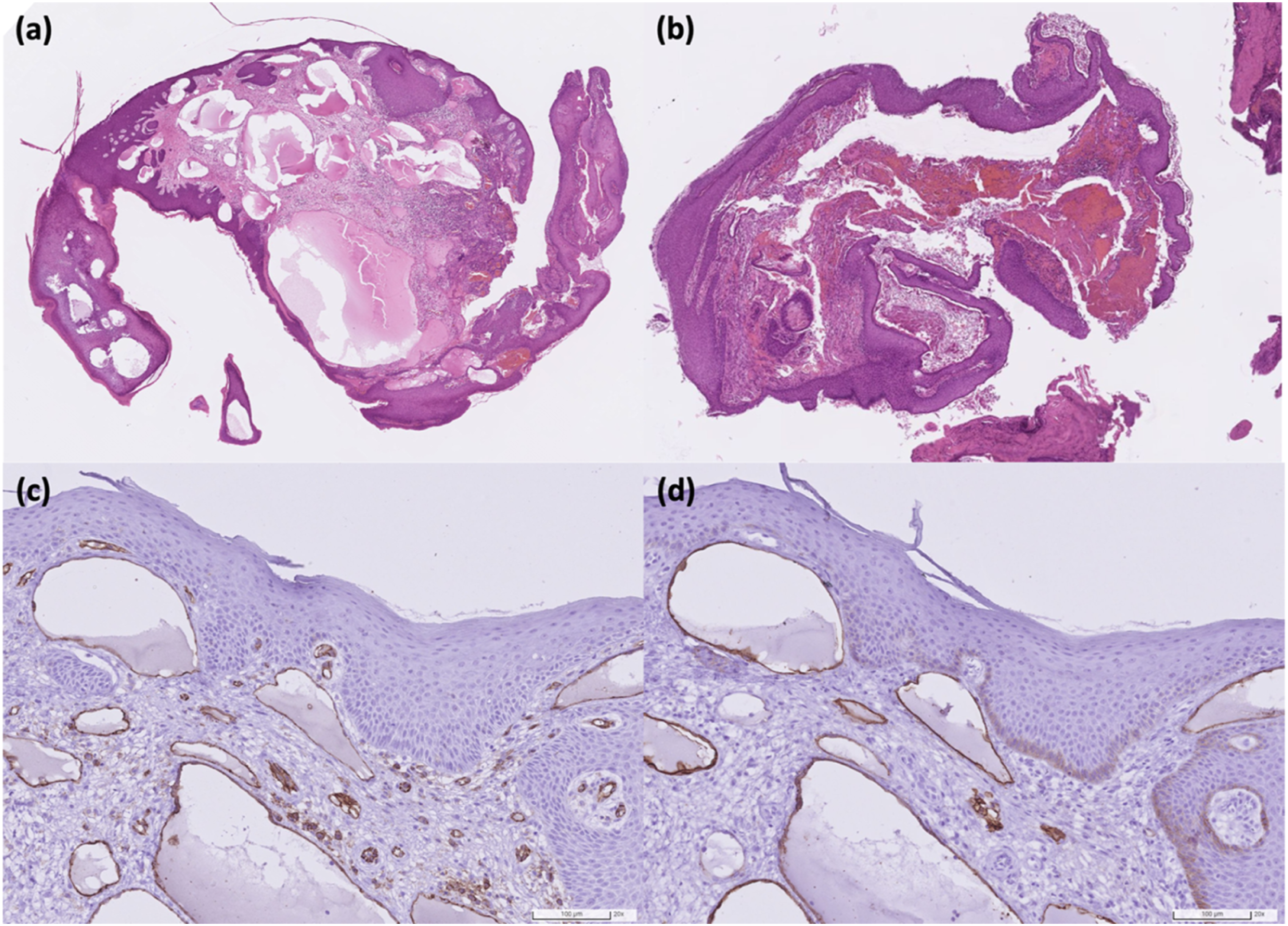
The patient had no postoperative complications, including facial nerve palsy, imbalance, or total hearing loss. The postoperative pure tone audiometry (PTA) showed mild left hearing improvement. The patient has been regularly followed up for eight months since the resection and continues to demonstrate no eardrum perforation or tumor recurrence.
