
Abstract
Sialendoscopy has emerged as a safe, effective and minimally invasive technique for management of obstructive and inflammatory salivary gland disease. The aim of our study was to analyze outcomes of sialendoscopy and steroid irrigation in patients with sialadenitis without sialoliths. We performed a retrospective analysis of patients who underwent interventional sialendoscopy with steroid irrigation from 2013 to 2016, for the treatment of sialadenitis without sialolithiasis. Twenty-two patients underwent interventional sialendoscopy with ductal dilation and steroid irrigation for the treatment of sialadenitis without any evidence of sialolithiasis. Conservative measures had failed in all. Eleven patients had symptoms arising from the parotid gland, 4 patients had symptoms arising from the submandibular gland, while 6 patients had symptoms in both parotid and submandibular glands. One patient complained of only xerostomia without glandular symptoms. The mean age of the study group which included 1 male and 21 females was 44.6 years (range: 3-86 years). Four patients had autoimmune disease, while 7 patients had a history of radioactive iodine therapy. No identifiable cause for sialadenitis was found in the remaining 11 patients. The mean follow-up period was 378.9 days (range: 16-1143 days). All patients underwent sialendoscopy with ductal dilation and steroid irrigation. Twelve patients showed a complete response and 9 patients had a partial response, while 1 patient reported no response. Only 3 patients required repeat sialendoscopy. The combination of sialendoscopy with ductal dilation and steroid irrigation is a safe and effective treatment option for patients with sialadenitis without sialoliths refractory to conservative measures. Prospective studies with a larger case series are needed to establish its role as a definitive treatment option.
Introduction
Chronic sialadenitis may be caused by sialoliths, mucous plugs, ducal stenosis, kinking, infections, immune-mediated or autoimmune disease, radioiodine therapy, radiotherapy and, rarely, and ductal compression by a tumor. 1 The symptoms include recurrent or persistent glandular swelling, pain, dry mouth, sour or foul taste, fever, and associated weight loss from less nutritional intake. The conventional conservative treatment options for chronic, recurrent sialadenitis without stones, include adequate hydration, warm compresses, gland massage, sialogogues, systemic steroids, and cholinergic medications. 2 Simple intraductal saline irrigation has also been shown to reduce the episodes of gland inflammation irrespective of the cause. 3 Sialadenectomy is considered a last resort only after conservative measures have failed, owing to its well-known neurological, cosmetic and functional complications. 4
Sialendoscopy was first documented more than 2 decades ago, for removal of salivary calculi, 5,6 and is presently considered a minimally invasive alternative for the diagnosis and treatment of various nonneoplastic salivary gland disorders.
The aim of this study was to evaluate the effectiveness of interventional sialendoscopy combined with duct dilation and intraductal steroid irrigations in patients with sialadenitis without sialadenitis.
Materials and Methods
Study Design and Patient Population
We performed a retrospective analysis of patients with sialadenitis without sialoliths who underwent interventional sialendoscopy combined with ductal dilation and steroid irrigation at Louisiana State University of Health Sciences, Shreveport, from 2013 to 2016.
Patients with any clinical, radiological or sialendoscopic evidence of sialoliths, or any extrinsic compression were excluded from the study.
Demographic and clinical data were collected on all patients, including age, gender, indication, comorbidities, etiological factors, glands involved, intraoperative findings, and patient response. Data were collected from the electronic records system and also by telephone interviews for patients who did not present to the clinic for follow-up. We evaluated patient satisfaction by means of a 0–10 visual analogue scale (in which 0 = no subjective improvement and 10 = maximal subjective improvement). Response was defined as complete if the score was 10, partial if the score between 1 and 9, and no response if the score was 0.
Technique
Sialendoscopy was performed in the operating room under general anesthesia. The duct opening was dilated with a ductal probe, and mucous plugs and debris were flushed out with irrigation. At the end of the procedure, the ductal system was irrigated with a diluted solution of triamcinolone acetonide (1 mL of 40 mg/mL Kenalog-40 in 5 mL of saline). The procedure was considered technically successful if the duct could be cannulated and the ductal system could be irrigated with steroid solution. Patients were asked not to suck on lemon drops for a week after the procedure so as to retain the steroids that were instilled into the duct and gland.