Discussion
Lymphangioma is a rare but benign tumor derived from lymphatic malformation. 1 Although about 70% of LMs locate in the head and neck, they are more commonly seen in the cervicofacial area.1,2 Lymphangioma in the auditory canal or middle ear cavity is extremely rare, with only several case reports published.3 -7 Most LMs are congenital lesions resulting from abnormality of the lymphatic system, 2 and about 95% of the congenital LMs are present within two years after birth.1,8 By contrast, the risk factors of the acquired LMs included trauma, infection, iatrogenesis, neoplasm, or other causes of chronic lymphatic compression.2,4
There are several systems for classifying lymphangioma, which could be macrocystic, microcystic, or mixed, based on the size bigger or smaller than two centimeters.4,8 On the other hand, the classifications based on the histological differences separated LMs into three types: cystic, capillary, and cavernous.1,4 Lymphangioma circumscriptum, as the diagnosis of our case, belongs to the capillary LM, which consists of thin-wall, vascular channels resembling capillaries, appearing as small vesicles protruding into the epidermis. It can also present as dilated lymphatics containing lymph or blood cells, while the surrounding stoma shows scattered lymphocytes. 9 The top differential diagnosis is hemangioma, which shares similar characteristics in images and histology. Immunohistological study plays a vital role in distinguishing these two entities. CD31 and CD34 are the biomarkers of the endothelial cells, which would be positive in the endothelium of both lymphangioma and hemangioma, while D2-40 is a reliable marker specific for lymphatic endothelium.1,6,7
The clinical manifestations of LMs usually derive from the mass effect, like aural fullness and otorrhea, due to an LM in the EAC. 6 Patients may suffer from more severe symptoms if the LMs locate in the middle ear cavity, which hearing loss, tinnitus, and even facial palsy have all been reported.3,4,7 In our case, the patient complained of hearing loss, aural fullness, and bloody otorrhea, while the CT revealed a soft tissue density lesion in EAC and middle ear cavity. At first, we thought it was a single lesion occupying both the EAC and middle ear cavity, but the final pathology showed two different results: lymphangioma circumscriptum of the EAC and cholesteatoma of the middle ear cavity. To our best knowledge, there was no previous English report of such combined presence of lymphangioma and cholesteatoma.
Cholesteatoma is a benign but destructive epithelial lesion that may cause the erosion of adjacent bony structures and various complications. The invasion of the ossicular chain and bony labyrinth may result in hearing loss, vestibular dysfunction, facial paralysis, and intracranial complications.10,11 It could be congenital or acquired, while the latter may result from tympanic membrane trauma or inflammation of the middle ear cavity. 11 The trauma to the tympanic membrane, including perforations, displacements, or retractions, would cause the migration of the epidermal layers of the tympanic membrane, resulting in a pre-cholesteatoma condition. Furthermore, prolonged or chronic inflammation would cause epidermal hyperplasia or metaplasia of the mucosal epithelial cells into keratinizing squamous epithelium.10 -12
The patient did not suffer from these aural symptoms until her adulthood, so both the EAC and middle ear lesion were supposed to be acquired. Though we could not trace the exact cause of the LM, we thought the cholesteatoma might result from the EAC LM. The lymphangioma occupied the whole EAC and caused the retraction of the tympanic membrane, leading to epidermal metaplasia in the middle ear cavity. Furthermore, our patient delayed the treatment for about one year due to her pregnancy. The prolonged status of negative pressure in the middle ear cavity may foster the growth of cholesteatoma and cause extensive invasion of the middle ear structures.
The treatment options for LMs include observation, aspiration, injection, cryotherapy, electrocautery, radiation, laser, ligation, and excision.13,14 There is no consensus on the best management so far, while the location of LMs, age of onset, growth rate, histological type, depth, extent, potential deformity, or dysfunction should all be considered. Since LM is benign, preservation of organ functions is the priority when treatment is implemented. Interventions for LMs in the head and neck regions carry potential complications, including facial nerve damage, Horner’s syndrome, postoperative lymphatic leakage, seroma, and poor wound healing. 14 On the other hand, the mainstay treatment of cholesteatoma is operation, which aims for total removal of the lesion. Surgical approaches include canal wall down (CWD), canal wall up (CWU), endoscopic, and staged procedures. CWD procedures and CWU with second-look procedures have lower rates of residual disease or recurrence. 15 For our patient, we only adopted the endoscopic approach for tumor excision since we did not foresee the presence of a cholesteatoma. Therefore, a second-look operation may be necessary in the future for a more thorough clearance of the cholesteatoma.
To our best knowledge, this is the first report in English literature about the combined disease of lymphangioma and cholesteatoma. Since these two lesions share some aural symptoms, the differential diagnosis could be challenging, and a thorough survey is necessary. As for the management, we need a multidisciplinary consideration to achieve the balance of a disease-free status and the preservation of function.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the medical ethical and human clinical trial committees of Chang Gung Memorial Hospital (ref. 202201798B0, December 02, 2022).
Informed Consent
Patient consent was waived due to the retrospective nature of the work. All patient identification information has been removed from the final report.
Disclosure
We confirm that this work is original and has not been published elsewhere. All authors have reviewed and agreed to co-author the submitted paper. None of the authors have published, posted, or submitted any related papers from the same study.