Results
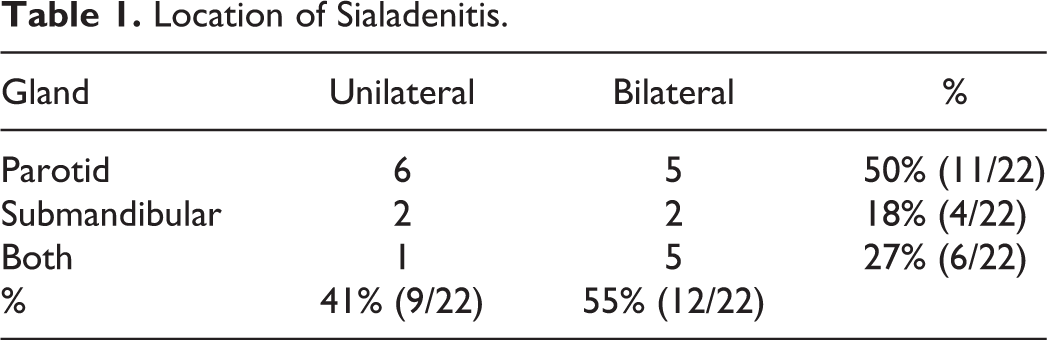
Twenty-three patients underwent interventional sialendoscopy with intraductal steroid irrigation for the treatment of sialadenitis without any previous evidence of sialolithiasis, between 2013 and 2016. Conservative measures had failed in all. One patient was found to have a calculus during the procedure and was hence excluded from the study. The median age of the study group which included 1 male and 21 females was 45.5 years (range: 3-86 years). Symptoms involving only the parotid gland were more common (50%) than isolated submandibular gland involvement (18%), with both glands involved in 27% of patients (6/22). One patient complained of only xerostomia without glandular symptoms. Symptoms were unilateral in 9 patients and bilateral in 12 patients (Table 1). Six patients had laboratory confirmed autoimmune disease and 7 patients had a history of receiving radioactive iodine therapy in the past, while the remaining 9 patients had recurrent sine causa sialadenitis.
Location of Sialadenitis.
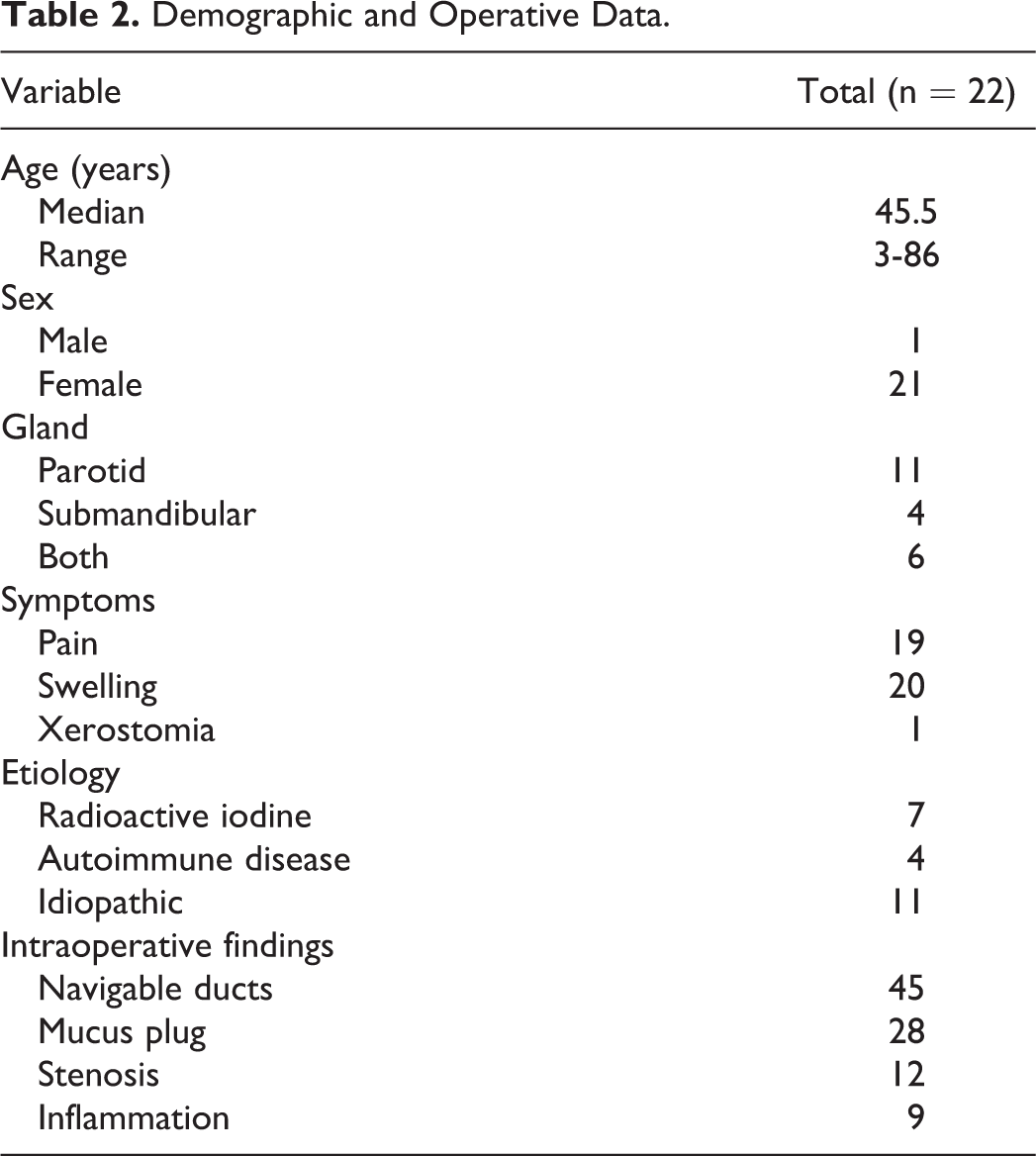
A total of 48 glands were explored in these 22 patients. Sialendoscopy was successfully completed in 84.2% (16/19) of submandibular glands and 100% (29/29) of parotid glands, with an overall technical success rate of 93.8%. Intraoperative findings included presence of inflammation, mucus plugs, and/or stenosis (Table 2).
Demographic and Operative Data.
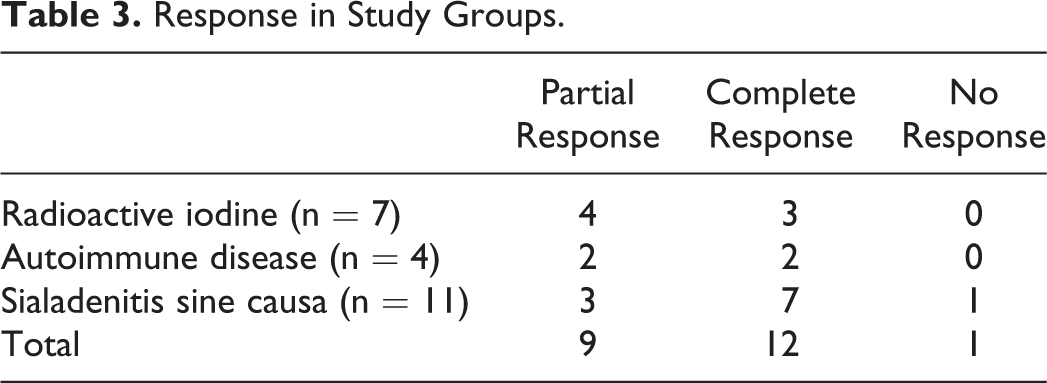
Subjective symptomatic improvement was noted in all but 1 patient after the procedure, with a complete response seen in 12 patients and a partial response in 9 patients (Table 3). Three patients with an initial response to treatment underwent repeat sialendoscopy with steroid irrigation at a later date for recurrence of symptoms. The time interval between the procedures ranged from 392 days to 672 days. The one patient who had no symptomatic improvement declined further treatment. All patients had postoperative pain and swelling of the glands, which resolved within 48 hours. There were no intra- or postprocedural complications noted. The mean follow-up period was 378.9 days (range: 16-1143 days).
Response in Study Groups.
Discussion
Traditional treatment of chronic sialadenitis comprises of either conservative therapy or sialadenectomy, the latter known for its neurological, cosmetic, and functional sequelae. 4
Sialendoscopy has revolutionized the management protocol of nonneoplastic diseases of the salivary glands and is now an accepted modality of treatment for chronic and recurrent sialadenitis. The benefits of sialendoscopy in these patients is likely due to mechanical dilation of the ductal papilla as well as the ductal system and removal of mucus plugs and debris with the irrigation. Steroid irrigation may add therapeutic benefit by reducing the periductal inflammatory activity and prevention of further scarring.
The etiology of sialadenitis in our patient population included recurrent sialadenitis sine causa (11/22), radioactive iodine therapy (7/22), and autoimmune disorders (4/22). All the 7 patients who had a history of radioactive iodine treatment had either partial (4/7) or complete (3/7) response to treatment. One patient underwent a repeat intervention after 1 year, with complete response. Our response rate of 100% is consistent with previously published data, which reports success rates from 50% to 100%.
Bomeli et al published a retrospective study of 12 patients with radioiodine-induced sialadenitis treated with interventional sialendoscopy, reporting a success rate of 75%. 7
Kim et al evaluated 10 patients treated with Radioactive Iodine treatment, with subjective symptom scores, salivary flow rate, and salivary gland scintigraphy prior to treatment and 3 months after sialendoscopy. 8 They found that postoperative obstructive symptoms were significantly improved without significant change in xerostomia-related symptoms, salivary flow rates, or scintigraphy functional results.
Our study included 4 patients with laboratory-confirmed autoimmune disease, out of which 2 patients showed a complete response to treatment and the remaining 2 showed a partial response. Shacham et al studied 10 patients with autoimmune disease related sialadenitis and reported their experience with sialendoscopy, ductal dilation, and steroid irrigation. 9 They reported that on sialoendoscopy, the major cause of recurrent sialadenitis in patients with autoimmune diseases was stricture formation, and hence, locating the stricture under direct vision, dilating the duct, and thoroughly rinsing the gland with steroids resulted in immediate symptomatic improvement. They reported no recurrence in symptoms, on a follow-up ranging from 5 months to 2.5 years. Adding steroid to the irrigation may be responsible for local disease control and preventing recurrence of symptoms and hence may add to the therapeutic value of interventional sialendoscopy by reducing the systemic steroid requirement and its major side effects.
In a prospective cross-sectional study elucidating the role of intraductal steroid therapy in patients with recurrent sine causa sialadenitis, Capaccio et al found that the addition of intraductal steroid irrigations increases the medium-term outcome of interventional sialendoscopy. 10
Of the 11 patients with recurrent sine causa sialadenitis in our study, only 1 patient showed no clinical improvement after treatment. This was the only failure in our study, which can be attributed to failed endoscopic access of the concerned gland. One patient with a complete response posttreatment had recurrence of symptoms after 6 months and underwent repeat sialendoscopy.
The limitations of our study are small numbers, heterogeneous patient population, and its retrospective design. The small number of patients and the heterogeneous patient population prevent us from making strong associations between the intervention and its effect. Also errors due to confounding variables and bias are more commonly seen in a retrospective study. Nonetheless, our study adds to the growing pool of data that endorse sialendoscopy with intraductal steroid irrigation as an improved treatment modality for sialadenitis without sialolithiasis. Prospective studies comparing saline irrigation with steroid irrigation during sialendoscopy will be required to further validate its specific therapeutic value.
Conclusion
Interventional sialendoscopy is a safe and effective treatment option for sialadenitis without sialoliths. It provides immediate symptomatic response attributed to the removal of mucus plugs and dilation of strictures. Combining the procedure with steroid irrigations may increase its therapeutic value due to the localized anti-inflammatory action of steroids. Further randomized studies are required to solidify these conclusions.
Footnotes
Authors’ Note
This article has been presented as a poster at the Triological Society 2018 Combined Sections Meeting held at Scottsdale, Arizona, USA from January 18, 2018, to January 20, 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.